
Abstract
Background and Purpose:
This study investigated the factor structure of an instrument to measure attitudes and beliefs of how physical therapist (PT) practitioners perceive working with people with a dementia disorder.
Methods:
A survey was mailed to every skilled nursing facility in Indiana (n = 495) for completion by a PT or physical therapist assistant. The survey was developed and included whether the severity of Alzheimer’s disease (AD) impacts the attitudes of physical therapy practitioners.
Results:
Of the 12 attitudinal questions, 11 were significant (P < .001) concerning how the severity of a diagnosis of AD (early, middle, and late) impacts attitudes of people in physical therapy practice. Principal component analysis identified 3 factors with Eigen values of 3.3 or higher accounting for 43% of the cumulative variance. These factors include professional competence, resources, and conscientiousness.
Conclusion:
This brief instrument could serve as an assessment tool to determine whether PT practitioners exhibit therapeutic nihilism when working with people with a dementia disorder.
Introduction
The percentage of the elderly individuals with a dementia disorder is increasing rapidly. Dementia disorders, in order of prevalence, include Alzheimer’s disease (AD), vascular dementia, dementia with Lewy bodies, mixed dementia, Parkinson’s disease, frontotemporal lobar degeneration, Creutzfeldt-Jakob disease, and normal pressure hydrocephalus. 1 The emerging reality is that health care providers face significant challenges, and abilities are strained in providing optimal care to this population. Currently, almost 13% of the US population is over the age of 65, and projections put that percentage to 19.6% by 2030 and 20.7% in 2050. 2 The current estimate is that 5% of the population over 65, and 15% to 25% of the population over 85 totaling approximately 5.4 million Americans have been diagnosed with AD. 2 Corrada et al 3 has estimated that the incidence of dementia doubles every 5 years after age 90. Increases in the elderly population presenting with such a debilitating disease will undoubtedly cause an increased demand for geriatric services. Nearly half of all nursing home residents are diagnosed with AD or dementia, and 75% of these individuals will be admitted to a nursing home by age 80, as compared to only 4% of the general population. 1 No known medical treatment effectively delays or stops the destruction of brain cells in this disease. If effective preventative measures or treatment methods are not discovered, projections indicate that by the year 2030 there will be approximately 7.7 million Americans diagnosed with AD, and by 2050 the number of Americans diagnosed could reach 16 million. 2
Ajzen and Fishbein’s 4 Theory of Reasoned Action suggests that attitudes influence an individual’s intention toward behavior. People with positive attitudes toward a specific person or object are more likely to have favorable behaviors, beliefs, and feelings toward those specific items. Negative attitudes are precursors to unfavorable behaviors, beliefs, and feelings. Therefore attitudes influenced by beliefs can induce behaviors in specific ways.
As the prevalence of dementia disorders continues to increase, more health professionals will interact with this population. Physical therapists and the physical therapist assistants (PTAs) that they supervise are skilled practitioners in the rehabilitation of people with musculoskeletal and neuromuscular disorders. Physical therapy (PT) providers are in a unique position to assist in the care of these individuals. A recent study found that 43% of the makeup of the caseload of PT practitioners, working in skilled nursing facilities (SNFs), consisted of people with dementia. 5 Understanding the attitudes and beliefs of PT providers would therefore be advantageous to determine whether there are underlying positive or negative assumptions brought to the patient–therapist interaction.
Many authors have researched the attitudes and beliefs of nursing staff, social workers, and health care students when working or preparing to work with patients diagnosed with a dementia disorder. 6 –15 In general, these studies found that more education, training about the disease, and management techniques for the people with dementia needed to be made available to staff. A decision was made to investigate how attitudes might affect the care provided by PT practitioners.
Kane 9 has explored how adequate social workers felt when working with people with AD and found that students and new graduates felt less competent than their counterparts who had been working with that population for many years. Kane 9 emphasized several keys to a positive experience when working with this population including previous exposure, education, influence from current practitioners, and recent experience/employment with people with AD or dementia. The primary component of the negative attitudes found in another Kane study 8 appears to be a lack of understanding of the disease processes. This lack of understanding led to a decreased desire to work with the aging population. The author described this as a lack of competence. An unknown, but equally important question to explore is how experience or education affects this attitude.
