
Abstract
Person-centered, nonpharmacological interventions for managing Alzheimer’s/dementia-related behavioral disturbances have received significant attention. However, such interventions are quite often of a single type limiting their benefits. We develop a comprehensive nonpharmacological intervention, the Behavior-Based Ergonomic Therapy (BBET), which consists of multiple therapies. This low-cost, 24/7 program uses learning, personality, and behavioral profiles and cognitive function of each resident to develop a set of individualized therapies. These therapies are made available through an accessible resource library of music and video items, games and puzzles, and memory props to provide comfort or stimulation depending on an individual resident’s assessment. The quantitative and qualitative benefits of the BBET were evaluated at the dementia care unit in a not-for-profit continuing care retirement community in west central Ohio. The 6-month pilot study reduced falls by 32.5% and markedly reduced agitation through increased resident engagement.
Introduction
Alzheimer’s disease and other forms of dementia are common reasons for admission to assisted living and nursing facilities. Behavioral disturbances associated with dementia are also common and challenging for both staff caregivers and visiting family members. According to our experience, having visited at least 10 long term care facilities, nonpharmacological interventions have been used with varying degrees of success, but are for the most part disappointing.
Cognitive stress can have physiologic or pathophysiologic causes (such as hunger, fatigue, need to toilet, pain, dyspnea, etc) and nonclinical causes (such as boredom, disengagement, or dissatisfaction with the environment). As a consequence, residents may exhibit challenging behaviors for staff, including restlessness, agitation, wandering, shadowing, sundowning, combativeness, and so on. These behaviors impact their own health, confidence, and well-being and increase the stress of caregivers, family members, and other residents in the unit. To avoid the use of physical restraints, methods for treating such behavioral issues have included medications, such as antipsychotics, antidepressants, anticonvulsants, cholinesterase inhibitors, and memantine. The adverse side effects and lack of efficacy of medications have raised interest in nonpharmacological interventions. 1 Although Alzheimer’s disease is a terminal illness, some patients may live up to 20 years with the disease. Providing a good quality of life and preserving meaningful relationships in patients during the course of illness should be essential components of any intervention. 2 Several studies have shown that nonpharmacological interventions can reduce disruptive behaviors in residents with Alzheimer’s disease and improve their quality of life. 3,4 Person-centered, nonpharmacological intervention has received significant attention owing to the limited benefits of group activities. Single-center studies have shown that person-centered interventions can reduce behavioral issues and improve quality of life of residents 5 ; recent multicenter studies confirm this finding. 1,6
Most studies, however, have been based on the use of a single type of intervention, such as music therapy, pet therapy, or aromatherapy and may not address the specific need underlying the dementia-associated behavior. These therapies require trained personnel (which limits the times and days of administering the intervention) or tend to focus specifically on calming an agitated resident through one-on-one care. There has been very little focus on individualized activities, which refers to the activities demanded by high-functioning residents or the act of proactively providing activities to keep residents engaged during times between scheduled activities and times when family members visit.
We have developed and implemented an individualized nonpharmacological intervention, the Behavior-Based Ergonomic Therapy (BBET) program, which combines the science of reducing stress (ie, ergonomics) with over 100 items in order to provide customized person-centered interventions and activities using information from resident profiles (learning, personality, and behavior) and level of cognitive functioning to determine a resident-specific action plan. The BBET program is not a group, but an individualized customized activity, that is available to the residents 24/7 through the staff, schedule-free. This is in contrast to the use of recreational therapists (RTs), who typically engage residents on a group or (sometimes) one-on-one basis driven by a specific schedule. Additionally, with minimal formal training (via an in-house certification program), BBET can be administered by the staff (nurses and aid). The staff need not have a dedicated activity specialization, unlike RTs who are credentials activity specialist. There is no specific guidance required to be imparted to the unit manager on how to implement the BBET program. The underlying idea of this program is to provide direct care via staff versus via specialist.
Furthermore, the key difference between the BBET and a few other multiple activity interventions proposed in the literature is that both the music and the video therapies are not typically included together along with stimulating interventions. A structured approach to provide multimodal therapies in a customizable manner that includes family inputs, and the 24/7 availability and ease-of-use (as indicated via our pilot study) is at the core of the BBET approach.
The long-term goal of this low-cost BBET program is to reduce cognitive stress and behavioral (or mood-related) issues such as agitation. A precondition for implementing the BBET program was that no additional staff would be hired to implement or maintain the program. A pilot study to determine the practical feasibility and effectiveness of this intervention was conducted in a dementia unit in a continuing care retirement community (CCRC) in west central Ohio. In this article, we describe the BBET approach as a potential person-centered nonpharmacological intervention and provide both qualitative and quantitative evidences for the effectiveness of this approach at this facility.
Methods
The BBET program is an International Review Board approved study and was developed in 2009 and implemented in 2010 in conjunction with executives and managers, family members, physicians, nurses and other members of the interdisciplinary team, and nursing assistants in a not-for-profit, religiously affiliated CCRC in west central Ohio situated on 240 acres. The campus consists of 250 cottages/garden homes, a 100-unit tax credit housing development, 83 independent apartments, 74 joint commission-accredited assisted living apartments, and a 120-bed joint commission-accredited Medicare/Medicaid nursing facility. Eighteen of the nursing facility beds comprise a dedicated dementia care unit for Alzheimer’s residents, referred to as the Alzheimer’s unit.
