
Abstract
The purpose of this study was to evaluate a popular measure of Alzheimer’s disease (AD) memory and behavior problems and to determine whether its aggressive behavior items coalesced empirically as a subscale to form a psychometrically viable AD aggression measure for clinicians. Data from self-report questionnaires were examined from 419 informal AD caregivers in the southern United States. Principal axis factoring revealed a unidimensional solution with robust item loadings on the single factor. Three forms of reliability analysis indicated moderately strong internal consistency on this proposed measure. Evidence of convergent validity analysis was suggested via the measure’s significant correlations to theoretically linked constructs. The proposed measure emerged as a reliable and valid tool for health care practitioners for the appraisal of problematic AD aggression behaviors from the caregiver perspective.
Introduction
Providing informal, or unpaid, care for an individual diagnosed with Alzheimer’s disease (AD) is typically extremely burdensome. In its early stage, the insidious nature of AD may cause the caregiver to question whether the family member is ill at all. 1 As the disease progresses, however, caregivers must adjust to the care recipient’s increasing level of disability, which runs parallel to the caregiver’s sense of burden. 2 An important factor shown to contribute to caregiver burden is aggressive behavior from the care recipient, or AD aggression. 3
Understanding AD Aggression
Alzheimer’s disease aggression in early-stage dementia is fairly uncommon. The prevalence and frequency of aggressive behavior tends to rise as the impairment worsens and then decline only in the most severe stage.1,4–6Aggression usually appears in the middle to late stages of AD, though not every individual with AD presents signs of aggression. 7 The treatment of AD aggression utilizes pharmacological and onpharmacological interventions. Physicians prescribe atypical antipsychotics or neuroleptics most frequently, though pharmacological effects include Parkinsonism, weight gain, sedation, cardiovascular complications, and even death.8,9 Nonpharmacological approaches include environmental changes, behavioral therapy, and caregiver training. 7 While many techniques show promise in alleviating psychological and behavioral symptoms in dementia, few specifically target aggression. 10
Alzheimer’s disease aggression is deemed a behavioral manifestation of psychological symptoms of dementia,11–15and research demonstrates that many individual traits trigger aggressive behavior. The most common characteristics of individuals with aggression are impaired cognitive and motor ability.7,11,16 Other internal factors that strongly correlated with AD aggression include comorbidities, such as mental illness and alcoholism, and the presence of significant pain, especially when the care recipient has difficulty in verbally communicating physical discomfort.17–20 Environment also plays an important role in AD aggression as certain external factors, such as noise or use of restraints, can increase the likelihood of aggression. 7 Studies show that intimate caregiving is the most common environmental trigger of aggression in individuals with dementia.21,22 Intimate caregiving, which entails helping with many activities of daily living such as bathing, dressing, and toileting, becomes necessary as the care recipient’s impairment worsens. 21 However, the frustration the care recipient feels due to the inability to complete these personal tasks and the intrusive nature of the related care may contribute to AD aggression.
Aggression in AD individuals can manifest as physical or verbal, active or passive. Examples of active verbal aggression include speaking in an aggressive or angry way, or verbally threatening another individual. 22 Active physical aggression can present in the form of hitting, pushing, kicking, slapping, or spitting. 22 Examples of passive aggression in AD individuals include refusing to speak or move. 23 The current study focuses on instances of active aggression.
