
Abstract
The conditions associated with wandering in people with dementia include purposeless activity, purposeful actions, irritation, and symptoms of depression. The words and actions of 5 people admitted to long-term health care facilities who often exhibited wandering behavior were observed, and the above conditions were studied based on our self-awareness model (consisting of “theory of mind,” “self-evaluation,” and “self-consciousness”). One person who had not passed the theory of mind task but had passed the self-evaluation task was aware of her wandering. However, she could not understand where she wanted to go or for what purpose. Four persons who had not passed the self-evaluation tasks were not aware of their wandering and had no purpose for their wandering.
Introduction
The deteriorated quality of life of people with dementia and their families and the difficulty in caring for these people are attributable to the behavioral and psychological symptoms of dementia (BPSD). The BPSD can be divided into psychological symptoms, such as anxiety, irritation, suspicion, hypochondriacal and persecutory delusions, depression, and behavioral symptoms, such as violent language, violence, repeated asking of questions, care refusal, wandering, undressing in public, and urination/defecation. There are currently approximately 2 million people living with dementia in Japan. 1 However, it is extremely difficult to care for people with dementia, and these people account for 80% of the elderly population having domestic abuse. 2 The main cause of the abuse is an increase in the burden of care triggered by the BPSD. 3
In this article, we present the results of an investigation of the conditions associated with one of the BPSD, namely, wandering, which can trigger a need for institutionalization and can cause traffic accidents. Purposeless activity, purposeful actions, irritation, and symptoms of depression are considered as conditions associated with wandering. 4 Why do these patients show purposeless activity? Why can they perform purposeful actions? Why do they get irritated? Why do they feel depressed? These questions must be answered to explain the conditions associated with wandering. Nonpharmacological interventions are the first choice of treating BPSD, including wandering; yet their efficacy has not been proven. 5 -9 On the other hand, pharmacological treatment, which is the second choice, is widely used. However, none of the pharmacological treatments have shown a dramatic efficacy. 10 –14 Besides, recent research has pointed out an increase in the mortality rate. 15 –17 Therefore, understanding BPSD by putting ourselves in the place of people with dementia is crucial, instead of merely pursuing a statistical decrease in BPSD.
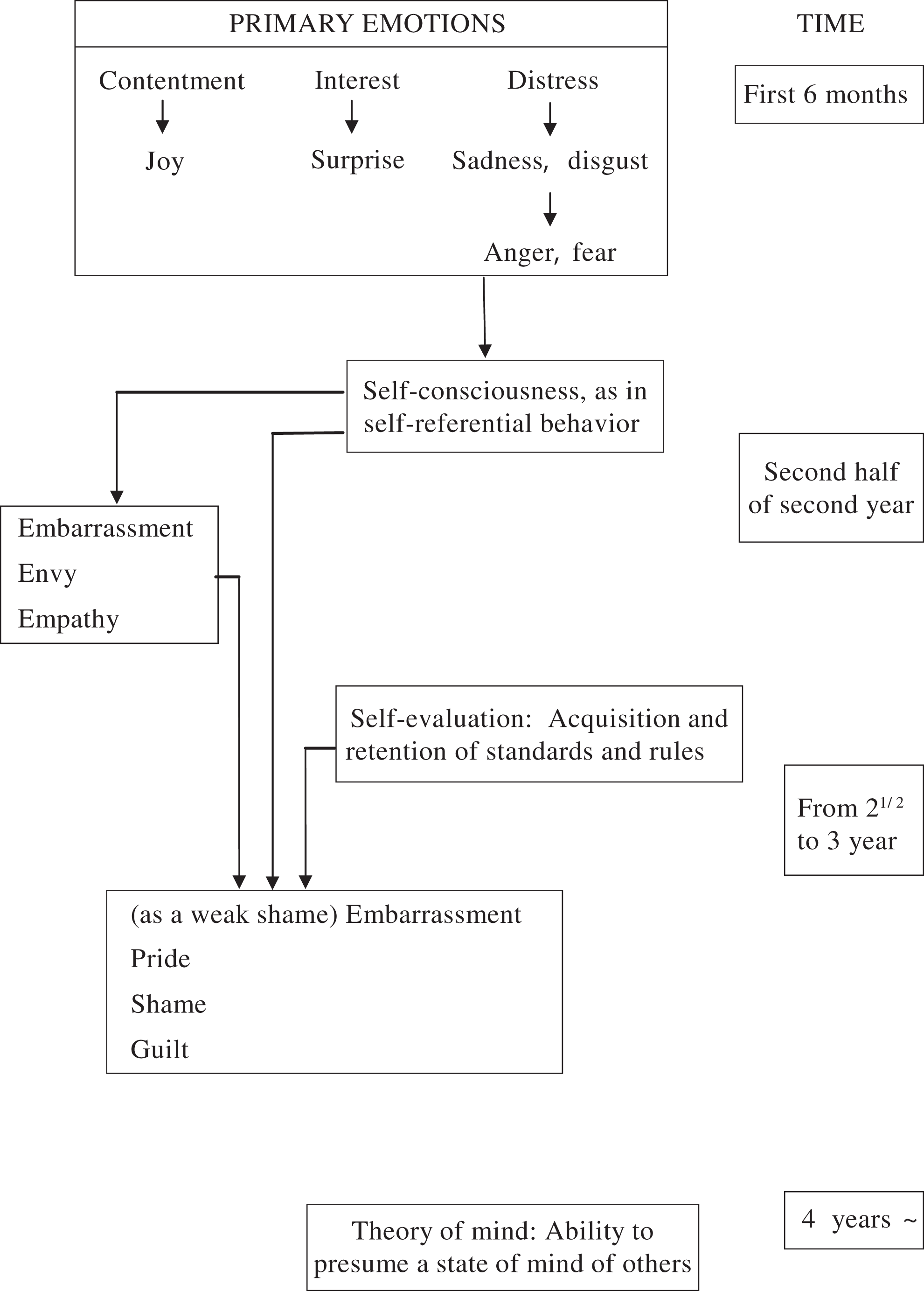
