
Abstract
Historically, minority groups have been underrepresented in research and clinical trials. The lack of participation by minorities has been attributed to a variety of factors including a mistrust of the predominately white research establishments and a lack of education about the purpose of research. The current study was designed to determine African American interest in Alzheimer’s disease (AD) research and to recruit African Americans as normal controls in current AD studies with the goal of eventually gaining consent for brain donation upon death. Participants were 46 African Americans aged 65 or older, who were interviewed about the knowledge of medical procedures and experience with research. After initial recruitment interviews, 31.7% of participants agreed to yearly testing with eventual brain donation. Study findings suggest a moderate relationship between participants' knowledge of medical procedures used to prolong life and willingness to donate one’s brain.
Recruiting participants for research and medical studies is one of the most difficult and challenging phases of the research process. While consent rates are low in general, they are particularly low among ethnic minorities and the elderly individuals. Historically, people of color and the elderly individuals have been consistently underrepresented in health-related studies and clinical trials. 1 An analysis of data gathered by researchers for the National Institute on Aging, the Alzheimer Disease Cooperative Study, and pharmaceutical companies revealed that only 3.6% of the sample population represented nonwhite participants. 2 This lack of participation has been attributed to a variety of factors that include a mistrust of the predominately white research establishment with its well-documented history of medical abuse, differing cultural attitudes and beliefs toward research and illness, isolation of older individuals, and a lack of education about the purpose of research in general and the informed consent process in particular. 1,3–5
In recent years, there has been a push to investigate and improve upon minority recruitment strategies. The National Institutes of Health (NIH) now mandates that investigators list participant demographics (including ethnicity), relate the sample population to the overall population of interest, and explain any incongruence. National Institutes of Health funding can be withheld if strategies focusing on the enrollment of ethnic minorities and women are not included. 6 Recruitment and retention of ethnic minorities in research is necessary because underrepresentation of minorities can jeopardize the ability of a study to generalize outcomes and results. In order for meaningful statistical analyses and generalizability of results, the sample populations must adequately represent the diversity and ethnicity of the population as a whole. Participation in medical research is becoming increasingly important for African Americans as a number of diseases such as Alzheimer's, some forms of cancer, hypertension, and heart failure disproportionately affect this population. Furthermore, documented differences in health care outcomes exist for African Americans and Caucasian Americans in terms of epidemiology of disease, clinical presentation, and response to treatments. 7 Therefore, continuing research with minorities should be conducted to improve our understanding of variables that influence the prevalence of such diseases across ethnic groups. Such research is also beneficial and necessary in assessing the safety and efficacy of new pharmacological treatments for diverse populations.
The need for greater inclusion of minorities in medical-related research has resulted in a growing body of literature that addresses minority perceptions of research, beliefs and attitudes toward research investigators and research personnel, and successful recruitment and retention strategies. In order to improve African American recruitment and retention rates in medical research, an examination of the specific barriers to gaining consent is necessary. In focus group interviews conducted in 1997 by Corbie-Smith, Thomas, Williams, and Moody-Ayers, 3 African Americans reported a general distrust of the medical community as the principal barrier to participation. African American focus group participants voiced concerns that they would not benefit from research findings even if they participated, citing the Tuskegee Syphilis Study as evidence of past medical abuse and unethical treatment of minorities. Likewise, discussion of the Tuskegee Syphilis Study revealed concerns by the black community that researchers would take advantage of them to obtain meaningful results for scientific publications. 1,3 Research by Mason, 4 Stahl and Vasquez, 5 and Moreno-John et al 8 suggests similar findings. In a review of these studies, African Americans consistently reported a lack of trust in research and research personnel. In general, African Americans were more likely than Caucasian participants to assume researchers would expose them to unnecessary risks and conceal important information from them.
Aside from the fear of being medically exploited and treated like a “guinea pig,” research also suggests that older African Americans may have a limited understanding of the informed consent process. 3 Corbie-Smith and her colleagues discovered that almost all focus group participants believed the informed consent form was designed to protect researchers from any legal responsibility and took away the participant’s legal rights in the event of a research mishap. This attitude can have a negative effect on the research process and can make fostering trust and building rapport extremely difficult. Research from Moreno-John et al 8 substantiates this finding, while suggesting that the medical and legal terminology often used in consent forms may create unnecessary confusion and reinforce existing misconceptions.