Kane 8 used principal component analysis of a survey instrument to identify 3 factors of attitudes and preparedness of social workers to work with the population of elderly with AD. These 3 factors were a general belief in the efficacy of psychotherapeutic services, a self-perceived adequacy to provide these services, and belief in the efficacy of other ancillary services. These 3 factors provided a framework to assess the readiness for social workers to work with this population. Kane’s 8 article also discussed the topic of “therapeutic nihilism” a term first noted by Dunkelman and Dressel 16 which concerns the attitudes of working with elderly individuals with AD. Therapeutic nihilism is a type of ageism where a belief is held that older people are or will become demented as they age. So some care providers to this population may feel that “since memory recovery among the memory impaired is not currently possible there is little point in providing services to this population.” 11 Because of the great amount of effort required to work with a patient population having this progressive disease, the valuable investment of time necessary to provide interventions may be thought to be wasteful, especially considering factors such as total workload, productivity requirements, and reimbursement. These factors were thought to be important in measuring the work environment and hence attitudes in treating this population of patients.
Stress on health care providers is present through the threat of litigation, restrictive reimbursement criteria, the lack of known efficacy for treatments, and the need to provide emotional support for individuals that are injured, impaired, or ill. Specifically, those professionals working with people that have dementia are faced with the reality that no effective means of treatment are currently available to abate the disease process. Alzheimer’s disease and most dementias are progressive disorders that ultimately lead to loss of function, loss of sense of self, and eventually death. In 2 separate studies, Novak and Chappell 17,18 found higher stress levels and more burnout in nursing assistants that cared for cognitively impaired patients. Brodaty et al 19 wrote that working with cognitively impaired people in nursing homes is associated with high levels of stress. The study showed that the nursing staff had a negative attitude to working with patients with dementia because of behavioral issues including lack of cooperation, aggressiveness, and lack of predictability. More negative attitudes toward the patients were associated with less satisfaction at work.
Education can have a positive effect on therapeutic efforts and can positively affect outcomes. Norbergh et al 20 wrote that a positive attitude is important for quality care to occur. A positive caregiver will do the best for a patient with dementia even in the presence of negative behaviors from the patient. These positive attitudes may then promote improved patient health and well-being. Conversely, negative attitudes of beliefs toward patients with dementia might result in avoidance or a decrease in interaction with these patients. This lack of patient interaction could result in an overall decrease in patient health and well-being.
Provider expectations may also have a direct impact on patient outcomes. van Dulmen and Bensing 21 found that physician expectations directly impacted the patient’s health because physicians “in a subtle way transmit those expectations to the patients” and may be “even more determinative for health effects in the patient than the expectancies of the patient” themselves. 21 A negative belief or attitude would undermine the therapeutic relationship between the practitioner and the patient which would limit the success of the intervention strategies.
Different health professions assess people with AD or dementia from different perspectives depending on the discipline-specific training they have received. While education regarding skilled assessment and/or interventions varies among all the professions and among the paraprofessionals, all of the studies found a need for increased education to serve this population. Lusardi and Wong 22 found that physical therapists were lacking in general knowledge regarding people with AD and strongly suggests that academic educators alter their programs to include more experiences with this population. Practitioners who provide services to people with dementia are required to go through a complex decision-making process to provide optimum care for these individuals. Poor decision making can lead to less than optimal care. The professionals working with this population must recognize that there is a specific body of knowledge and skills to master to provide the optimal care to people with dementia. A number of studies have confirmed the influence of clinician attitudes on clinical decision making. 23 –26 The literature has clearly shown that education and attitudes about dementia disorders can influence care.
Methods
Instrument Development
The formulation and development of this survey was designed by the author, a physical therapist and geriatric clinical specialist, and reviewed by selected individuals to refine the content areas and clarity of the questions. To improve face and content validity, and with the intent of progressing to a principal component analysis for construct validity, adjustments were made to the original survey instrument based on comments received from participants following a trial study, and a panel consisting of 2 geriatric clinical specialists, and 2 survey experts before being sent out state-wide.
Following 30 demographic questions, 12 attitudinal questions were asked and subdivided into 3 categories of severity of Alzheimer’s/dementia. The attitudinal portion of the survey asked therapists to rank their attitudes regarding treatment of patients with dementia during the early, mid, and late stages of the disease. Answers were reported in a Likert-type scale for each stage with a ranking from 1 to 5 from strongly agree (1), agree (2), neutral (3), disagree (4), to strongly disagree (5).