Alzheimer’s disease aggression amplifies psychological distress for the caregiver and contributes greatly to caregiver burden.3,6 Of many behavioral disturbances related to AD, including irritability, apathy, and sleep and appetite disruption, caregivers report higher distress in the presence of aggression. 12 VandeWeerd and Paveza found that caregivers of verbally aggressive elders were 8 times more likely to be verbally aggressive toward care recipients. 24 Research shows that aggressive behavior negatively affects female caregivers more than male caregivers.3,25 The probability that females provide intimate care more often than males offers a possible explanation for the gender difference. 25
Alzheimer’s disease aggression has been cited as the leading factor in the caregiver’s decision to institutionalize the care recipient.3,26 These studies highlight not only the impact of AD aggression on caregiver burden but also the urgent need for health care practitioners to provide intervention techniques and support predicated on the identification of AD aggression. The aim of this study is to propose and empirically evaluate a potential measure of AD aggression embedded within a commonly used assessment tool for AD problem behaviors, the Revised Memory and Behavior Problems Checklist (RMBPC). 15
Proposed AD Aggression Measure
The 24-item RMBPC was originally designed to demonstrate the importance of education and training in the management of behavioral problems to alleviate caregiver burden.15,27 It is a self-administered checklist that measures the frequency of and caregiver’s emotional response to the care recipient’s bothersome behaviors. The items are aggregated via behaviors related to memory, depression, and disruption. Teri et al emphasized these behavioral aggregates because of their importance and prevalence in patients with dementia. 15
The current study examines the verbal and physical aggression items of the RMBPC. The 4 items address property destruction, dangerous behavior toward self or others, threats to hurt others, and verbal aggression.15(p625) Destroying property is a physically aggressive behavior and is often associated with tearing things, such as pages out of books, in individuals with dementia.19,20,28 The item referring to dangerous behavior may broadly include symptoms of physical aggression, such as hitting, kicking, and throwing objects.22,29 It can also include self-destructive behavior, such as cutting or hitting oneself, and repeated removal of essential medical equipment (eg, tubes and catheters). 30 Threatening to harm others may refer to verbal and/or physical aggression and includes verbal attacks or intimidation, name calling, raising a fist, and standing in an aggressive posture. 31 Verbal aggression may include yelling, screaming, and/or cursing and is the most common form of aggression observed in individuals with dementia.22,29 The RMBPC assesses the frequency of these behaviors and their negative impact on the caregiver, that is, the extent to which the behaviors bother the caregiver. This study focuses on the psychometric properties of a scale that measures the negative impact of AD aggression from the caregiver perspective. For validity analysis purposes, the concept of AD aggression is viewed through the lens of the Pearlin Stress Process Model. 32
Conceptual Framework
The Pearlin Stress Process Model (PSPM), one of the most influential theoretical models in the realm of caregiver research, offers a paradigm on how the stress and burden of caregiving affects the psychological and physical well-being of the caregiver. 33 The generic model consists of 4 key elements: a primary stressor; a secondary stressor proportionally related from the primary stressor; a health/well-being outcome that is often negatively affected by the stressor/stressors; and a moderator that buffers the deleterious effect of the stressor/stressors on the outcome.32,34 Figure 1 illustrates the generic PSPM.
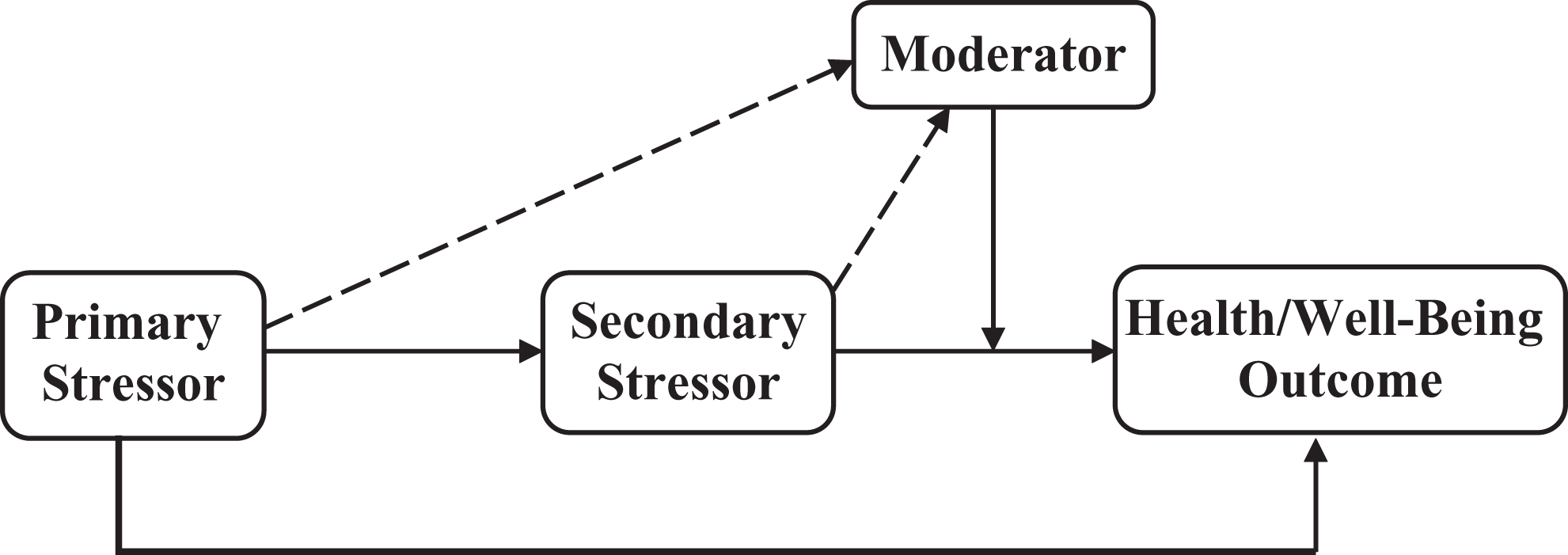
Generic Pearlin stress process model (moderating). Dotted line denotes a possible, significant relationship. Solid line denotes a significant relationship.