Dementia is defined as a state in which acquired mental functions, such as memory, judgment, language, and emotion decrease or disappear, thereby limiting daily life and social life activities. 18 However, dementia is not a mixture of impairments in intellectual functions, such as memory impairment, impaired judgment, and disorientation, but a state in which the intellectual subject integrating these intellectual tools is invaded, 19 which will defy an understanding of the whole picture of dementia, even if the intellectual functions are scrutinized piece by piece. 20 Therefore, to interpret the words and actions of people with dementia, we paid attention to self-awareness, the intellectual subject integrating intellectual tools, and examined how humans would have acquired self-awareness in the first place. Toward the end, we first identified “a developmental model of cognition and emotion” by a developmental psychologist, Lewis, 21 ,22 and “theory of mind” by the psychologists Wimmer and Perner 23 (Figure 1). According to Lewis, a human is born with emotions of “contentment,” “curiosity·interest,” and “distress,” and a baby in relation to others develops and differentiates emotions such as “joy,” “surprise,” “anger,” and the likes. At approximately 1.5 years of age, “self-consciousness” arises, by which an individual becomes aware of his or her own presence and begins to observe oneself closely to distinguish between self and others; the emotions of “embarrassment” and “empathy” develop at this time. At 2.5 to 3 years of age, an individual acquires the function of “self-evaluation,” by which they understand the rules and standards of the society in which they live and judge whether their thoughts, emotions, and actions are good or bad in comparison with the rules and standards; at this time, the emotions of “shame” and “guilt” develop. In addition, although it is usually assumed that the function of mind is as the background of other’s behavior, 24 Wimmer and Perner 23 revealed that the children can acquire the theory of mind, which is the ability to estimate psychological states (intention, thought, belief, desire, emotion, preference, etc) that are in the background of the behaviors of oneself and others and cannot be directly observed 25 at 4 to 6 years of age. In other words, the appearance of self-consciousness makes infants aware of their own presence and gives them the ability to distinguish between self and others; self-evaluation makes them begin to prepare to adapt themselves to the rules of the society in which they live; theory of mind makes them estimate others’ minds to adapt themselves to human relationships with many unspecified people. The development of self-awareness is the basis by which infants adapt themselves to complex human relationships.
