
Abstract
The aim of this study was to investigate the practical utility of endocervicoscopy and targeted biopsy in high-risk human papilloma virus–positive women with abnormal squamous cells on cervical cytology and unsatisfactory colposcopy with nonvisible squamocolumnar junction. Seventy-seven high-risk human papilloma virus–positive patients with abnormal cervical cytology for squamous cells bearing type 3 transformation zone were enrolled. Endoscopic examination of the endocervical epithelium, with office-based continuous-flow hysteroscopy after application of acetic acid 5%, followed by targeted biopsies and consequent large loop excision of the transformation zone was carried out. Sensitivity, specificity, positive predictive value and negative predictive value of endocervicoscopy, and orientated biopsy were confronted with the results of large loop excision of the transformation zone (referral test). The sensitivity and specificity of endocervicoscopy and orientated biopsy for low-grade cervical intraepithelial neoplasia were 53% and 81%, respectively, while the sensitivity and specificity for high-grade cervical intraepithelial neoplasia were 64% and 47%, respectively. The positive predictive value for low-grade cervical intraepithelial neoplasia was 64% and for high-grade cervical intraepithelial neoplasia was 88%. The negative predictive value for low-grade cervical intraepithelial neoplasia was 87% and for high-grade cervical intraepithelial neoplasia was 41%. Endocervicoscopy is a safe, office-based technique. It is a reliable method to detect the transformation zone in patients with type 3 transformation zone and unsatisfactory colposcopy. It potentially allows target biopsy of the transformation zone but presents a relatively low specificity/negative predictive value to predict high-grade cervical intraepithelial neoplasia, thus negative biopsy results should be interpreted with caution.
Introduction
Colposcopy is a relatively precise technique and, in expert hands, is a formidable tool in evaluating cervical preneoplastic disease. Colposcopy was first introduced in early 1925 by Hans Hinselmann, and Walter Schiller proposed a precursor of Pap smear in 1928. Despite the continuous changes in techniques and devices, the main aim of colposcopy remains the detection of precancerous lesions. 1,2
Colposcopy associated with cervical cytology and the human papilloma virus (HPV) test are the most effective examinations to detect cervical intraepithelial neoplasia (CIN), and together they have contributed to the dramatic decrease in the incidence of cervical squamous carcinoma. 3 –10 However, the false positive and false negative results of cytology are well known. 11 –18
Not all women present a visible squamocolumnar junction (SCJ) suitable for colposcopic evaluation of the transformation zone (TZ). The discrepancy between a positive high-risk HPV test and a borderline cytology in women with nonvisible TZ constitutes a therapeutic dilemma and may lead to unnecessary conization which, especially in the childbearing age, is an overtreatment with a considerable burden for patients and community.
Endocervicoscopy is a relatively new procedure proposed for the evaluation of endocervical epithelium. This technique combines the classic hysteroscopic equipment with the colposcopic classification system. 19,20 The aim of this study was to investigate the accuracy of endocervicoscopy with orientated biopsy to detect CIN in high-risk HPV–positive women with abnormal squamous cells on cervical cytology, nonvisible SCJ, and unsatisfactory colposcopy (type 3 TZ).
Patients and Methods
Among 435 patients who underwent colposcopy, 77 women, bearing a type 3 TZ, were enrolled. All patients underwent endocervicoscopy with orientated punch biopsy and consequent large loop excision of the transformation zone (LLETZ) according to the guideline of the European Federation for Colposcopy in the management of abnormal cervical cytology. 21 In all cases, SCJ was visualized and, regardless of the endocervicoscopic findings, all biopsies were performed on TZ.
Inclusion criteria were a positive high-risk HPV test, adequate cervical cytology consistent with squamous dyskaryosis (low and high grade) or abnormal squamous cells, a type 3 TZ, and an intact LLETZ, including the TZ, with no CIN on endocervical, ectocervical, and deep/lateral margins. Exclusion criteria were a negative high-risk HPV test, inadequate cervical cytology, type 1 and 2 TZ, abnormal cytology consistent or suspicious for glandular lesion, and patients who underwent conization. The LLETZs with positive margins and/or with no TZ included, fragmented LLETZs and LLETZs which showed important diathermy artifacts, not suitable for a precise evaluation of margins, were also excluded from the study.
Normal endocervicoscopy consisted of the absence of acetoreactive areas and abnormal vessels. Abnormal endocervicoscopic findings consisted of acetowhite areas, abnormal vessels, cuffed crypt (gland) openings, and erosion. Irregular border, inner border sign, ridge sign, and rapid appearance of acetowhitening, which are part of colposcopic findings, were not assessable in endocervicoscopy procedure.
Cervical cytology was carried out by fluid-based, thin-layer ThinPrep (Cytyc, Boxborough, Massachusetts) as previously reported. 22 Endocervicoscopy with biopsy was performed according to the procedure described by Bifulco et al. 19
The study was conducted according to the World Medical Association Declaration of Helsinki. The aim of this study was to ameliorate the diagnostic service; therefore, no institutional review board and/or ethics committee approval from San Carlo Hospital, Rome, Italy, was necessary. Patients provided oral informed consent, which was inserted into the medical charts.
Statistical Analysis
Statistical analysis was performed with SPSS software package V.22 (SPSS, Inc, Chicago, Illinois). Demographic and clinical characteristics were summarized by standard descriptive summaries.
Pearson chi-square test was used to assess the association (contingency) between the results provided by the diagnostic tests here considered. Finally, to describe the performance of punch biopsy during endocervicoscopy with respect to LLETZ, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated.
Results
The study was performed between 2011 and 2015. Seventy-seven patients met the inclusion criteria and were eligible for study. The mean age of patients was 41.1 ± 9.6 years (median 42 years, range 20-67 years). Cytology showed low-grade dyskaryosis in 28 (36.4%), high-grade dyskaryosis in 28 (36.4%), borderline squamous cells in 8 (10.4%), and borderline/suspicious high-grade squamous cells in 13 (16.9%) patients.
Endocervicoscopic findings were normal in 11 (14.3%) and abnormal in 66 (85.7%) patients. Endocervical biopsy showed negative results in 13 (16.9%), low-grade CIN in 14 (18.2%), and high-grade CIN in 50 (64.9%) patients (Table 1).
Clinical and Cyto-Histopathological Characteristics of Patients.a