Applying to the current study, the primary stressor is AD aggression, that is, aggressive behavior from the care recipient. The secondary stressor is the caregiver’s perceived sense of burden stemming from AD aggression. The health outcome is caregiver resilience, a psychological marker of hardiness. Resilience is the ability to adapt and maintain balance when confronted with adversity (in this case, factors of caregiving burden), and the subsequent self-perceived ability to succeed when confronted with future adversity. 35 The moderator is the coping strategy typically employed by the caregiver. The current study focuses on 3 popular coping strategies: (1) task-focused, that is, seeks to perform a task in order to alleviate the problem; (2) emotion-focused, that is, seeks to regulate or alleviate distressing emotions; and (3) avoidance-focused, that is, avoids problem or situation in order to decrease stress.36,37 Figure 2 illustrates the PSPM with application to the current study.
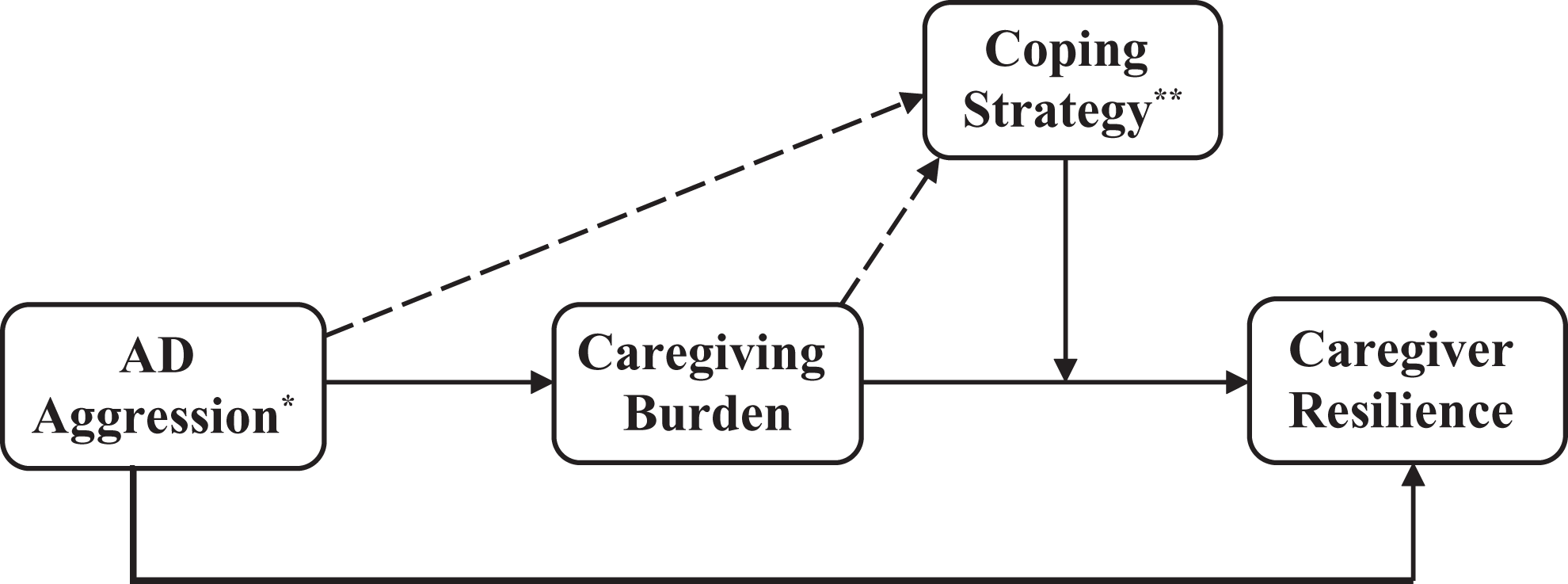
Applied Pearlin stress model to the current study. Dotted line denotes a possible, significant relationship. Solid line denotes a significant relationship. *Aggressive behavior from the care recipient diagnosed with Alzheimer’s disease. **Three different types: task-focused, emotion-focused, and avoidance-focused.