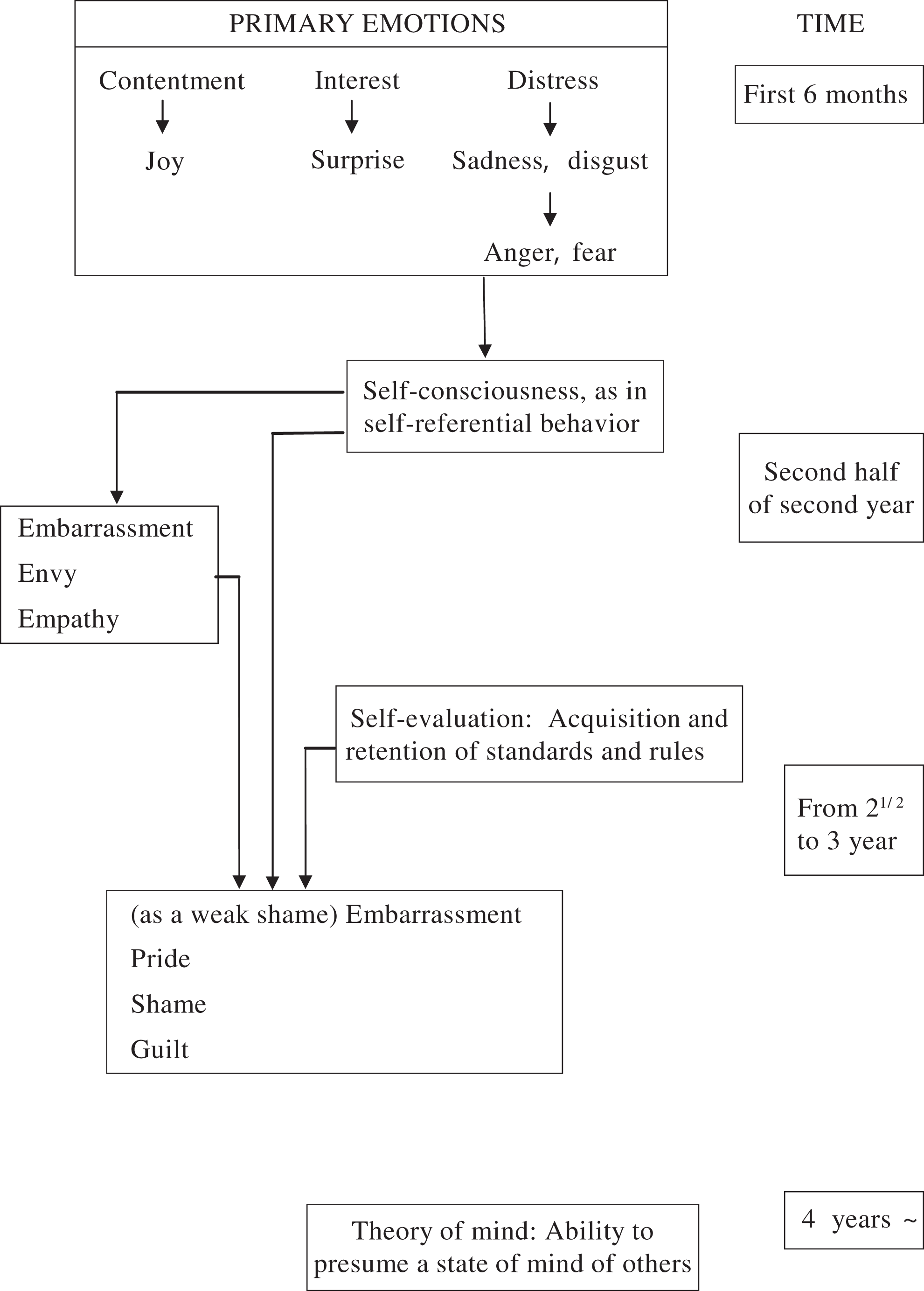
Development process of self-awareness of infants (compiled from Lewis’s developmental model of cognition and emotion, and Wimmer’s and Perner’s theory of mind).
Moreover, in today’s evolutionary theory, the social intelligence hypothesis is also widely accepted; this hypothesis suggests that “intelligence” evolved not because humans were tool makers but because they had to adapt themselves to complex human relationships, such as cooperation and negotiation with other individuals in a group. 26 –28
We perceived that the progression of dementia is a process in which one becomes unable to adapt oneself to complex human relationships as a result of decreases in cognitive functions. We hypothesized that people with dementia follow a process opposite to that observed in infants when adapting themselves to human relationships and created “a model for interpreting puzzling words and deeds of people with dementia from the viewpoint of self-awareness” 29 ,30 (Figure 2).
Model for interpreting puzzling words and deeds of people with dementia from the viewpoint of self-awareness.
In this article, we report the results of our investigation of the conditions associated with wandering in people with dementia; the investigation was based on our self-awareness model and observations of 5 people with dementia who exhibited wandering behavior.
Participants and Methods
Participants
Of the 48 people admitted to the dementia wards of the long-term health care facilities surveyed in our study and who had been diagnosed as having dementia according to the Diagnostic and Statistical Manual of Mental Disorders (Fourth Edition; DSM-IV) criteria, 31 the words and the actions of 5 individuals who commonly exhibited wandering behavior were examined. These 5 people had entered the facilities at least 1 year earlier, so their wandering was not caused by temporary confusion arising from environmental changes.
For ethical considerations, the objectives and methods of the study were explained to the families of the 5 individuals, and written consent was obtained from each of them.