For ease of use of the survey instrument, the stages of dementia were classified as early, middle, and late, which were defined on the survey instrument as follows:
Early: loss of short-term memory, decreased judgment, safety concerns, difficulty with mathematical calculations, inability to comprehend abstract ideas.
Middle: difficulty with speech and language (aphasia and anomia), labile personality changes, changes in usual grooming habits, apraxia, urinary incontinence, wandering, hallucinations, paranoia, or depression.
Late: inability to perform activities of daily living; inability to remember how to walk, toilet, eat, or swallow; minimal to no communication, immobility, requires total care.
Procedure
Eligible participants were physical therapists (PTs) or PTAs practicing in an SNF in Indiana. Some SNFs employ PTAs as a less expensive care provider, and the PT may only visit on a part-time basis for evaluation and supervision. As the PTA may be the person directly providing care to this patient population, a decision was made to include both PTs and PTAs in this study. This would also allow researchers to determine whether any differences in attitudes existed between these 2 differently educated groups of care providers. A comprehensive list of all the SNFs located throughout the state of Indiana (n = 495) was compiled, and a survey was mailed to each facility.
Data Analysis
This study used a prospective nonexperimental design. Responses from the surveys were coded and entered into Statistical Package for the Social Sciences 16.0 (SPSS, Chicago, Illinois, 2008). Once completed, the entered data were cross-checked to minimize the possibility of data entry error.
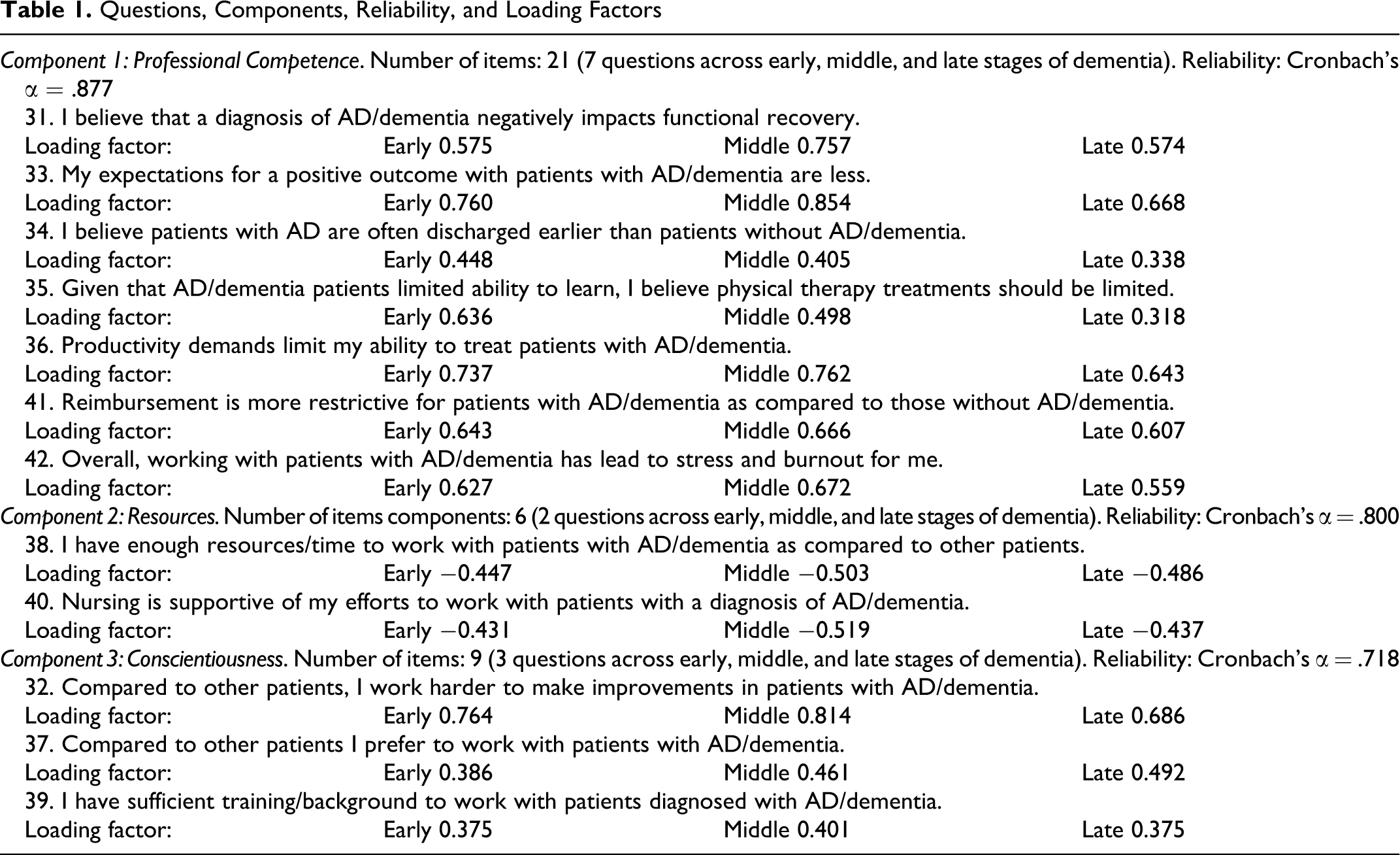
Interferential statistics were run on the attitudinal questions numbered 31 to 42, Table 1 which looked at how the severity of a diagnosis of dementia (staged early, middle, and late) impacted attitudes of physical therapy practice. Construct validity of the instrument was established using an exploratory principal component analysis with varimax rotation. The 36 of interrelated variables were combined into factors representative of conceptual model of therapist attitudes. Each factor was verified for internal consistency using Cronbach’s α. A Kaiser-Meyer-Olkin (KMO) was utilized to determine sampling adequacy.