The residents in the Alzheimer’s unit are ambulatory but usually require help with meals (feeding assistance or prompting) and other activities of daily living (ADLs). A number of methods are employed to help reduce resident falls, increase engagement, manage challenging behaviors, and improve interactions among residents. For instance, shift changes are accompanied by completing fall safety rounds and alarm checks. A team-based incentive is implemented to reward unit teams that achieve zero falls each month. There are dedicated activity coordinators who facilitate group exercise in the morning and 1 to 2 group activities during the rest of the day. When a behavioral episode occurs, the staff usually attempt to calm residents by helping them with their needs (eg, hunger/thirst, discomfort, pain, and toileting), taking them to their room to soothe and redirect them, or walking with them around the unit. If the distressing or disruptive behavior does not improve, pharmacologic interventions are usually implemented, often accompanied by an assessment to search for new medical conditions or a change in existing medical or neuropsychiatric conditions.
During earlier projects at this facility, it was observed that the residents with Alzheimer’s disease or other dementias had different risk and precipitating factors for falls than the residents in the other units. It is often challenging for one activity to engage all the residents simultaneously (and sometimes crowds and transitions in and out of activities trigger behaviors in some residents). This motivated a creative exploration of nonpharmacological methods for managing a variety of behaviors, not only those that lead to falls. The term selected for the approach is the BBET program.
Behavior-Based Ergonomic Therapy Program
Ergonomics deals with the physiological and psychological effects of cognitive stress. Overburdened cognitive function in people with dementia develops into mental fatigue accompanied by general sensation of weariness. 7 The principles of ergonomics formed the underlying basis for this program. The program was named BBET to reflect the unique type of therapies needed to improve a resident’s interaction with the environment in light of the challenges associated with Alzheimer’s disease or other dementias. The BBET program aims at preventing nonclinical issues such as boredom and disengagement using comforting or stimulating interventions tailored to each resident’s interests and capabilities. Boredom and disengagement are primary causes of behavioral disturbances (negative behaviors) in residents with dementia. 8
The BBET program can be carried out in the following manner. First, the family members of a new resident are asked a series of questions designed by the first author. This questionnaire is designed to develop a personality (eg, life story) and interest profile for each resident. Second, resident learning style inventory is developed by personnel in the activities department, which is based off of an in-house procedure developed through several modifications of the Gardner theory; 9 describing this procedure is beyond the scope of this manuscript. Learning style information is collected by the staff (nurse or aid) from the activities department. Third, functional assessment is based on nurse observations and interviews with the resident and family. Fourth, behavior profile is captured, also by a nurse, through initial observations of the resident. Finally, all this information is combined to develop an action plan tailored for individual residents. For example, comforting therapy selections are determined from families (interest and personality assessment), while stimulation therapy selections are based on functional and learning styles.
Comforting interventions utilize portable CD and DVD players, headphones for each resident, a DVD library, and a music library. Also included is a prop box for each resident in which memory props provided by families can be stored securely. These items are often sentimental and provide comfort and joy for the residents. The family members are given a list of memory prop ideas to help them identify appropriate items for the program (ie, family photos, magazines, books, stuffed animals, etc). Stimulating interventions were designed for residents with medium-to-high cognitive functioning and included tools from the stimulating library such as stage-specific games and puzzles. These tools are kept in a resource center on the unit for easy and quick retrieval, instead of resident rooms where they may be difficult to find, become damaged, or destroyed.
The BBET program is designed not only as an intervention for challenging behaviors but also as a proactive approach to reduce boredom and cognitive stress, thus reducing the risk of more challenging behaviors. The program is available to residents 24 hours a day and the activities can also be requested when family members are visiting. The staff is trained to identify program opportunities throughout the day and night, facilitate BBET activities with “buddies” (ie, 2 residents interacting with each other or a resident interacting with a volunteer), and help family members utilize the program to enhance their experiences with their loved ones.
Pilot Details
The BBET program pilot began on February 18, 2010 with 3 of the 18 residents on the unit. The staff became comfortable with the program within 11 days compared with the anticipated 6 weeks, and by March 1, the caregivers were initiating and tracking BBE therapies on their own. The staff’s ability to choose an appropriate item in the libraries that produced a good outcome for the resident was important in implementing the program. Therefore, the 100+ library items were coded for easy access by caregivers. The specific codes from each library that will work best for each resident were determined through developing an individual BBET action plan utilizing information about the resident’s learning style, personality and behavior profile, and the resident’s cognitive skill level (Figures 1 and 2).