Methods
Assessment of Wandering
Two of the authors observed and recorded the words and the actions of the 5 participants, mainly those occurring during scenes of wandering, for 3 days (from 9
Assessment of the Ability of Self-Awareness
Two of the authors collaboratively assessed the theory of mind, self-evaluation, and self-consciousness in a quiet place, considering the maintenance of the participants’ attention and the degree of their hearing loss.
Assessment of the presence or absence of theory of mind
The author sat face-to-face to the participant across a table, showing much simplified adaptations of 4 picture cards that were originally in the version of “Wrong Belief” of Wimmer and Perner depicted by Muto 32 and confirmed the presence or absence of theory of mind by pointing to the cards for each scene, while slowly reading out the description seen in Figure 3. If the answer of the participant was the round box, the theory of mind was judged to be present.
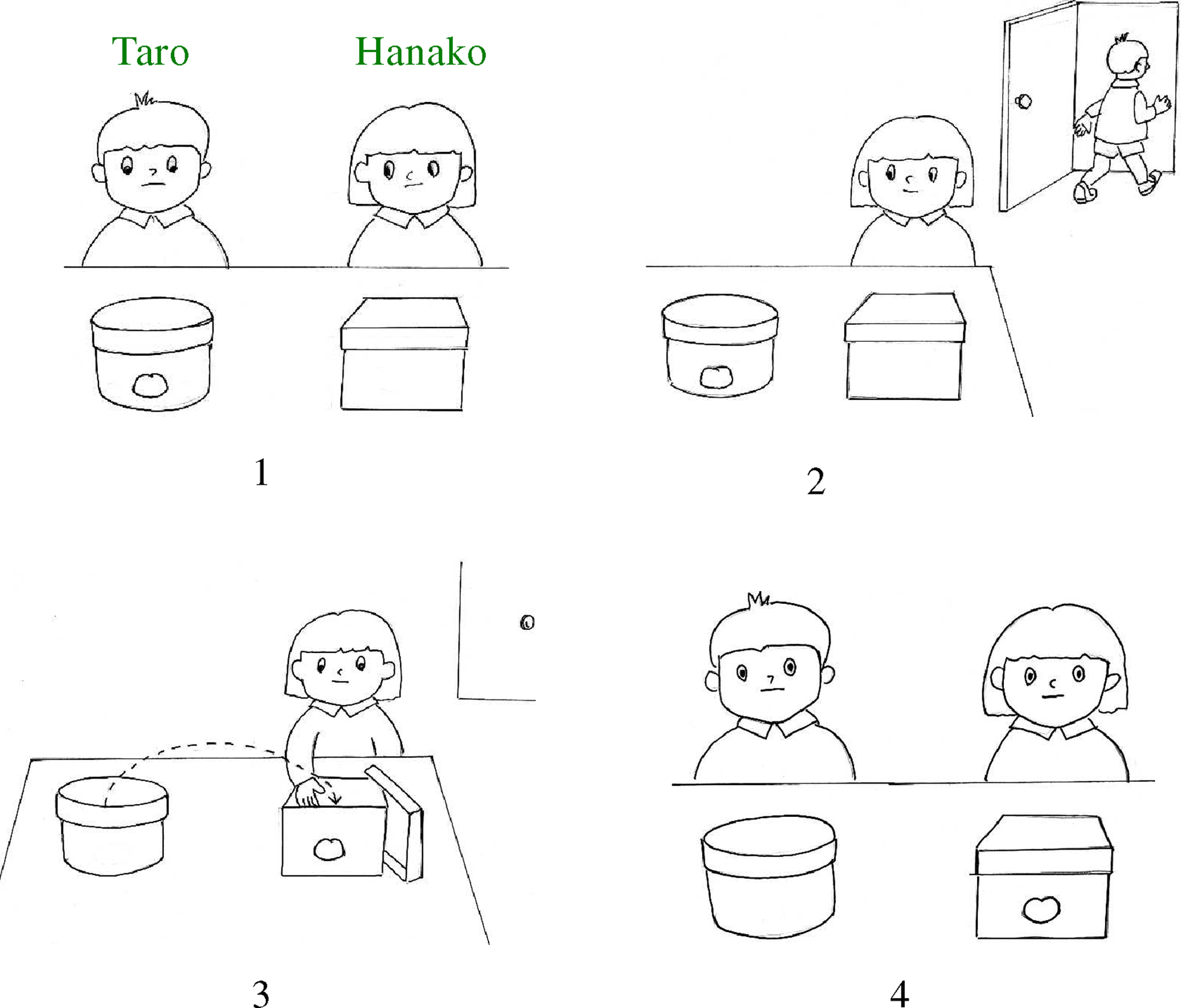
Assessment of the presence or absence of theory of mind.