Questions, Components, Reliability, and Loading Factors
These factors were then analyzed using Friedman’s analysis of variance ([ANOVA] α = .05 for differences in provider attitudes across the 3 stages of dementia). For the significant component factors in which a significant difference was found, the Wilcoxon signed rank test with a Bonferroni adjustment of α was used to compare the attitudes of each stage: early versus middle, middle versus late, and early versus late.
Power analyses at 0.80 were conducted on all the attitudinal components to determine whether the sample size of 93 participants, that answered all of the questions, was sufficient to detect a meaningful difference. To control for α inflation of multiple tests, pairwise comparisons were adjusted to an α of .01 to determine statistical significance. The degree of statistical difference of all pairwise comparisons was documented using Cohen’s d effect size.
Results
Survey Return
Of the 495 potential respondents, 112 (21.6%) were returned. Eight were returned with a statement regarding the inability to complete the survey due to time and productivity constraints. Two were returned without completing the attitudinal questions. Four were returned after the set closure date 90 days after the survey was first sent out and data analysis had commenced. Ninety-three (18.8%) surveys were deemed completed and utilized for data analysis. This number reasonably fits the guidelines for determining minimum returned sample size for a continuous data study to maximize the likelihood of finding a statistical difference. 27 For demographic data see Table 2.
Participant Demographics
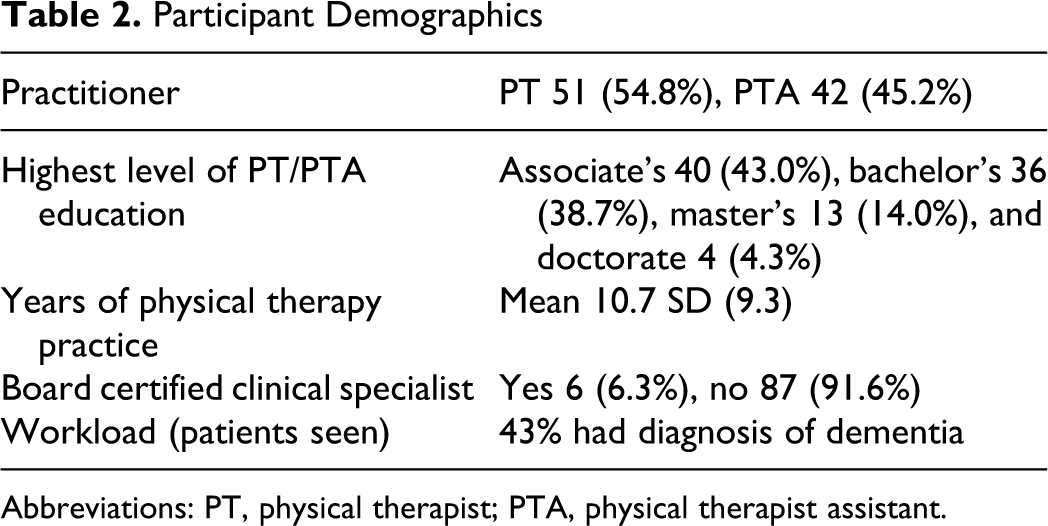
Abbreviations: PT, physical therapist; PTA, physical therapist assistant.