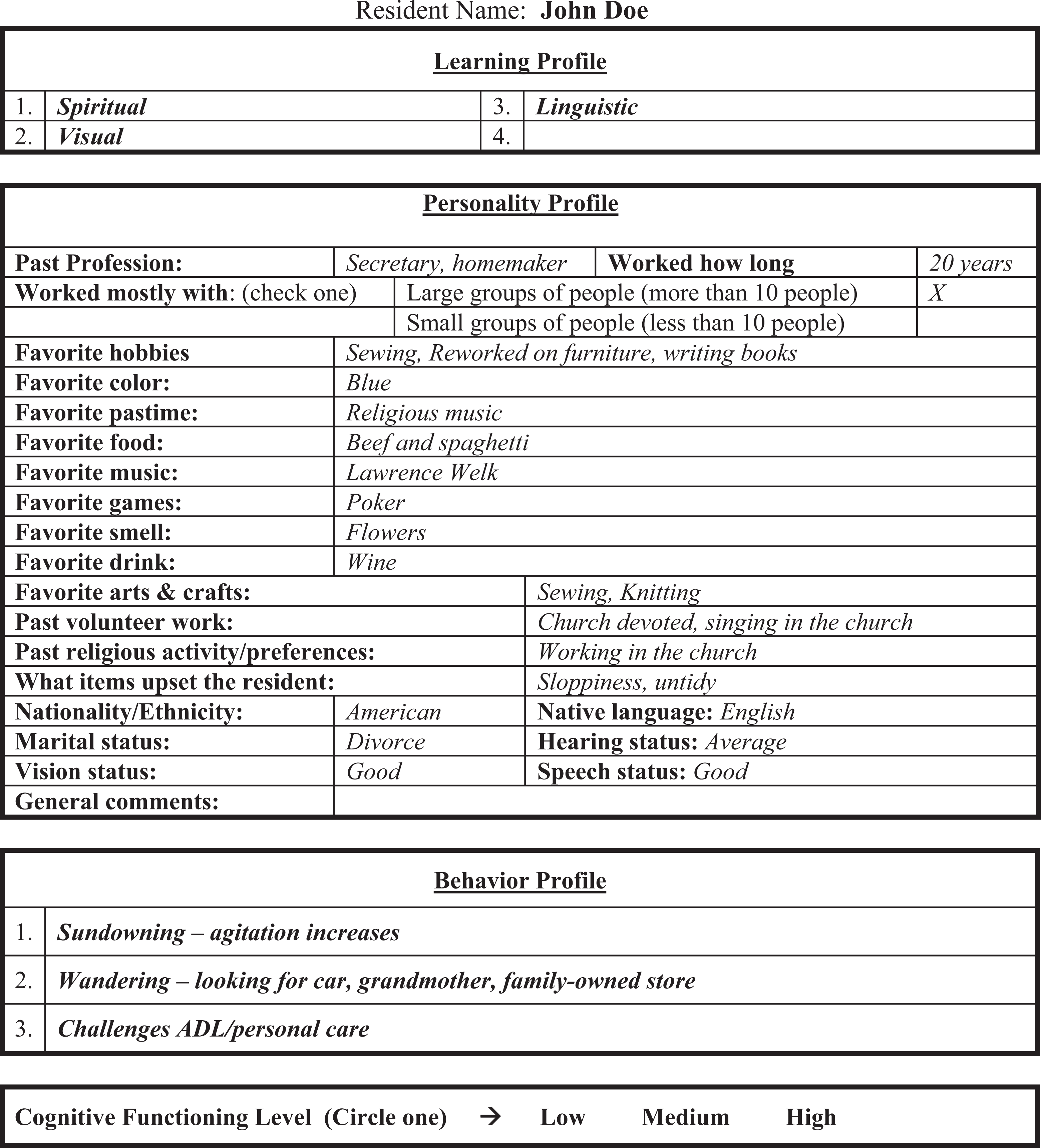
An example Behavior-Based Ergonomic Therapies (BBET) profile for a resident.
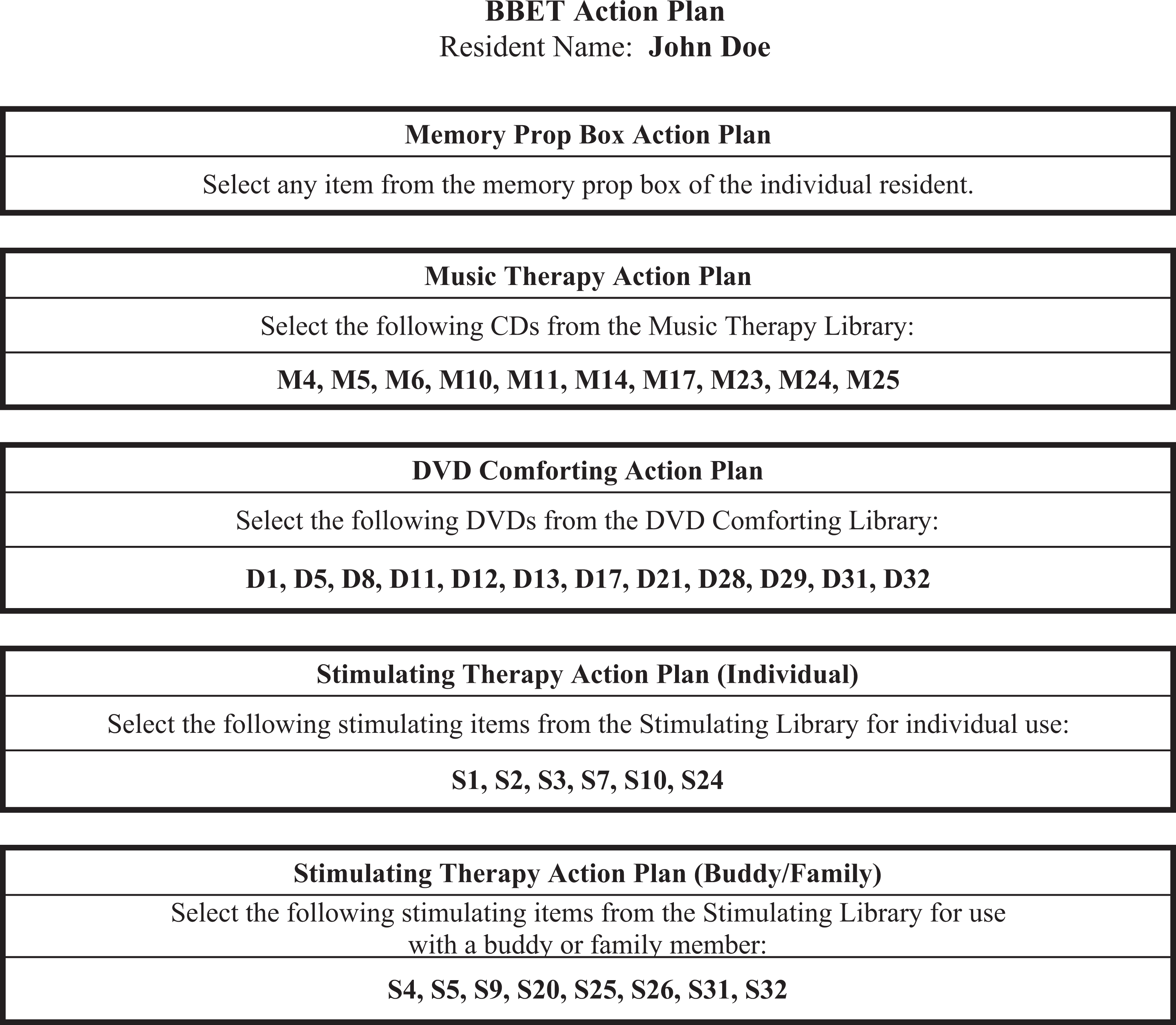
An example Behavior-Based Ergonomic Therapies (BBET) action plan for a resident.
The resident personality profile contains likes and dislikes and past “life-story” information about the resident. This information is used to initiate and encourage a resident to try an intervention. It helps caregivers to build relationships with the residents, so that the caregiver can discern usual from unusual behaviors. The behavior profile is used to fit the BBET program into a care plan. Investigating the usual time or triggers for behaviors to emerge (ie, when a family member leaves or when group activity ends) adds to the alignment of the program with person-centered care and a rhythm-of-the-day philosophy. The following is a list of behaviors used by the resident coordinator to fill in the behavior profile: wandering, shadowing, rummaging, aggressiveness, restlessness, hoarding, combativeness, agitation, inappropriateness, sundowning, disorientation, and withdrawal. In some cases, behaviors may also be correlated with learning styles. The cognitive skill level is used to determine which stimulating items are appropriate for each individual resident. Residents were observed with certain representative items from the stimulating library to determine which types of items were appropriate. The skill level is generally a factor in success of the intervention, along with attitude toward the activity. For example, if a small puzzle is not overwhelming, a resident with moderate cognitive impairment may be motivated to finish the activity even if it takes a long time.
The early morning staff incorporated prop box items into the care process when residents wake up and are waiting for breakfast (Table 1). It was expected that encouragement by the staff, the availability of simpler stimulating activities that still provide cognitive challenge, and removing distractions in the environment may contribute toward a calm and therapeutic environment. The staff can use the BBET codes in a resident’s action plan to obtain the appropriate intervention within about 3 minutes, initiate the intervention using guidelines presented in the BBET certification training, and then monitor the resident from a distance while performing other care tasks. This approach was expected to increase staff morale because caregivers can provide emotional support as well as physical or clinical support without increasing their overall workload.