Assessment of the presence or absence of self-evaluation
Lewis had not shown any method of assessing the presence or absence of self-evaluation; therefore, we created 4 pairs of picture cards that could be used to assess understanding of the basic rules and standards of Japanese society (Figure 4). 29,30 The authors sat at a table across from each participant and showed him or her these 4 pairs of picture cards, one pair at a time. After confirming that the participant was paying attention to the cards, the authors slowly read out the contents of the picture cards using the name of the subject for XXX, as shown in Figure 4. The cards illustrating women in the same scenes were used for the female participants. If the participant correctly answered all 4 tasks, self-evaluation was judged to be present.
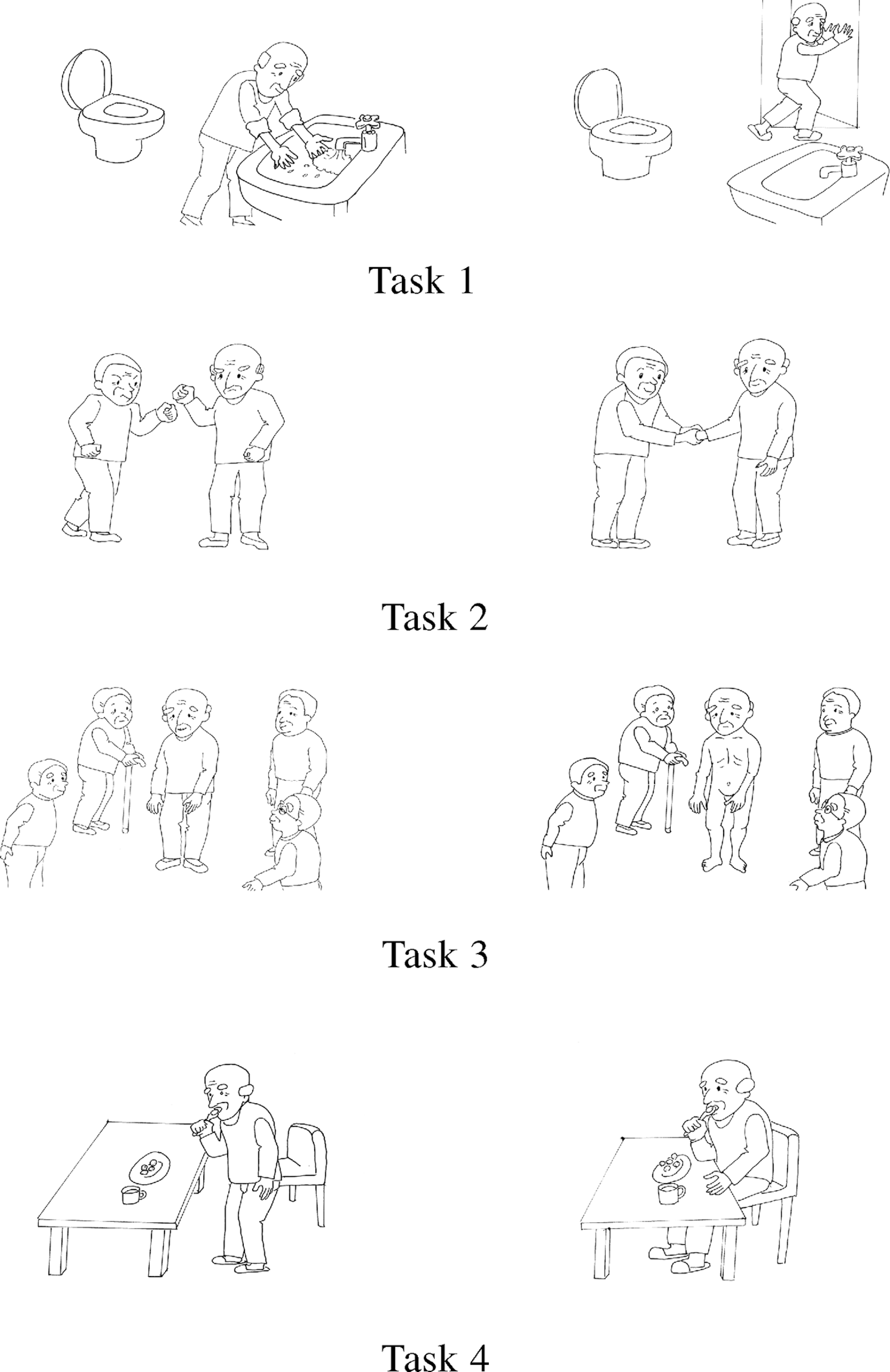
Assessment of the presence or absence of “self-evaluation.”