Attitudes and Beliefs
Of the 12 attitudinal questions, 11 (31, 33-42) were statistically significant (P < .0001) concerning how the severity of a diagnosis of AD or dementia (early, middle, and late) impacted the attitudes of PT practice. Of these 11 questions, significant differences between early–middle, middle–late, and early–late were found for each pairwise comparison except for the early–middle comparison for question 41 (P = .0253). The only attitudinal question not found statistically significant (P = .674) was question 32, which asked the participant whether he or she worked harder to make improvements in patients with AD/dementia as compared to other patients. There was no significant difference found between PTs and PTAs for any of the responses to the attitudinal questions.
Principal Component Analysis
The KMO of 0.628 was found which indicated that all the variables were useful and not too multicollinear allowing factor analysis to proceed. Principal component analysis was used to group the 36 survey’s questions into a few meaningful factors representative to practitioner attitude. All 36 questions were included in a 3-factor component model. This result provided clarity in interpretation of the attitudes that PTs/PTAs held about patients with dementia. A scree plot (Figure 1) was examined to find a break point among the component for data reduction. A break point was selected at a 3-factor solution in which all Eigen values had scores of 3.7 or higher. A decision was made to proceed with a principal component analysis of a 3-factor solution. This model had appeal because all 36 questions loaded into 1 of the 3 components, and each component could be interpreted for conceptual sense. With a varimax rotation, the 3-component model accounted for 43.3% of the variation (Table 3).
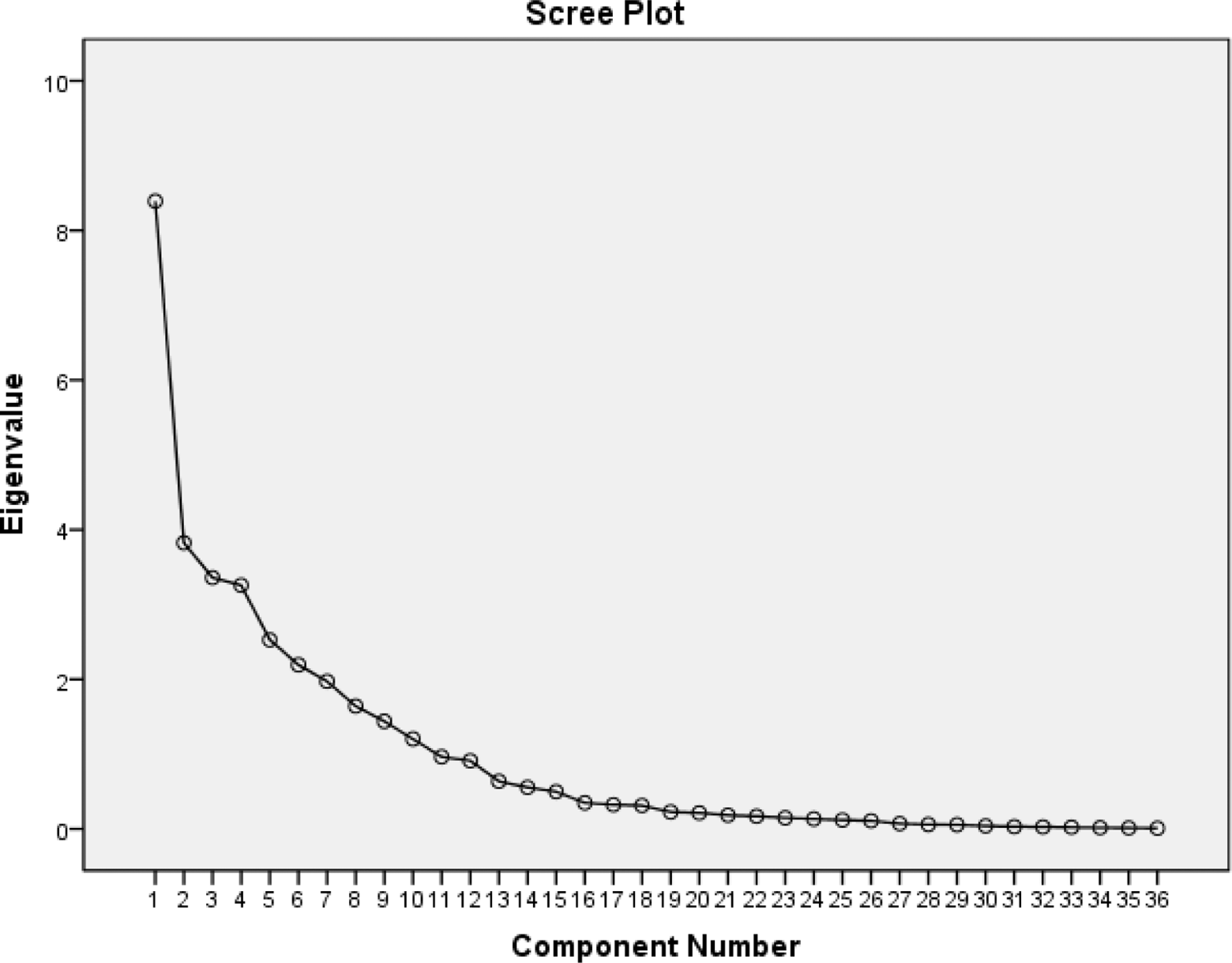
Scree plot.