Opportunities to Use BBET Throughout the Day
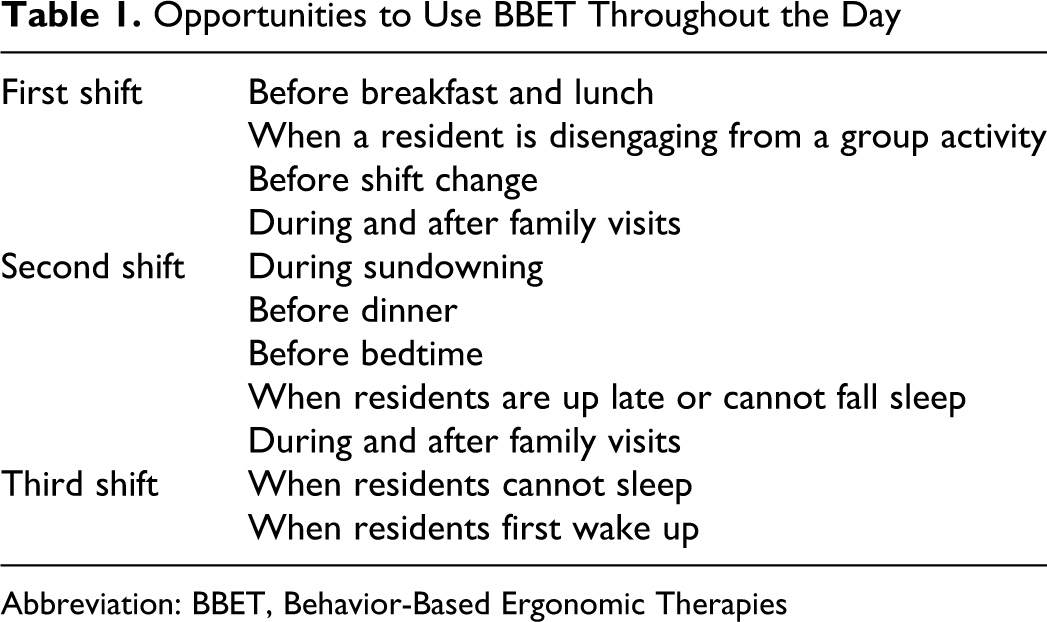
Abbreviation: BBET, Behavior-Based Ergonomic Therapies
New permanent caregivers and staff floating into the unit were allowed to participate in the program after undergoing an internal certification program that provided training on behavior management. This certification program included 4 hours of educational films, 1 hour of one-on-one training with a BBET training coordinator, and a certification exam. Although the certification program required some downtime from the staff, the lost hours and the associated cost were fairly low.
Evaluation Measures
The success of the program was dependent on the caregivers’ ability to initiate appropriate therapy, both proactively and while behaviors are escalating, in a timely manner and with minimal disruption of work flow. The staff captured the following information on each BBET intervention through the tracking sheet: resident name, item (ie, M16 for a CD, or PB for prop box), time started, time ended, and comments/feedback. Based on this information and other observations, the following measures were derived to measure the program’s effectiveness: number of interventions of each type (comforting including prop box and simulating), total contact time across all interventions, and falls. Total therapy contact time refers to number of hours that the residents were engaged in a personalized therapy, not going through behavior challenges, not adding to the stress of other residents. Contact time is calculated using the start and end time of each recorded intervention. When the caregiver pulls a therapy from the resource center, the start time is recorded (along with the resident’s name and item number) on a simple tracking sheet. When the therapy concludes, the caregiver returns the therapy items to the resource center and records the ending time. Because there is generally no delay in the documentation of start/end time (and because the staff is not actually calculating contact time), these data are reasonably accurate. Reduction in agitation levels was sometimes included in the comments section of the tracking sheet but was mostly an observational measure from the caregivers and family members.
Findings
The residents’ stay in the Alzheimer’s unit typically begins when they are ambulatory and ends when the resident is no longer ambulatory or requires extensive physical care to perform ADLs. During the pilot study, the number of residents in the unit ranged between 16 and 18 and had an average age of 82 years and an average length-of-stay of 358 days. Fifty-four percent of the participants were female. Resident tracking sheets served as the main source of quantitative and qualitative data collection, along with observations from caregivers and family members.
Number and Percentage of Therapy Interventions
Figure 3 shows the total number of therapy interventions, categorized as comforting and stimulating, provided during the 6-month pilot across 18 residents in the unit. In March 2010, a total of 111 interventions were administered, which increased to 320 by August 2010. The number of comforting therapies (counting the prop box tools) increased steadily from 92 in March 2010 to 304 in August 2010. While the number of stimulating therapies saw a steady increase from March through May 2010 (19 to 59 therapies). However, it dropped later due to staffing changes since the stimulating therapy requires higher training and intervention skill by the staff.
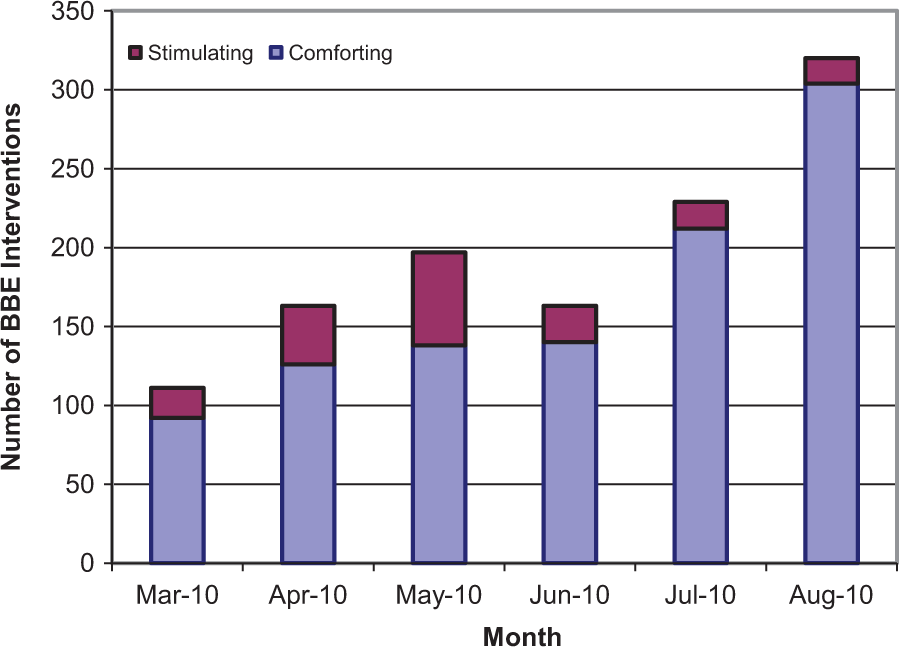
Number of Behavior-Based Ergonomic Therapies (BBETs) interventions by month during pilot study.