Research also indicates that African Americans may decline to participate in medical studies because of their cultural beliefs about illness and the natural course of aging. For example, African Americans may view dementia and other forms of cognitive impairment as a normal part of the aging process. 1 Likewise, African Americans may fail to see the need for healthy participants in Alzheimer's disease (AD) research, as many report a lack of information about such disorders. Finally, African Americans may simply not be aware of research opportunities or the benefits of research participation. 1
Recently, researchers have begun to focus attention on better understanding the reasons for low participation in research, and their findings suggest solutions to boosting recruitment numbers. Numerous studies describe the advantage of openly acknowledging issues of distrust. 1,3–4,6,9 Research suggests that honest and direct communication about the risks and benefits of study participation may be the most powerful recruitment technique. In Corbie-Smith’s 1997 focus group study, the need for more honest communication by physicians and research staff and complete information about the risks and benefits of the study were repeatedly suggested when participants were asked how to improve recruitment. Potential research participants want to know exactly what they are being asked to do in clear language from a variety of sources. 3 Video presentations along with written information provided on the consent form and verbal instructions from research personnel were well received. Participants consistently reported that a full knowledge of the procedures, expectations, and available alternatives was needed to reduce their apprehension and to build trust. In addition to information regarding the research study, African Americans reported that background information about the researchers directing the study, including their credentials, increased participation. Allowing time for potential participants to talk with family and physicians about the study also improved participation rates. 6
Brown and Alexander 10 suggest face-to-face in-person contact to establish rapport and demonstrate a genuine interest in potential participants. This in-person contact often decreased the feeling of being “just another guinea pig in a science experiment,” a feeling that many African Americans cite for declining study participation. Meeting potential participants in community centers, churches, public health facilities, their homes, and other familiar settings in the neighborhood may foster respect by demonstrating a willingness to accommodate by the research team. 4 Meeting participants in convenient, familiar locations communicates concern for the individual, and it conveys a welcoming message to a population that has long been stigmatized and discriminated against. 4 Meeting participants in locations convenient to them also addresses another barrier to recruitment: accessibility. Offering a flexible schedule and providing transportation if needed eliminates the stress of traveling to clinic sites, a reason many older individuals often give for declining participation. 7
Making each participant feel involved, valued, and respected throughout all phases of research requires that research personnel follow-up with participants regularly and communicate results and outcomes in a timely manner. Such follow-up activities aid in demonstrating how findings are beneficial and relevant to the African American community, and they convey appreciation for participation. 7
Singhal and Rogers 11 propose a theoretical model of “entertainment education” which works by combining entertainment forms with educational messages. Fritsch et al 9 conducted a study in which theater pieces were used to educate African Americans about concepts related to AD and social issues related to research participation. Presenting education within an entertainment venue allows audience members to focus on main themes and messages while identifying with characters who may serve as role models. Using this model, Fritsch and his colleagues presented 3 plays that demonstrated the daily struggles of African Americans living with AD. All plays were written, produced, and performed by African Americans. Results from this research showed a significant increase in minority recruitment when the plays were shown to African American audiences. These findings suggest that sensitivity to ethnic and cultural issues, coupled with social learning via the media, is capable of increasing minority participation. 9
In another study, Bachman et al 7 used public health care facilities in black communities to reach African Americans for participation in AD research studies. Because potential participants were approached while they sought routine treatment in a familiar setting by medical personnel with whom they had an established relationship, the authors hypothesized lower levels of distrust and increased participation. Results supported this hypothesis as an effective strategy for enrolling African Americans into AD research. The authors of this study, along with others, suggest fostering strong community involvement through outreach programs and maintaining good relations with prominent community groups and leaders may provide credibility to research studies. Community involvement may be especially helpful when discussing sensitive issues such as advanced directives and brain donation preferences. 12 Research by Mason 4 and Moreno-John et al 8 supports the importance of community-based recruitment strategies. Both propose an active and collaborative effort with church officials, senior ministries, and community advisory boards to build trust between the black community and the research team so that health and medical education becomes a prominent cultural and social issue. When possible, Moreno-John et al advises incorporating ethnic values and practices into research protocols and recruitment. For example, the importance of religious beliefs and family decision making for African Americans should be considered in protocol development. Likewise, employing researcher staff with similar racial and ethnic backgrounds to those targeted for recruitment may facilitate enrollment.
Related to AD research, participation is the sensitive topic of brain tissue donation. Consent from African American participants for brain donation and autopsy remains a particularly challenging obstacle for dementia researchers. Autopsy and neuropathological studies of patients with AD are typically completed to confirm the clinical diagnosis. 12 Brain autopsy can also provide essential tissue samples for research.
Research by Bonner et al 12 identified the following obstacles to brain donation by African Americans: religious beliefs, preexisting notions about autopsies, family disagreement, concerns with viewing the body and funeral arrangements, and inadequate and inaccurate information on autopsy. In an effort to reduce these barriers, Bonner and her colleagues implemented a 2.5-year recruitment program that relied on face-to-face discussions with caregivers about postmortem treatment preferences. Their discussions focused on developing trust by employing empathetic listening when talking about sensitive topics, offering assistance with acquiring health services, and providing 24-hour accessibility to researchers. Caregivers who expressed mistrust or had negative views about brain donation were not approached further after initial interviews were conducted. Caregivers who were positive about autopsy during the initial interviews were followed for the duration of the study and encouraged to consider brain donation for their loved one. Two face-to-face interviews and a telephone call were completed each year to maintain contact with participants during the study. At the end of her study, Bonner reported an autopsy completion rate of 29%, a rate nearly 7 times greater than the reported rate prior to her study. She credits her success to culturally sensitive methods that allowed for the development of trust.