Total Variance Explained Through Varimax Rotation

To further validate the 3 components, they were analyzed for internal consistency utilizing Cronbach’s α across early, middle, and late stages. Each component had internal consistency and each component was independent of each other through varimax rotation. Component 1 (professional competence) consisted of questions 31, 33, 34, 35, 36, 41, and 42 and had a reliability score of .877 (21 questions). Component 2 (resources) consisted of questions 38 and 40 and had a reliability of .800 (6 questions). The third component (conscientiousness) consisted of questions 32, 37, and 39 and had a reliability of .718 (9 questions). All 36 questions loaded into these 3 components signifying the importance of all of the questions in this framework. The loading factors for each question can be found in Table 1. The reliability for components 1 and 2 is rated as good, and the third component as satisfactory for internal consistency.
Since the data within the 3 constructs were not found to have a normal distribution, a nonparametric Friedman’s ANOVA examined the overall differences between each of the 3 stages of dementia for all 3 components. All 3 components were statistically significant (P < .001) across early, middle, and late stages of dementia. The Wilcoxon signed rank post hoc test with a Bonferroni correction showed significant pairwise differences (P < .01) between early, middle, and late stages of dementia. The effect size of difference was large.
Discussion
The primary purpose of this study was to investigate a factor structure of PT providers regarding beliefs, and attitudes on physical therapy as a treatment approach for patients diagnosed with a dementia disorder residing in SNFs in Indiana. The proposed 36-item instrument contains a 3-factor solution. The 3 factors were named professional competence, resources, and conscientiousness.
The first component questions dealt with the current base knowledge of disease progression, patient management, and self-management on how these effect attitudes and beliefs. This component which contained questions 31, 33, 34, 35, 36, 41, 42 consisted of factors that appear to be either within the therapist's control, or external health care delivery factors affecting the therapist’s ability to perform their job. The authors have called this the professional competence component. The professional competence component involves the therapists current knowledge of disease progression and case management at different levels of the disease. The previous education of the practitioner has direct relationship within this component (questions 31, 33, 34, and 35). Respondents believed that productivity demands (question 36) and more restrictive reimbursement (question 41) limited their ability to self-manage in the treatment of patients in the later stages of dementia. In fact, 8 surveys were returned that indicated that productivity demands were so strict that they would be unable to spend 15 to 20 minutes to actually complete the survey. Several other surveys may have been discarded and not returned for the same reason. The survey tool found an increase in stress and burnout in therapists (question 42) as the patient’s condition worsened. Working as a physical therapist has been found to be a stressful occupation. 28 –30 Treating a patient with dementia can be an additional difficult and stressful task. 31
Ries et al 32 found significant differences in performance in outcome measures from individuals with mild to moderate AD as compared to those with moderately severe to severe AD. As the dementia progressed, Ries 32 was able to show that the performance decline in the outcomes exceeded the decline that would be expected in the normal aging process. Consequently, it stands to reason that working with patients in the later stages of dementia is perceived as more difficult than working with patients in the earlier stages as they have lessened abilities. The literature is clear regarding the influence of knowledge and education on positive attitudes when working with people with dementia. More positive attitude leads to less burnout and may improve care.