The PSPM presents a conceptual framework that is the foundation of validity analysis, as the model illustrates the theoretical links among AD aggression, caregiving burden, coping strategy, and resilience.
Research Questions
Restating the purpose, the current study is a psychometric examination of a proposed AD aggression measure, a potential subscale of the RMBPC. With this purpose in mind, the researchers formulated the following research questions that underscore 3 principal psychometric areas among the AD aggression items:
What is the underlying factor structure among these items? To what extent are the items of the proposed measure internally consistent? What is the evidence of construct validity with this proposed measure?
Methods
Design and Sampling
The study utilized cross-sectional analysis of self-reported data from AD caregivers in a metropolitan area in the southern United States. The study recruited caregivers using 2 different methods. The first method involved mailing surveys to approximately 5000 caregivers on the mailing lists of a nonprofit 501(C)3 AD service organization. The AD service organization assisted in the mail out in order to maintain confidentiality of its caregivers. The aforementioned process of confidentiality prevented the researchers from tracking with additional follow-up mailings.
The second method of recruitment addressed the African American population, the second largest group of caregivers in the United States. 38 African Americans constitute approximately half of the population in the study’s geographical focus. 39 Because many African Americans may be less likely to utilize formal support services due to perceived cultural barriers, it was important to recruit directly from this community to assure that they were appropriately represented in the study population. 40 A faculty consultant with expertise in African American caregiver research recruited participants from several African American-centered community organizations and agencies including a home health agency, adult day centers, churches, and community centers.
Caregivers were offered $10 compensation for their time and participation. Almost 700 AD caregivers submitted completed questionnaires. From this overall sample, 419 participants reporting incidence of AD aggression constituted the sample in the current study. The study was approved by Louisiana State University Institutional Review Board.
Instrumentation
Data were solicited from a self-administered questionnaire. Measures on the questionnaire germane to the current study were related to demographic and caregiver contextual factors, AD aggression (proposed measure), caregiver burden, caregiver coping strategy, and caregiver resilience.
Demographics and caregiving context
The demographic items included gender, age, ethnicity, and marital status. The caregiving context items were the caregiver’s relation to the care recipient and the stage of AD: early stage (noticeable memory loss/other cognitive deficits, yet functioning independently), middle stage (decline in mental abilities, physical functioning with increased dependence), and late stage (loss of bodily functions requiring total dependence).
Caregiver burden
The shortened, 4-item Zarit Burden Interview (S-ZBI) solicits data regarding the burdensome impact of caregiving on daily responsibilities. 41 Responses on a 5-point Likert format range from 0 = never to 4 = nearly always. Bedard et al revealed sound psychometrics on this newly revised measure. 41
Alzheimer’s disease aggression
Alzheimer’s disease aggression was assessed using the proposed subscale of the RMBPC. 15 Of the 24 behavior items on the RMBPC, this study focused on the 4 behavior items entailing aggression: property destruction, dangerous behavior to self/others, threats to others, and verbal aggression. The RMBPC asks caregivers to rate the frequency of observable behavior problems. Caregivers also rate the impact of the behaviors (how bothered they are by said behaviors) from 0 = not at all to 4 = extremely. Previous studies have reported sturdy psychometrics for the full RMBPC.15,42 The psychometric properties for the proposed AD aggression subscale are the center of the current study and are reported in the Results section.