The current study was based on this earlier work by Dr Gloria Bonner who also assisted in the development of the University of Kentucky research protocol. The Kentucky study was implemented after 3 years of working with African American religious and community leaders to increase awareness of AD and develop mutual trust. In keeping with Dr Bonner’s research on variables associated with increased brain donation, we implemented a scripted interview that emphasized empathetic listening and building rapport by discussing sensitive topics prior to bringing up the topic of brain donation. Our study had 2 major purposes (1) to determine African American interest in AD research participation and (2) to recruit African Americans as healthy controls into current AD studies with the intent of eventually gaining consent for brain tissue donation upon death.
Methods
Participants
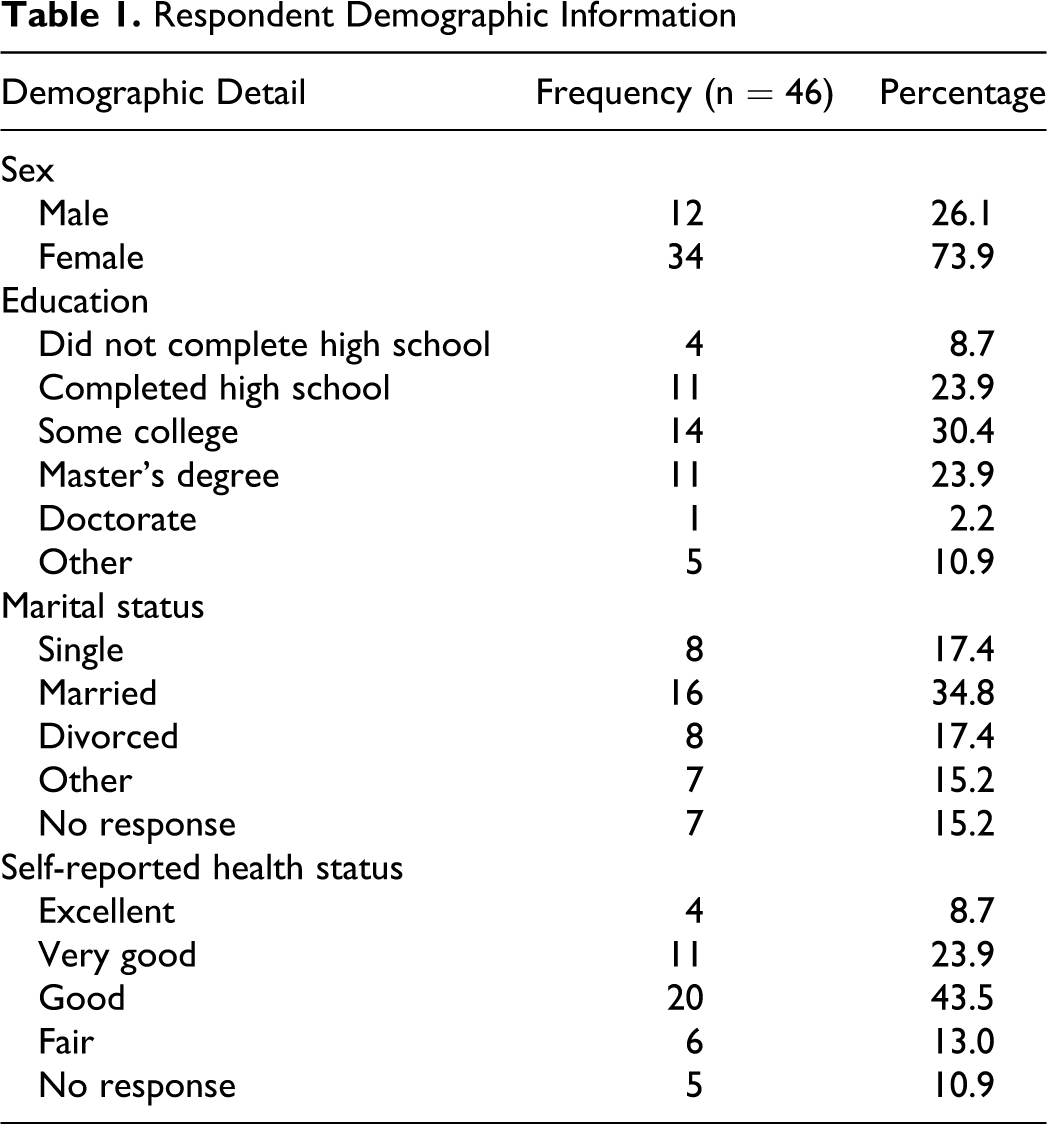
Research participants were 46 African Americans aged 65 or older and recruited from a database of registered voters available at the Sanders-Brown Center on Aging in Lexington, Kentucky. To be included in the community database, registered voters aged 65 and older from the county responded to a letter asking for participants for studies of aging to be conducted at the University of Kentucky. Responses were obtained from approximately 13% of those contacted. For this study, we selected individuals who identified themselves as African American, 7% of those who responded. Telephone contact was made by trained interviewers to determine interest in the study and to schedule an interview time. Interviewers followed a scripted discussion for each telephone contact. Seventy-four percent (n = 34) of the individuals contacted by telephone, who agreed to be interviewed were female. See Table 1 for complete demographics.