According to Lewis, the self-evaluation ability develops from 2½ to 3 years old. In order to confirm whether the above task was appropriate for the cognition ability in this age span, a child care worker in charge at a child care facility conducted a study in which the characters on the cards were changed into children. Twenty-eight children participated with the consent of their parents, with ages from 1 year 7 months to 3 years 11 months. The results confirmed that the age of 2 years 11 months in most of the children was appropriate for the development of self-evaluation.
Assessment of the presence or absence of self-consciousness
Lewis 21 ,22 put red lipstick on the tips of the noses of infants without drawing their attention to it and assessed the presence or absence of self-consciousness by examining whether the participants touched the tips of the noses when shown their faces in the mirror. However, people with severe dementia do not have high interest, unlike infants, and have attention deficits; therefore, the lipstick task cannot be used. Accordingly, the participant’s name 33 (last name and first name), which is the core of the perception of self and others and a symbol indicating the reality of each person, another person’s name, and the meaningless sound, “ahh,” were uttered from behind the participant, and the participant’s response was verified by the presence or absence of an answer or looking back. If the participant answered or looked back only on hearing his or her name, self-consciousness was judged to be present.
Assessment of the Severity of Impairment in General Cognitive Function
The severity of impairment in the general cognitive function was collaboratively assessed by 2 of the authors and the care workers engaged in daily care using the Clinical Dementia Rating. 34
Analysis Method
First, the participants were classified into 4 stages according to the presence or absence of the theory of mind, self-evaluation, and self-consciousness (those who had passed the theory of mind task, those who had not passed the theory of mind task but had passed the self-evaluation tasks, those who had not passed the self-evaluation tasks but had passed the self-consciousness task, and those who had not passed the self-consciousness task). Next, scenes of wandering and scenes related to self-awareness apart from that of wandering were put in order for each participant and the conditions associated with wandering were investigated based on our model. The reason for describing scenes related to self-awareness apart from the scenes of wandering was to clarify the characteristics of wandering from the viewpoint of self-awareness.
Results
I. Participants who passed the theory of mind task
None of the participants exhibited wandering behavior.
II. Participant who did not pass the theory of mind task but who passed the self-evaluation tasks
Case 1: A woman in her 80s with Alzheimer-type dementia; Clinical Dementia Rating (CDR): severe
<Scenes of wandering>
Scene 1: While wandering, she talked to another person with severe dementia who was also wandering and said, “I do not know where to go, please take me with you.” She clasped the person’s hand and began to wander with the person.
Scene 2: With a sad look on her face, she told the author, who was walking closely with her, “Everyone thinks that I am walking for pleasure.”
<Other scenes related to self-awareness> Scene 3: After assessing the severity of her cognitive function impairment using picture cards, the author said to her, “Thank you very much,” and she replied, “Thank you very much, although I do not understand anything.” Scene 4: While talking, she often covered her face with her hands and, with a look of crying, would say, “Ah, I do not know what to do.” Scene 5: While talking to the author, she said, “I do not know anything, but you are kind to visit me. You are big and I am small.” After a while, she pointed with her finger to a mountain outside the window, saying, “You are a big mountain and I am a small mountain.” Scene 6: She repeatedly asked the author, “Are you higher or lower than me?” In addition, while looking at another person staying at the facility, she said, “Is he/she higher or lower than me? I wish he/she were lower than me. If higher, it is no good; it would be a pity.” Scene 7: While the author was sitting next to her, she ate half of her afternoon snack and held the remaining snack out to the author, saying, “I have eaten, you please eat.” Scene 8: Every night, she would come out of her room to use the bathroom. However, after she had used the bathroom with the assistance of the staff, the staff would take her to her room and she would rest until morning without wandering. III. Participants who did not pass the self-evaluation tasks but who passed the self-consciousness task
Case 2: A woman in her 70s with Alzheimer-type dementia, Clinical Dementia Rating (CDR): severe
<Scenes of wandering>
Scene 1: She often wandered, following approximately 1 m behind the participant in case 3, who wandered at a quick pace. Scene 2: When she wandered alone and the author was ahead of her, sometimes she would approach the author with a smile, and sometimes she would pass by the author with her head down and a gloomy look on her face. Scene 3: One day, she suddenly stood up from her chair in the dining room, saying, “I am sorry, I will go out for a while. Please wait.” She then started to wander along the corridor. Scene 4: She wandered in her room and along the corridor, even at night.