On the whole, stimulating therapy interventions comprised 15% to 20% of the total interventions as only medium-to-high-functioning residents used the stimulating library. Over 20% of stimulating interventions involved a buddy or family member, suggesting more interaction between residents and greater use of the program during visits with spouses, children, and grandchildren. Over 200 interventions of the first 1000 used memory props from prop boxes. This increased sharply in later months as the staff and manager worked with families to provide more items for the prop boxes. The team noted that contributions to the comforting libraries increased during the pilot study from 30 CDs and 32 DVDs to 43 CDs and 74 DVDs.
Tracking sheets also indicated that 90% of interventions lasted over 10 minutes, as indicated by the start and end times of the intervention. The 10-minute threshold was decided as it was observed to correlate well to the positive comments in the tracking sheets. The average time was 39 minutes for comforting therapies and 30 minutes for stimulating therapies (Figure 4).
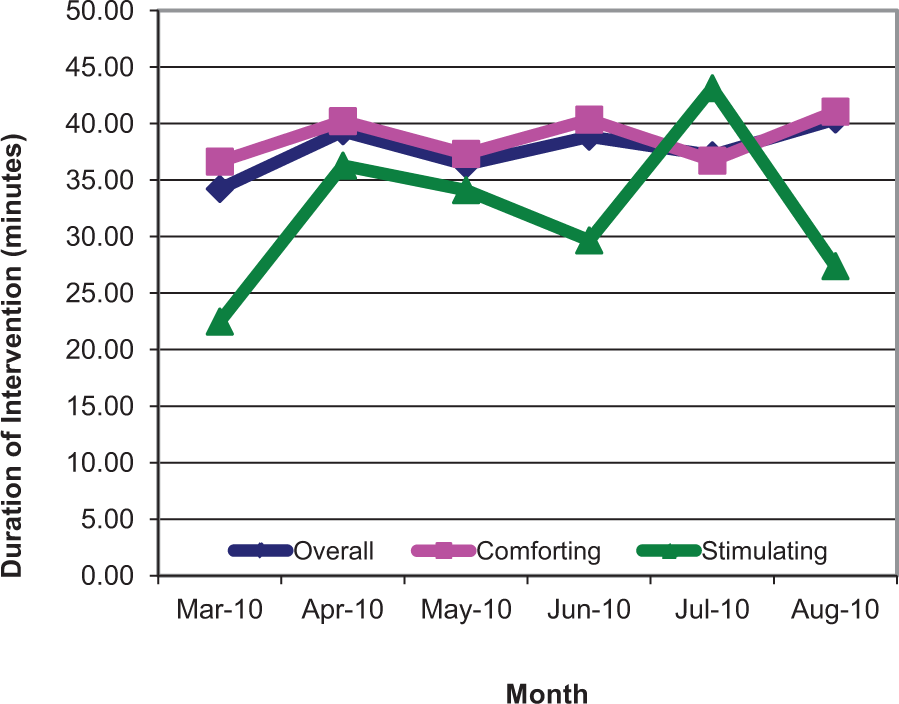
Average duration of Behavior-Based Ergonomic Therapies (BBETs) interventions by month during pilot study.
Total Therapy Contact Time
Figure 5 shows the contact time in hours by each month during the 6-month pilot. Monthly contact time for comforting therapy interventions was 56 hours in March 2010 and increased by 271% to 208 hours by August 2010. The total contact hours for comforting and stimulating interventions during the pilot were over 650 hours and about 94 hours, respectively.
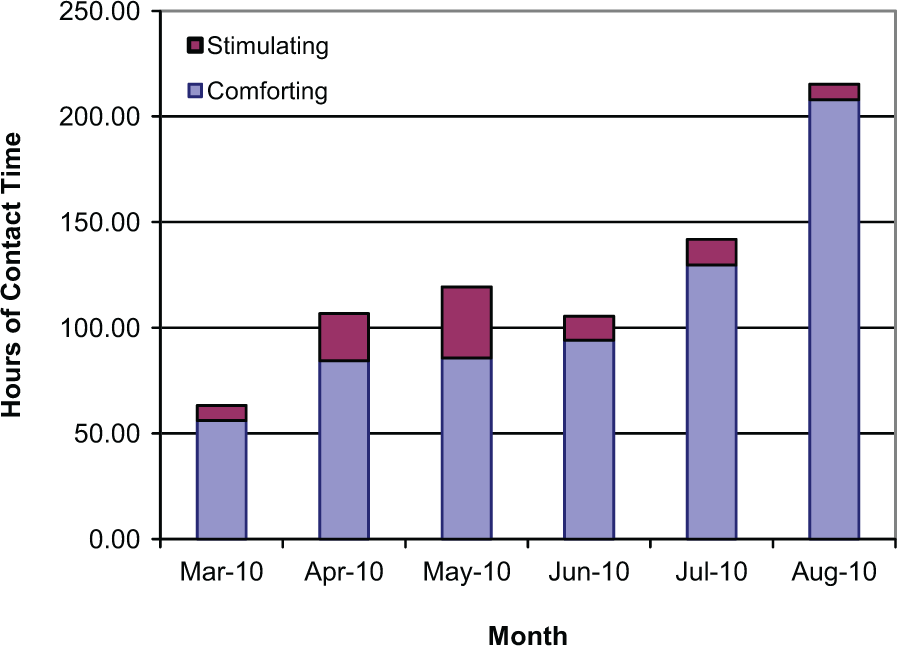
Total therapy contact time of Behavior-Based Ergonomic Therapies (BBETs) interventions by month during pilot study.