Coping strategy
The situational Coping in Task Situations (CITS) questionnaire comprises three 9-item subscales that assess the likelihood that the individual typically engages in (1) task-focused, (2) emotion-focused, and (3) avoidance-focused strategies. 43 Item responses range from 0 = not at all to 4 = extremely. Matthews and Campbell disclosed adequate or better psychometric properties on all 3 subscales. 43
Resilience
The 14-item Resilience scale (RS-14) measures individual resilience. The format is a 7-point Likert scale ranging from 1 = disagree to 7 = agree. Items include statements such as “I can get through difficult times because I’ve experienced difficulty before” and “My life has meaning.” 44 Wagnild and Young reported the RS-14 with strong internal consistency. 44
Analytic Strategy
Descriptive statistics were reported for sample characteristics and for each item of the proposed AD aggression measure. For research question 1, principal axis factor analysis (using R2 as an estimate of common variance) was conducted to identify underlying dimensions of the AD aggression measure. The factor analyses rotated to a varimax solution with no limit on the number of potential factors. A customary minimum eigenvalue setting of 1.0 determined the number of factors retained for final solution. Minimum factor loadings 45 for item retention accorded with the following formula: 5.152/(N − 2). For research question 2, reliability of the AD aggression measure was observed via 3 methods: Cronbach α, Guttman split-half coefficient, and inter-item correlations. For research question 3, convergent validity analysis was performed in order to determine how the measure related to the other constructs in the theoretical model. These variables include global scores on the ZBI (burden), the CITS (coping), and the RS-14 (resilience). Correlations were calculated using Pearson r, as these measures are parametric.
Results
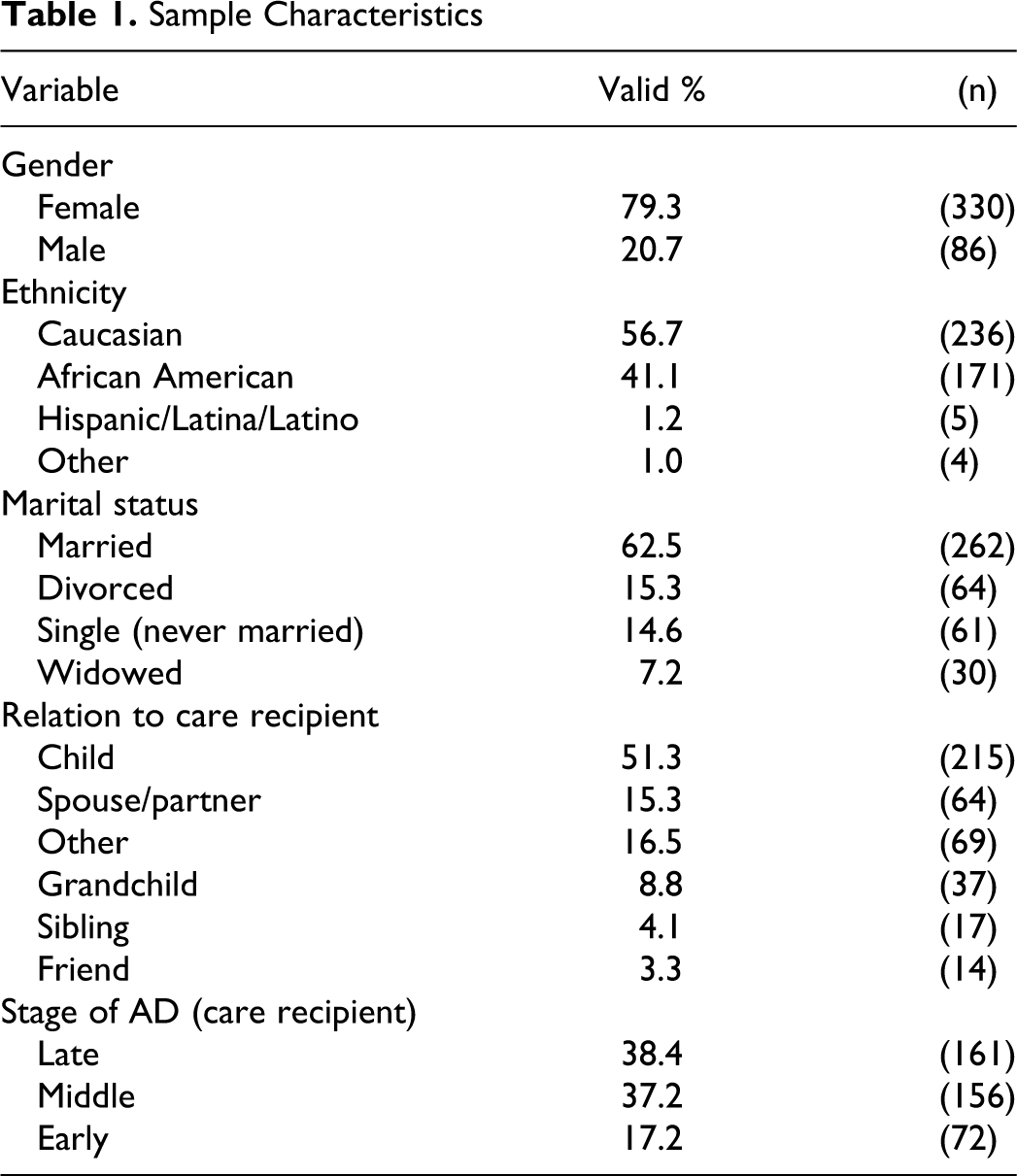
The majority of caregivers were female (79.3%, n = 330). The average age was 61 years. A slight majority of caregivers reported their ethnicity as Caucasian/white (56.7%, n = 236), with the next largest group as African American (41.1%, n = 171). The majority was married (62.5%, n = 262). Most caregivers were the adult child of care recipients (51.4%, n = 215) or described their relationship as other (16.5%, n = 69). The most common stages of AD were late stage (41.4%, n = 161) and middle stage (40.1%, n = 156). Table 1 provides the complete details of sample characteristics.