<Other scenes related to self-awareness>
Scene 5: She rarely approached others. When we said “Hello” to her, she would reply “Hello,” and when we asked her, “Are you bored?”, she answered, “Ah, yes.” She did not continue any further conversation. Scene 6: She laughed upon hearing the word “naked,” which appeared in one of the questions of the self-evaluation tasks. Scene 7: A meal was served, but she did not begin to eat. When she was told to eat, she took chopsticks and began to eat, but stopped eating again soon. Scene 8: She sometimes urinated on the floor of her room not only at night, but also during the day. Scene 9: A male inpatient who was sitting at the same table as her was rapping on the table and speaking with a loud voice, and she said to the author, “Something scares me.”
Case 3: A woman in her 60s with Alzheimer-type dementia, Clinical Dementia Rating (CDR): severe
<Scenes of wandering> Scene 1: The author would be standing ahead of her, but she often passed by without even looking back. Scene 2: She often wandered at a quick pace along the corridor with her head down, with a blank expression on her face, and occasionally entered others’ rooms and the bathroom along the corridor; then she would hang around without doing anything in particular, and then she would begin to wander again along the corridor. Scene 3: While she was wandering, case 2 often wandered behind her, following her from approximately 1 m behind, but she did not look back at all. Scene 4: She hardly understood others’ words, but while nodding at what another inpatient at the same table was saying, she suddenly got up and began to wander. Scene 5: She wandered in her room and along the corridor, even at night.
<Other scenes related to self-awareness>
Scene 6: The author asked her, “Do you have children?” and she answered, “Yes.” The author asked her, “How many?” and she answered, “1, 2, 3, 20, about that many.” Scene 7: While looking at an empty bed, she said, “Grandpa, grandpa, how are you doing?” Then she looked sideways and said, “Here you are, grandma, too.” Scene 8: She often talked to herself in the mirror. The author stood by her side, but she hardly turned her eyes to the author in the mirror. Scene 9: During meals, when we made her hold chopsticks, she was able to use them, but soon she would drop them and begin to eat with her hands. Scene 10: She sometimes urinated on the floor of her room and at the edge of the corridor not only at night, but also during the day.
Case 4: A woman in her 80s with Alzheimer-type dementia, Clinical Dementia Rating (CDR): severe
<Scenes of wandering>
Scene 1: Her walking was unstable, and she wandered slowly using the handrail along the corridor. During wandering, she entered others’ rooms, but did nothing there. After a while, she returned to the corridor and started walking again, holding on to the handrail.
Scene 2: During wandering, she sometimes tried to pick up something from the floor even when nothing was present.
Scene 3: She wandered in her room and along the corridor, even at night.
<Other scenes related to self-awareness>
Scene 4: She sometimes lay down on the floor.
Scene 5: She undressed in the dining room, in full view of the other inpatients.
Scene 6: She put her finger into a hole in a sofa, which seemed to be a meaningless action.
Scene 7: She used a spoon upside down for eating and soon dropped the spoon and began to eat with her hands. She also licked plates.
Scene 8: She held her shoes that had fallen off her feet to the author’s feet, which seemed to be a meaningless action.
Scene 9: She often urinated and defecated in the corridor and her room not only at night, but also during the day. IV. Participant who did not pass the self-consciousness task
Case 5: A woman in her 80s with Alzheimer-type dementia, Clinical Dementia Rating (CDR): severe
<Scenes of wandering>
Scene 1: While she was wandering, the author would stand ahead of her, but she would often pass by without turning in the author’s direction.
Scene 2: She often wandered carrying rolls of toilet paper or a futon in her arms.
Scene 3: During wandering, she repeatedly pushed and pulled the handrail along the corridor, which seemed to be a meaningless action.
Scene 4: While wandering, she entered the pantry, and the staff held her shoulder to change her direction toward the door of the pantry. She did not resist and began to walk in the direction directed by the staff, as if she did not have her own will.
Scene 5: She wandered in her room and along the corridor, even at night.
<Other scenes related to self-awareness>
Scene 6: During the day, she was often found to be taking a nap on a chair or wandering.
Scene 7: She ate a meal if food was brought to her mouth, but when we made her hold snacks in her hands, she did not try to eat them.
Scene 8: She often urinated and defecated in her room and in the corridor not only at night, but also during the day.