Respondent Demographic Information
Procedure
Two trained interviewers, at least one of whom was African American, completed the semistructured in-home interview with study participants. Interviews took 30 to 60 minutes depending on how much the participant wanted to share. One interviewer conducted the interview with the other taking notes. After arriving at the home of the participant, the interviewer described the study and obtained a written informed consent. The first part of the interview provides background information about the University of Kentucky Sanders-Brown Center on Aging, the Alzheimer’s Disease Center, and the on-going efforts of scientists at the Center toward finding a cure for AD and providing support to families coping with the disease. Next, the participants were asked about their personal experience with health and medical procedures, their feelings about research, and their interest in participating in annual memory and cognitive screenings, and willingness to donate brain tissue to AD research. Finally, if interested in participating, medical history information was collected to confirm study eligibility.
Health Experience and Medical Procedure Questions
Each participant was asked questions about their familiarity with specific medical procedures (magnetic resonance imaging [MRI], mechanical ventilation, tube feeding, and autopsy examination). For each procedure, the following questions were asked in sequential order: the purpose of each procedure, personal experience with the procedures, and the likelihood of using the procedures if it was deemed necessary by their current family physician. If a participant was unfamiliar with a procedure, the interviewer provided a brief explanation, and the participant was given the chance to answer again about whether or not they would consent to having the procedure done if recommended by their physician. Answers regarding familiarity with procedures were given in a yes or no format, while likelihood to use a procedure was answered in a Likert-type scale with 1 being yes, definitely and 5 being no, would not. At the conclusion of the interview, a fact sheet describing the medical procedures was left with the participant. Leaving information with the participant was based on earlier work by Dr Bonner that found sharing information with participants reduced feelings of power differential that often accompany participant mistrust. 13
Research Participation Questions
Questions in this section asked for the participant’s general thoughts and feelings about research participation. Participants were asked what research meant to them, including any benefits or drawbacks, whether they or a family member had participated in research, whether they were currently interested in participating in research and why, and whether there was anything about a particular study that would either increase or decrease their chances of participating. Any answer yes was followed by a request for more detail. More specifically, if they answered that they or a family member had participated in prior research, they were asked to explain the study, when it took place, whether it was a good or bad experience, and how they would rate the experience on a Likert-type scale, with 1 being extremely good and 5 being extremely bad.
Healthy Aging Research Questions
The interviewer explained that the current group of normal controls being followed at the University of Kentucky consists of approximately 500 persons aged 65 and older but had included only a small number of African Americans. The importance of studying older healthy African Americans was explained, and participants were asked whether this research was of interest to them. For those who answered no or don’t know, an explanation for declining was requested.
For those individuals who expressed an interest in participation, the research was described as a program dedicated to the study of healthy older persons for comparison to patients exhibiting memory and thinking problems. Interviewers explained that involvement in this research required annual evaluations of memory and cognitive performance. If participants were willing to be followed, inclusion criteria were reviewed. Inclusion criteria include the availability of an informant or family member to provide necessary information. Brain donation is not a requirement for participation and was brought up only if the interviewer felt that the participant would be comfortable with this topic. This decision by the interviewer was based on whether adequate rapport had been established and whether the participant’s expressed attitudes about research were perceived as positive. In addition, exclusion criteria were also reviewed. Participants were ineligible to participate if they had any major medical illness or injuries affecting their brain health or if they had a history of substance abuse. After the inclusion and exclusion criteria were reviewed, participants were thanked for their time, and if they were eligible and agreed, told that they would be contacted in the next few weeks to schedule testing and the initial physical exam.
Autopsy and Brain Donation Questions
As part of the inclusion criteria, autopsy and brain tissue donation were discussed only if the interviewer considered the participant to be comfortable with the topic. Observed level of rapport, verbalized attitudes and beliefs, nonverbal responses during the interview, knowledge and interest in medical procedures, and overall openness to research influenced whether or not participants were asked.
Data Analysis
Collected data were analyzed using exploratory data analysis and bivariate analysis. Specifically, correlation tests and Fisher exact test were performed to examine the relationship between variables and consent to brain donation. P values <.05 were considered significant.