Sample Characteristics
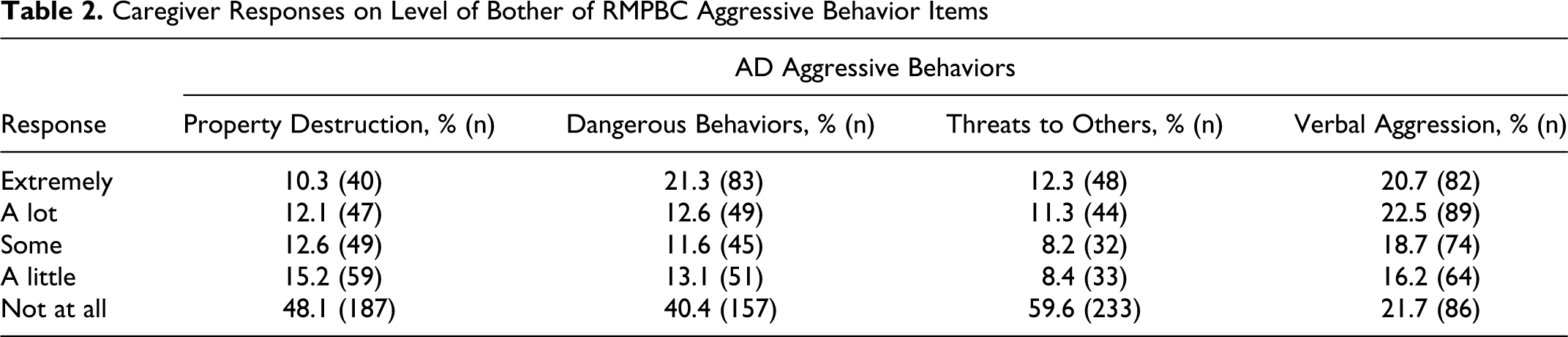
Looking at descriptive statistics on the AD aggression items, among respondents who reported occurrence on the item property destruction, approximately 10% (n = 40) were extremely bothered by this behavior, while48% (n = 187) were not at all bothered. Among those who reported occurrence on the item dangerous behaviors, approximately 21% (n = 83) of caregivers were extremely bothered by this behavior, while 40.4% (n = 157) were not bothered at all. Among those who reported occurrence on the item threats to harm others, about 12% (n = 48) reported they were extremely bothered by this behavior, while 60% (n = 233) reported they were not at all bothered. Among those who reported occurrence on the item verbal aggression, approximately 21% (n = 82) reported they were extremely bothered by this behavior, while almost 22% (n = 86) reported they were not at all bothered. Table 2 displays the frequencies and percentages of caregivers' responses to the RMBPC aggressive behavior items regarding caregiver reactions to said behaviors.
Caregiver Responses on Level of Bother of RMPBC Aggressive Behavior Items
Principal axis factoring on the proposed measure held a minimum eigenvalue of 1.0, with no limitation on the number of possible factors. One factor emerged with an eigenvalue above 1.0 (2.411) among the items, and it accounted for 60% of variation among the 4 aggression items. All items loaded strongly on the aforementioned latent factor, as follows: property destruction = 0.767, dangerous behavior = 0.837, threats to harm others = 0.818, and verbal aggression = 0.674.