Discussion
Case 1, who did not pass the theory of mind task, but who passed the self-evaluation tasks, talked to the author with a sad look on her face and said, “Everyone thinks that I am walking for pleasure” (scene 2). These words indicate that she was aware of her condition of wandering. The fact that she was aware of her condition was also well observed in other scenes, as represented by the following words and actions: when she said, “although I do not understand anything” during the assessment of cognitive function impairment using the picture cards (scene 3); when she covered her face with her hands, with a look of crying on her face, and said, “Ah, I do not know what to do” (scene 4); when she said, “you are a big mountain and I am a small mountain,” with her finger pointing to a mountain outside the window and when she repeatedly asked, “is he/she higher or lower than me? I wish he/she were lower than me. If higher, it is no good; that would be a pity,” while looking at another inpatient (scene 6); and when she said, “I have eaten, and you please eat,” while eating her afternoon snack (scene 7). As shown in Figure 1, emotions of pride and shame are considered to be retained in persons who can self-evaluate. These confusing words and actions performed with irritation, and the patient’s words showing feelings of inferiority are considered the result of a self-evaluation of her condition using her diminished intellectual functions while retaining the emotions of pride and shame. However, as shown by her misunderstanding that people around her thought that she was walking for pleasure, she could not correctly estimate others’ minds (intentions, thoughts, etc). In addition, as shown by her saying to another person with severe dementia who was walking by while she was wandering, “I do not know where to go, please take me with you” (scene 1), she thought that she wanted to go somewhere, but did not know where she wanted to go or what she wanted to do (purpose). The purpose is to arrive at the expectation by imagining future scenes and realizing them. 35 This participant was thought to be unable to estimate her own mind (intention, thought, desire, etc) and, as a result, she could neither find a purpose nor imagine future scenes.
Cases 2, 3, 4, and 5, who had not passed the self-evaluation tasks, including the one who had also not passed the self-consciousness task, were speculated to be not clearly aware of their conditions not only during wandering but also during other life scenes and to have almost lost the emotions of pride and shame. This is well represented by their actions of not meeting with others’ eyes, the action of case 2 of urinating on the floor of the room during the day (scene 8), the actions of case 3 of eating with her hands (scene 9), and urinating on the floor of the room and at the edge of the corridor during the day (scene 10); the actions of case 4 of lying down on the floor (scene 4), undressing in the dining room in full view of the other inpatients (scene 5), eating with her hands and licking her plate (scene 7), and urinating and defecating in the corridor and in the room during the day (scene 9); and the action of case 5 of urinating and defecating in the room and in the corridor during the day (scene 7). In addition, wandering is considered to be purposeless. For example, case 2 wandered approximately 1 m behind case 3, who wandered at a quick pace (scene 1). She was moved by something other than her own will. Case 3 wandered at a quick pace along the corridor with her head down, with a blank expression on her face, and entered others’ rooms and the bathroom along the corridor, but she hung around without doing anything (scene 2). Case 4 also entered others’ rooms while wandering, but did nothing (scene 1). Case 5 entered the pantry while wandering, but when the staff held her shoulders directing her toward the door of the pantry, she did not resist and began to walk as directed by the staff, as if she had no will of her own (scene 4). On the other hand, case 2 suddenly stood up from a chair in the dining room, saying, “I am sorry, I will go out for a while. Please wait.” She then began to wander along the corridor (scene 3). Case 3 nodded at what another inpatient sitting at the same table said, as if she was listening to him/her, but then suddenly got up and began to wander (scene 4). These actions initially seemed to have some purpose, but once the participants began to wander, their appearance was always the same. In addition, all the participants who had not passed the self-evaluation tasks, including these 2 participants, wandered even at night, and it is speculated that they might have lost their sense of time. A sense of time cannot exist if the ability to stand outside the present time and look back at the self is lost. 36 When healthy people talk with others, images unrelated to the talk sometimes enter their minds. However, healthy people have the ability to stand outside the present time and to look back at themselves and can distinguish images of past events from those of current events. Therefore, their actions are not induced by images of past events. However, if one’s sense of time is lost, one’s actions can be induced by images of past events. The unexpected words and actions of these 2 participants were thought to have been triggered by images of past events, but since these images soon disappeared, the participants soon resumed their wandering as usual.
Conclusion
Purposeless activity, purposeful actions, irritation, and symptoms of depression have been considered as the conditions associated with wandering. 4 When one becomes unable to estimate one’s own mind (loss of theory of mind), one loses the purpose of wandering. On the other hand, while one is aware of one’s decrease in intellectual functions, the emotions of pride and shame are retained. Therefore, wandering could be caused by irritation or depression and anxiety. When one becomes unable to self-evaluate, not only is the purpose of wandering lost but the person also becomes unaware of his or her own decrease in intellectual functions, resulting in a marked decrease in the sense of pride and shame. Therefore, one becomes unable to show persistent irritation and anxiety. As a result, wandering caused by irritation or depression and anxiety is unlikely to occur.
Moreover, the model of this article is based on the lower levels of self-awareness. Therefore, we think that there is little cultural difference in the content discussed in the article. In addition, the assessment of self-evaluation is practicable in any country, when assessments are created in the same process as this article made.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.