Results
Forty-six participants completed the initial interview. Most study participants were familiar with the medical procedures discussed in the interview. See Table 2 for complete list of results. Those who were familiar with the procedures were asked to define the procedures in their own words. For example, 1 participant defined an MRI as “something used to look inside, like an x-ray.” One participant defined mechanical ventilation as “life support,” while another participant defined it as “a breathing machine … where a patient has a pulse but is not alive.” To explain the purpose of a feeding tube, 1 participant said, “when they put that tube down into your stomach so you can get food.” Likewise, most participants defined an autopsy as “to see what you died of.”
Respondent Familiarity With Procedures
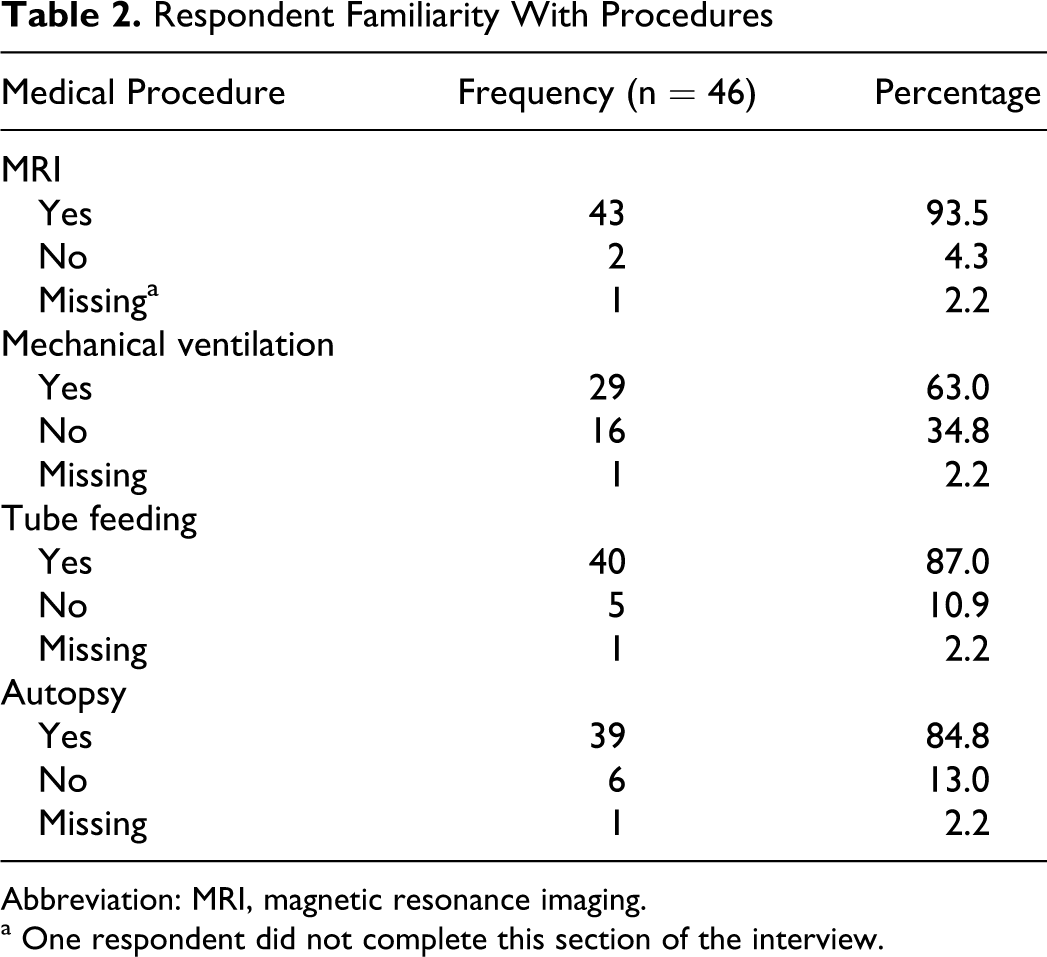
Abbreviation: MRI, magnetic resonance imaging.
a One respondent did not complete this section of the interview.