Reduction in Resident Falls
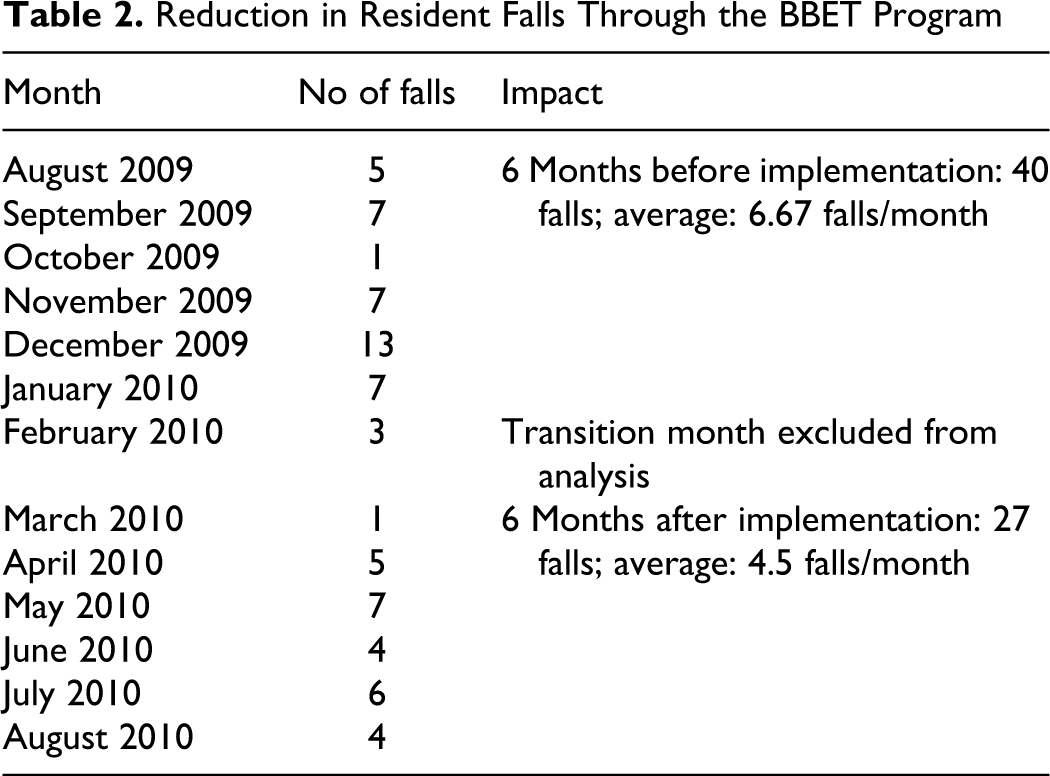
Given that the Alzheimer’s unit at St Leonard is an ambulatory unit, behavioral disturbances sometimes lead to wandering, shadowing, and rummaging, which increase the likelihood of falls. By mitigating the root cause of falls (ie, behavioral disturbances) through an increase in contact time, the likelihood of falls is reduced. We observed that resident falls decreased by 32.5% during the pilot study, as shown in Table 2. The average number of falls 6 months prior to the implementation of the BBET program (August 2009-January 2010) was 6.67 falls/month. This number dropped to 4.5 falls/month during the first 6 months of implementation (March-August 2010).