For convergent validity, zero-order correlations were observed between the proposed AD aggression measure and the measures corresponding to its theoretically linked constructs in the PSPM, as previously discussed in Conceptual Framework section. Alzheimer’s disease aggression significantly, positively correlated with the ZBI (caregiver burden): r = .20, P < .01. Alzheimer’s disease aggression significantly, negatively correlated with the RS-14 (caregiver resilience): r = −.12, P < .05. Finally, AD aggression significantly correlated with 2 of the 3 caregiver coping strategies from the CITS: emotion-focused coping (r = .20, P < .01) and avoidance-focused coping (r = .34, P < .01). As expected via the PSPM framework, AD aggression was the primary stressor that significantly related to its secondary stressor, caregiver burden. The primary stressor also significantly related in an opposite direction to the framework’s health outcome, caregiver resilience. As the primary stressor increased, so did the likelihood of the caregiver’s utilization of emotion-focused and avoidance-focused coping strategies (moderators in the PSPM framework).
In terms of reliability within the measure, all interitem correlations were significant (P < .01) and are summarized in Table 3 . Items on the proposed AD aggression measure showed a Cronbach α of .78 and a Guttman split half coefficient of .73.
Interitem Correlations on Proposed AD Aggression Measure
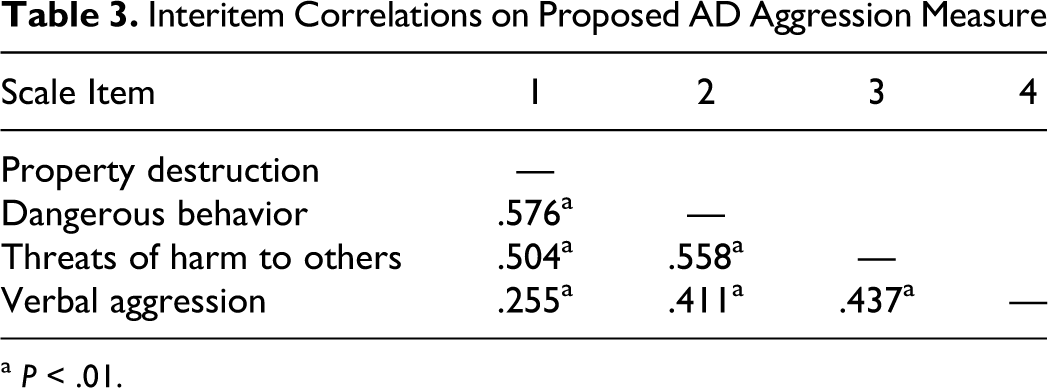
a P < .01.
Discussion
Comparability of Findings to the Previous Research
The study sample reflects the typical AD caregiver in the United States38,46: female, married, and the child of the care recipient. Ethnic groups were comparable in proportions similar to those in the study’s geographic focus. The greater percentage of female caregivers in this study (80%) compared to the general AD caregiver population (60%) may be due to sample recruitment from support groups, as women are more than twice as likely to participate in support groups as men.47,48 As expected, most in the sample reported their care recipients in the middle to late stages of AD, when aggressive behavior is most common. 7
This study’s reliability coefficients show comparable internal consistency to other RMBPC subscales in the previous studies.15,49,50 Additionally, the current study’s findings on factor loadings were higher than loadings from the same items on broader RMBPC subscales in the previous research.15,49 These factor analysis findings, along with the reliability statistics and evidence of validity shown in this study, reinforces the assumption of an AD aggression subscale among these 4 items.