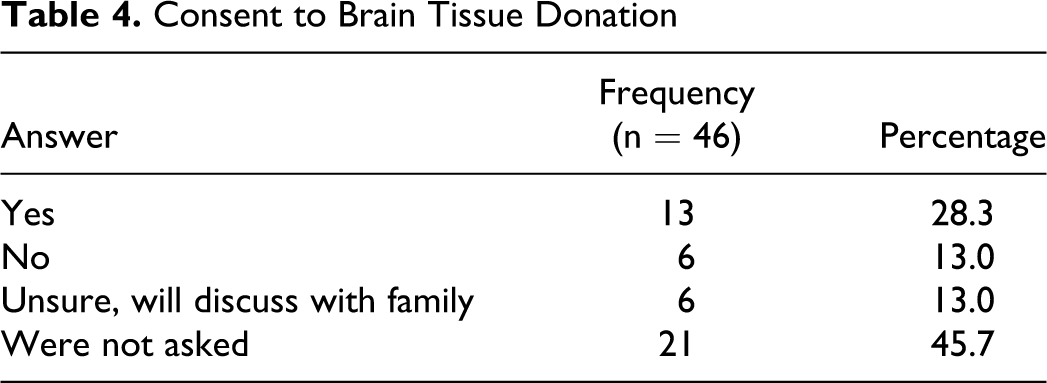
After being educated about each procedure’s use, 95.5% (n = 42) answered yes, definitely when asked whether they would trust their physician’s order to have an MRI done. Likewise, 54.5% (n = 24) would agree to mechanical ventilation, 61.4% (n = 27) would agree to tube feeding, and 75.0% (n = 33) said yes, definitely to having an autopsy performed postmortem. When asked for consent to brain tissue donation, 28.3% (n = 13) answered yes, while 13% (n = 6) answered no. The remainder of the participants, 58.7% (n = 27), were unsure or were not asked about brain tissue donation because they declined to be followed yearly or the interviewer did not feel it was appropriate. See Tables 3 and 4 for a complete list of these results.
Respondent Hypothetical Consent to Procedure
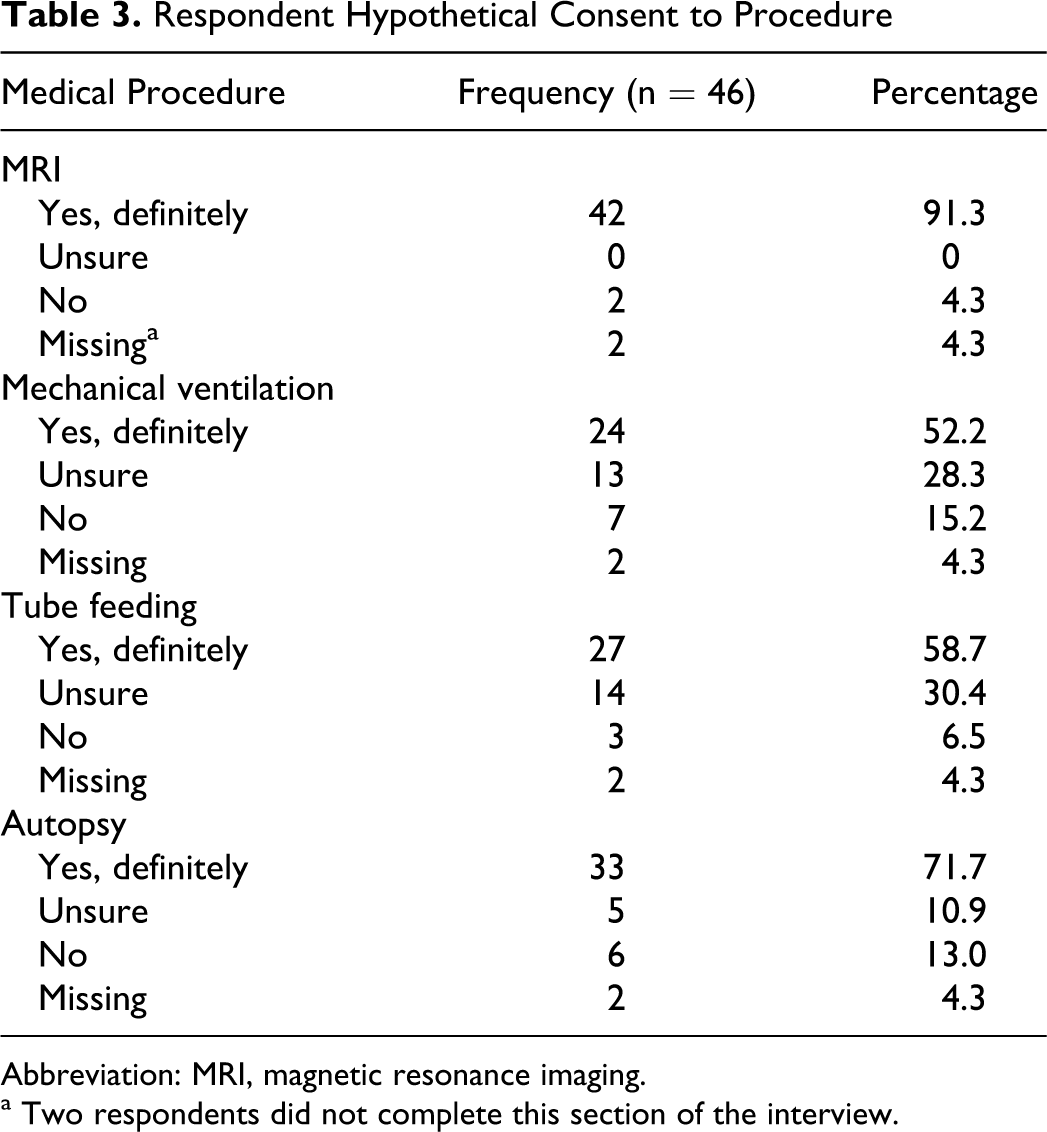
Abbreviation: MRI, magnetic resonance imaging.
a Two respondents did not complete this section of the interview.