Reduction in Resident Falls Through the BBET Program
Reduction in Agitation Level
Staff and family members noticed a marked improvement in the agitation levels of residents and their loved ones. Following are quotes from these members based on their observations during the pilot: “I’m completely amazed. The tough residents were more calm and quiet, and we were able to get more people up before shift change.”—third Shift Aide “I’m glad the higher-functioning residents are coming out of their rooms more. We are doing more to engage them now.” —first Shift Aide “This can help the family members enjoy more activities with their loved ones when they visit.”—Social worker “The emergency calls about resident behaviors and agitations have reduced sharply after the implementation of the BBET program”—Medical Director “These tools are simple and yet effective way to break communication barriers when you don’t know what to say.”—Grandson of a resident “This program to individualize the activities has had a very positive impact on the Alzheimer’s residents. The atmosphere is calmer.”—Daughter of a resident “This is useful before breakfast when the aides are busy and residents have to wait for the meal to arrive. It is nice to start their day with something they like.”—third Shift Nurse “This program will definitely reduce the stress of the residents and stress on the staff. It is very beneficial.”—Unit Manager “My dad felt better about himself and more successful. He feels good when he is helping people, and I’m so happy he is coming out of his room and interacting more.”—Daughter of a resident
Discussion
Nonpharmacological interventions can alleviate many behavioral disturbances experienced by residents with Alzheimer’s disease and other dementias and should be attempted first, followed by the least harmful medication for the shortest time possible. 10 These interventions include modifications of the physical or social environment, 11,12 removal of physical restraints, 13 music therapy, 14,15 exercise, 16 aromatherapy, 17 and real or simulated social contact, for example, family videotapes and one-on-one social interactions 18 and animal-assisted therapy. 19 Combination interventions have also been successful, such as the Activities, Guidelines for psychotropic medications, and Education (A.G.E) program, which included activities, guidelines for psychotropic medications, and educational rounds. 20 Several of these interventions could be used as individualized therapies in an effort to provide person-centered care. Such a care plan has recently gained attention of researchers and practitioners as it is grounded in understanding the preferences and needs of residents. 1,21
Most proposed person-centered plans combine nonpharmacological interventions; however, these plans often are limited by the number of interventions used and the schedule for administering the interventions. Well-designed person-centered plans should allow for a large variety of intervention tools, be available at the time the resident is ready, engage the resident without extended one-on-one assistance from the staff, and require little effort from the staff during training and continuous administration. From that perspective, we developed a person-centered nonpharmacological intervention program, BBET, designed to enhance each resident’s sense of dignity and quality of life. The BBET combines concepts from ergonomics with person-centered care and employs both comforting and stimulation therapies with a total of over 100 tools. The program transformed the learning, personality, and behavior profiles and cognitive level of each resident into a resident-specific action plan. The BBET program was successfully implemented in a dementia unit in a CCRC and changed the way caregivers and family members were able to engage residents, both proactively and while behaviors are escalating. High level of therapy contact time with the BBET program greatly reduced residents’ risk of falls as they were engaged more, while reducing their agitation for the rest of the day, and in some cases improving their sleep.
The BBET program has several strengths. The 24/7 access to the BBET program can be treated as a complementary individualized activities program not tied to a schedule, but rather driven by the cues from the resident. The availability of these interventions allows the staff to provide enjoyable activities when the residents are ready to receive them. The role of the staff is to start the therapy intervention and engage the resident without requiring one-to-one caregiver assistance. The staff can monitor the resident “from a distance” while caring for another resident. This special ability to better manage their time in a care giving role gives the staff more capacity to provide emotional support in addition to physical and clinical support, thereby potentially improving the morale of the staff because they can use the BBET tools to deliver a positive care experience without increasing their overall workload. This program is practical and adaptable to all care settings, and it has a low setup cost and minimal learning curve. No new staff members were hired to sustain the program. This is because if and when an abnormal behavior is identified by the staff, a BBET intervention is administered immediately. It takes about 2 to 3 minutes to initiate the intervention and less than a minute to record the contact time of the intervention in a tracking sheet if the intervention is successful. That is, the total time required through the use of BBET to proactively detect and manage a behavioral disturbance is less than 5 minutes compared with 10 to 60 minutes of managing a behavior when it occurs. This time difference more than offsets the increase in tasks required to develop a one-time BBET action plan for new residents, thus eliminating the need for additional staff. Furthermore, the empowerment roles among the staff appeared to foster a sense of teamwork, ownership, and continuous improvement.
Our study has several limitations. First, this pilot was conducted at a single 18-bed Alzheimer’s unit. This could limit the generalization; however, BBET is now being implemented in adult day care where the outcomes and results are being monitored. Second, given the experimental nature of this study, our assessment of reduction in agitation levels was primarily observational. Using standardized scales to assess baseline level of cognitive functioning (eg, Mini-Mental State Examination) and agitation (eg, Cohen-Mansfield Agitation Inventory or the Neuropsychiatry Inventory–Nursing Home scale) is expected to provide additional quantifiable outcome measures. Third, the significance of the findings through this pre–post pilot study, like many previous studies, may have been affected due to the presence of nonspecific factors that were either difficult to identify or measure. A randomized control trial is preferred, however, may not be practical at every facility.
The BBET program addresses withdrawn or passive behaviors as well as disruptive behaviors. While the more agitated residents receive more attention from caregivers, the BBET program is often used to get the quieter residents, including those who are early in the disease and prone to depression, out of their rooms. In this regard, it is more than a behavior management program and becomes part of the unit’s socialization process. It could be speculated that this constructive interaction and the cognitive exercise offered by the stimulating therapy will prevent subsequent episodes of agitation.
When implementing the BBET program at other facilities we realized that the elements in the BBET profiles used to create each resident’s BBET action plan could be further expanded. For example, Gardner theory of multiple intelligences, which was used to derive the learning styles of residents on the unit, can also be used by the activities director to systematically tailor group activities to smaller clusters of residents. In order to most effectively tailor interventions to the patient’s behavior, we selected learning styles that directed the appropriate intervention (audio, linguistic, kinesthetic, visual/spatial, and interpersonal/intrapersonal). This can be included in the advanced BBET training for staff or in continuing education after further investigation.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.