The current finding of AD aggression’s proportional relationship with caregiver burden agrees with prior studies denoting the significant contributions of AD aggression to caregiver stress.3,6,12,22 Hart et al found that aggression caused more distress to caregivers than any other behavioral disturbance related to dementia. 12 The current finding regarding the relationship between AD aggression and 2 strategies of coping, emotion- and avoidance-focused, falls in line with the previous research that shows these strategies typically aligned with the issues of caregiver adversity.36,37,51 Also, this study’s finding of AD aggression’s negative link to caregiver resilience reflects the findings of the previous research. 52
Implications
Caregivers in a study by Miyamoto et al reported that care recipients' aggressive behavior caused caregivers to fear for their safety as well as sadness from witnessing behavior so incongruent to the person they know and love. 6 Caregivers choosing to care for their loved one at home must adapt to the added burden of time and responsibility while watching their loved one deteriorate physically and mentally. Monitoring aggressive behavior and related caregiver stress allows health care practitioners to intervene as the behavior first appears or begins to worsen. Relative to this intervention, the current study found that the proposed AD aggression measure is a valid and reliable method of determining the emotional response of a caregiver to her or his care recipient’s aggressive behavior. Previous studies found the full RMBPC to be a helpful, practical, and easy-to-use scale in clinical settings.15,49 The use of the aggressive behavior subscale provides doctors, mental health professionals, and other clinicians a quick understanding of the prevalence of the behavior without having to observe the individual. Longitudinal use of the AD aggression measure may assist health care providers to discern increases and or decreases in aggressive behavior and make changes to treatment intervention accordingly.15,49,53 Altering the treatment plan may include adjusting or adding medication, making environmental changes, and or training the caregiver in aggressive behavior-reducing techniques.
The aggressive behavior subscale may also identify caregivers needing intervention in order to minimize or reduce burden outcomes such as psychological and physiological distress. This study found that caregivers reporting a higher frequency of aggressive behavior were more likely to utilize emotion- and avoidance-focused coping strategies. As previous research links these strategies with negative psychological outcomes, these caregivers are at a higher risk of depression, anxiety, and physiological symptoms related to stress.36,37,51 Mental health professionals can intervene by helping the caregiver identify unhelpful and maladaptive coping techniques. Once these techniques are identified and acknowledged, the social worker can teach the caregiver more successful, task-focused coping strategies and improve his or her problem-solving skills. Caregivers may find that they need these lessons to be reinforced as the disease progresses and new symptoms or complications arise. The subscale can be helpful to caregivers to monitor their reactions to the care recipients' behavior and examine whether environmental changes or strategies are working to minimize aggressive behavior.
Upon identification of a caregiver’s upsurge in ratings on the AD aggression measure, health care providers can also emphasize the importance of social support. Many caregivers increasingly sacrifice their time with friends and family throughout the duration of care, especially when aggressive behavior is present. 25 Decreased social support coincides with caregivers' poorer physiological health, greater strain due to caregiving, depression, and anxiety.3,54,55 Informal social support (eg, time with family members and friends) often augments caregiver resilience.35,56,57 More formal types of support, such as respite care and support groups, may provide much-needed rest from caregiving duties, opportunities to receive validation, and expressions of concern from peers, and community resources to reduce the financial burden of caregiving.58,59
Limitations
The higher percentage of gender (80% female) and older average age (61 years) compared to the general AD caregiver population may have been due to participant recruitment methods. A large portion of participants in this study were recruited from AD support groups, members of which are more likely to be older and female.48,59 Previous research showed gender and age as important factors correlated to caregiver burden.3,25,49,60 Future research could include populations who are less likely to seek out support services in their caregiving responsibilities.
The data instrument was a self-administered survey. The behavior items are stated in general terms and depend on the interpretation of the individual taking the survey. For example, some caregivers may interpret threatening harm to others differently than others, depending on the caregiver’s perception of bodily expression. Therefore, the items are vulnerable to the subjective opinions and observations of the individual caregiver. Item responses are also dependent on the caregiver’s ability to recall instances of problem behavior. Because the survey is self-reporting, it does not have the accuracy that observation or interviewing may provide. 15 Also, the instrument was written on a 10th grade reading level which may have presented an instrumentation threat to the internal validity of results. 15 This threat was less prominent in the second phase of data collection as the consultant was present with participants during data collection.
Conclusion
This study examined the psychometric properties of a proposed aggressive behavior subscale of the RMBPC and findings showed it is valid and reliable. This measure can alert health care practitioners to the presence or escalation of AD aggression via its emotional response from caregivers. Such knowledge enables professionals to better prepare informal caregivers by informing them of effective coping strategies, including the reduction of environmental triggers for AD aggression. It is hoped that this scale will be a helpful and practical resource for AD researchers, professionals, and caregivers, as they face the challenge of providing dignity and better quality of life for individuals with AD.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The John A. Hartford Foundation's Faculty Scholars in Geriatric Social Work Program, administered by the Gerontological Society of America.