Consent to Brain Tissue Donation
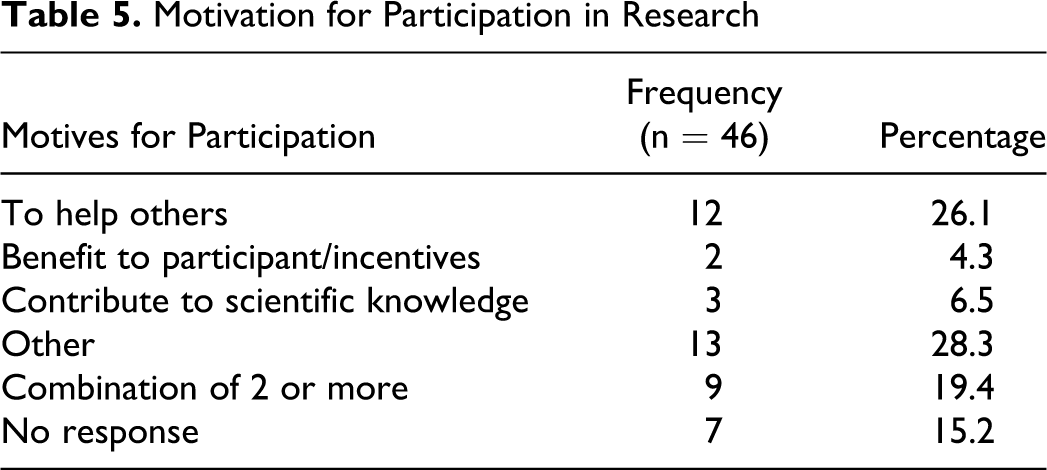
When examining motives for participation, most participants were interested in research participation for altruistic reasons. Indeed, 30.8% (n = 12) of participants reported answers that fell under the heading of “to help others,” while 7.7% (n = 3) cited reasons that fell under the heading of “to increase scientific knowledge.” Lastly, 5.1% (n = 2) cited “participation incentives” such as money or free medical services as the primary motive. The remainder of participants cited “other” or a combination of the reasons listed above. See Table 5 for a complete summary of results.
Motivation for Participation in Research
In order to investigate the relationships between variables, correlation analyses were conducted for variables based on familiarity with each medical procedure and brain donation. Tests suggest a significant relationship between reported consent to autopsy based on physician recommendation and consent for brain donation, as r = .44, P = .003. The strength of this relationship is moderate, indicating a positive correlation between hypothetical consent to an autopsy and consent to brain donation as part of the current study. A significant moderate relationship was also found between hypothetical consent for mechanical ventilation and consent to brain donation, as r = .40, P = .008. Furthermore, Fisher exact test also confirmed a significant relationship (P =.017, Fisher exact test) between hypothetical consent to mechanical ventilation based on doctor’s recommendations and consent to brain tissue donation. However, no relationship was found between a family history of dementia and consent to brain donation r = .156, P = .401. Similarly, statistical analysis did not indicate a relationship between previous research participation and consent to brain tissue donation.
After initially consenting to participate in the recruitment interview, 6 individuals did not agree to being followed annually. Therefore, of the 46 initially contacted to be interviewed, 40 healthy, African American participants are presently being followed and tested annually. Thirteen have consented to brain tissue donation, while 27 have not, making the current donation consent rate 31.7%. To date, 2 deaths have occurred, with 1 autopsy completed, yielding a 50% autopsy completion rate with this group.
Summary and Discussion
The historically low recruitment and retention rates of persons of color into health-related research and clinical trials remains an issue for medical researchers. This lack of participation has been attributed to a variety of factors that include a mistrust of the medical establishment, differing cultural attitudes and beliefs toward research and illness, the common misconception that research findings are typically biased to be advantageous to white populations only, and a lack of education about the general purpose of research. However, participation in medical research is becoming increasingly important for African Americans because a number of diseases, including AD, disproportionately affect this population. 7
Past data from focus groups conducted by Corbie-Smith strongly support the importance of full disclosure when presenting research opportunities. Likewise, face-to-face, in-person strategies that demonstrate genuine regard for potential participants has been linked to increased African American participation. Meeting potential participants in community centers, churches, public health facilities, their homes, and other familiar settings in the neighborhood have been found to foster the building of respect and communicate concern for the individual. Offering a flexible schedule and providing transportation if necessary has also been cited as useful. 7
The present study contributes information that may aid in understanding current trends in African American research participation and brain donation. Forty-six African Americans were interviewed in person regarding their knowledge of medical procedures, views on research, motives for participation, potential reasons for withdrawing from research, and willingness to donate their brain tissue upon death.