The second component looked at resources such as space, equipment, and time allocated on how these affect practitioner attitudes and beliefs. Management constraints and limited assistance from nursing staff appear to negatively affect attitudes needed to properly care for individuals with a dementia disorder. This component consisting of questions 38 and 40 holds together as a concept and was called the resources component because these concepts support the therapist in their role as a clinician. The analysis of the resources component revealed an interesting finding. The respondents actually felt more negative in the earlier stage than the middle and late stages. As dementia progressed to the later stages of the disease, more practitioners did not indicate insufficient training/resources (question 38) to work with this patient population. This may be because the therapists feel they needed more support in the early stages of the disease when they believed more progress could be made than in the later stages where less improvement might be made. This may actually be a more fatalistic belief, or a possible indication of therapeutic nihilism, regarding the course of the disease.
The third component questions appear to be acknowledging the therapist’s self-concern about their job performance. This component contains questions 32, 37, and 39 and is called the conscientiousness. The conscientiousness component included work preference, how hard the therapist works, and whether they feel they have sufficient training to meet the needs of the patients and work with this population. This component revealed some low correlations, but all the 9 questions (3 parts of the 3 questions) contributed to the component. Therapists reportedly felt that working with patients with a dementia disorder was more difficult or “they worked harder” (question 32) and preferred not to work with individuals (question 37) in the later stages of the disease when compared to patients in the earlier stages of the disease process. This is understandable considering that therapists have the same productivity demands and time to treat each patient, no matter the complexity or involvement of each patient. Additionally, the survey found that as the condition worsened, the therapists felt less confident in their training (question 39). Practitioners felt that more training was required in the later stages of the disease. Both the literature and this survey are in agreement that additional training is warranted, and the clinicians should be provided the opportunity to partake in this activity. Further study is needed to determine exact types, how much, and at what stages additional education needs to be provided to therapy providers.
The results of this study indicate the notion that beliefs in PT practice are increasingly more negative or pessimistic when working with patients in the later stages of dementia compared with the earlier stages of dementia. Therapists may have felt that worsening dementia negatively impacted functional recovery and, as a result, they had fewer expectations for a positive outcome and may be exhibiting therapeutic nihilism. This result should not be surprising that therapists prefer to work with patients in the early stages of dementia because it was at this stage in the disease process therapists felt they could be of the most help to the patient. Working with patients in the later stages of dementia appears to make therapists less satisfied than working with patients in the earlier stages of dementia. Treatment became more challenging as the disease progressed and therapists no longer felt treatment sessions were as effective as in the earlier stages of the disease.
Future Research
These 3 components now become a good place to continue research with a more refined tool that may be able to identify the needs of therapists. This new tool may be able to determine what additional education, resources, and support that therapists require in order to optimize their job performance. Further development of this survey instrument to improve internal and construct validity is needed. The instrument should then be distributed to a larger target area for increased sample size and broader national representation. Additional factor analysis should be made comparing the attitudinal responses between different professions. Although the sample frame is limited to SNFs in the state of Indiana, variation across different geographical regions may be negated because of national rules and regulations for institutional care and reimbursement.
Conclusions and Implications
This survey has shown that a significant portion of the therapists’ caseload in an SNF setting consists of patients with dementia, and the therapists surveyed did not feel they have adequate training, resources, or reimbursement to treat these patients as the severity of the disease increased. Beliefs and attitudes of therapy providers were more negative working with patients in the later stages of dementia, perhaps exhibiting therapeutic nihilism, when compared to patients in earlier stages of dementia. The results indicate the instrument is a good initial step toward developing a tool with desirable internal consistency and construct validity that may be able to be used with other health care professionals.
Utilization of therapeutic services for a growing population of people who have or may develop dementia is and will be an integral component of improving the quality of life in those individuals. This research has contributed new knowledge to the interaction between therapists and people with a dementia disorder. This brief instrument could serve as an assessment tool to determine whether practitioners exhibit therapeutic nihilism in work with people with a dementia disorder. The survey could also determine whether additional education and resources minimized the effect of therapeutic nihilism in work with people with dementia. The components of competence, resources, and conscientiousness need to be further investigated to see whether the attitudes and beliefs can be modified to improve care of patients in later stages of dementia.
Footnotes
William H. Staples planned the study, supervised the data analysis, and wrote the article. Clyde B. Killian assisted with statistical analyses and contributed to revising the article.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.