The importance of establishing rapport and being aware of cultural preferences is essential when asking for consent to brain donation and postmortem tissue examination. 12 In the current study, research was not conducted until trust between key African American stakeholders and the researchers had been established. Study findings suggest a moderate relationship between participant’s knowledge of certain medical procedures frequently used to prolong life and willingness to donate one’s brain. That is, being familiar with and hypothetically consenting to life support treatments—mechanical ventilation in particular—had a statistically significant relationship to brain tissue donation consent. Studies conducted by Kwak and Haley 14 and Phipps et al 15 support the idea that African Americans are more likely than other ethnic groups to prefer the use of life support measures at end of life. Work by Waters 16 suggests that such preferences are a direct result of enduring mistrust (from the Tuskegee Syphilis Study) and negative experiences with the medical community. Many African Americans voiced concern at signing a legally binding contract—which may include consent to brain donation and autopsy—that might restrict health care choices at end of life or place power in the hands of medical personnel whom they did not trust. Knowledge of and preference for the use of all possible end-of-life treatments may illustrate how African Americans combat the fear of being medically exploited or as 1 participant puts it “signing my life away.” While tube feeding may be considered a life support procedure, it is often used when there is no immediate threat of death, while mechanical ventilation may suggest a more aggressive approach to sustaining life. African Americans are more likely than other ethnic populations to endorse the use of all life support measures, especially the most aggressive ones. 14 This finding may help to explain why mechanical ventilation was significantly related to brain donation while tube feeding was not. Future studies designed to increase African American research participation that includes brain donation should consider incorporating information and education that acknowledges the importance of using all possible measures to prolong life as one way to foster trust and reassure those skeptical of agreeing to postmortem procedures.
We consider our brain donation consent rate of 31.7% after one interview a major accomplishment, as African Americans are nationally underrepresented in brain donation programs when compared with their Caucasian counterparts. 12 We believe our commitment to establishing rapport and trust via empathic listening and thoughtful discussion of medical procedures related to end-of-life treatments contributed to this higher than expected consent rate. For those participants who were unsure of brain donation or were not asked about brain donation during the recruitment interview because of perceived apprehension of the subject matter, the topic will be revisited at the next yearly testing visit. Additional time will allow the family to discuss this possibility and enable greater rapport and trust to be established with our medical research staff. We expect that with greater time, rapport, and experience with research, more of our participants will agree to brain donation as part of their research participation. Although Bonner’s research found “maybes” were usually “no,” we expect at least some of our “maybes” will change to “yes.”
Brain donation is in no way a requirement for participation in this study, and while we are pleased with our consent rate and hope to encourage others to consider the option, our primary focus remains increasing African American participation in AD research. Regardless of donation status, all study participants will undergo fairly invasive procedures in the form of annual memory and cognition tests and physical examinations that include blood draw. That we successfully recruited 40 African American individuals into a study that requires such a commitment provides additional support to recruitment strategies emphasizing trust, respect, and honesty when providing the risks and benefits to research participation.
This study examined relationships between knowledge of and consent to medical procedures and AD research, including possible brain donation upon death. Surprisingly, there was no significant relationship between a family history of AD and willingness to participate in research. It is possible that our small sample size may have minimized this effect. Given that many of the participants in this study cited helping others as the main reason for research participation, future studies investigating recruitment may want to incorporate material that illustrates the community benefits of research participation as well as brain donation.
This study is limited by its sample size, which may not be representative of the larger population. For example, our participants were all from Lexington, and they all had incomes above poverty level. They were also well educated, with most having some college experience. The larger number of women participants may reflect the larger number of African American women who are interested in research participation. Perhaps women are more regularly exposed to research and recognize its value and benefits. While the sample is more educated than one would expect of the larger population, we think everyone can benefit from knowledge of medical procedures and research regardless of their educational history. Likewise, trust developed between the community and researchers is beneficial to all. Clearly, the sample used in this study is biased to ensure a relative amount of success in this challenging research. However, greater diversity in the African American sample would be valuable in future studies. Lastly, the mean age of our cohort is 74. However, because all participants must be relatively healthy to participate as a “normal control,” we expect fewer deaths when compared to cohorts comprising those with mild cognitive impairment or advanced dementia. Therefore, our brain autopsy completion rate should be interpreted by keeping this in mind.
We recognize that the establishment and maintenance of trust and rapport is key to the successful recruitment and retention of African Americans in research. In the present study, trust and rapport were established and maintained through (1) face-to-face interviews in a community setting of the participant’s choice, (2) supportive discussion of sensitive material pertaining to end-of-life care, and (3) exchange of health information with participants to reduce feelings of power differential. Our findings suggest that recruitment strategies grounded in building rapport may be most beneficial when implemented within the framework of certain cultural preferences that reflect strong community ties, family-based decision making, and the importance of using all possible measures to prolong life.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed the receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this work was provided through an NIH Administrative Supplement to Grant AG0 28383.