Abbreviations: BSC, borderline squamous cells (atypical squamous cells of uncertain significance [ASCUS]); BSC/HG, borderline squamous cells/high-grade (atypical squamous cells of uncertain significance/high-grade [ASC-HG]); EC, endocervicoscopy; ECB, endocervical biopsy; HGCIN, high-grade cervical intraepithelial neoplasia; HGSDYS, high-grade squamous dyskaryosis (high-grade intraepithelial lesion [HGSIL]); LGCIN, low-grade cervical intraepithelial neoplasia; LGSDYS, low-grade squamous dyskaryosis (low-grade intraepithelial lesion [LGSIL]); LLETZ, loop excision of the transformation zone; SCC, squamous cell carcinoma.
aResults are expressed as means (standard deviations) or as frequency (percentage).
Considering cytology findings and endocervicoscopy (P = 0.79) of 28 patients with low-grade dyskaryosis on cytology, 4 patients showed normal, while 24 patients showed abnormal endocervicoscopy results. Of the 28 patients with high-grade dyskaryosis on cytology, 3 patients had normal, while 25 had abnormal endocervicoscopy results. Endocervicoscopy was normal in 1 of 8 women with borderline squamous cells, while 7 women showed abnormal findings. Among 13 patients with borderline/suspicious high-grade cytology, 3 had normal endocervicoscopy results, while in 10 the findings were abnormal. Considering endocervicoscopy and endocervical biopsy results, among 13 patients with a normal biopsy results, 4 had normal and 9 had an abnormal endocervicoscopy result. Three of 14 women showing low-grade CIN (Figure 1) had normal endocervicoscopy, while 11 showed abnormal results.

Endocervicoscopic biopsy of low-grade CIN.
Among 50 patients presenting high-grade CIN on biopsy (Figure 2), 4 had normal endocervicoscopy and 46 showed abnormal results. Although the number of patients is too low, there was a statistically significant association between LLETZ and endocervicoscopy results (P = .016).
Endocervicoscopic biopsy of high-grade CIN.
The comparison between endocervicoscopy and LLETZ results showed that among 17 patients presenting low-grade CIN, 5 had normal and 12 presented abnormal endocervicoscopy results. Among 59 patients with high-grade CIN, 5 had a normal and 54 showed abnormal findings. One patient with microinvasive squamous cell carcinoma (SCC) showed normal endocervicoscopy (Table 2).
Endocervicoscopy Results by PAP, Biopsy (ECB), and LLETZ.a

Abbreviations: BSC, borderline squamous cells; BSC/HG, borderline squamous cells/high grade; ECB, endocervical biopsy; HGCIN, high-grade cervical intraepithelial neoplasia; HGSDYS, high-grade squamous dyskaryosis; LGCIN, low-grade cervical intraepithelial neoplasia; LGSDYS, low-grade squamous dyskaryosis; LLETZ, large loop excision of the transformation zone; PAP, Papanicolaou test; SCC, squamous cell carcinoma.
aResults are expressed as frequency (percentage).
b P value refers to chi-square test.
When the results of endocervical biopsy were compared with the results of LLETZ, a statistically significant association (P = .003) was found: 2 of 13 patients with normal biopsy showed low-grade CIN on LLETZ, while 11 patients showed high-grade CIN. Of the 14 patients with low-grade CIN on biopsy, 9 showed the same results on LLETZ, while 5 patients showed high-grade CIN.
Among 50 patients showing high-grade CIN on biopsy, the diagnosis was confirmed on LLETZ in 43 patients; 6 women showed low-grade CIN and 1 patient showed SCC (Table 3). Table 4 reports the sensitivity, specificity, PPV, and NPV of endocervicoscopic biopsy with respect to LLETZ. The sensitivity and specificity for low-grade CIN were 53% and 81%, respectively. The sensitivity and specificity for high-grade CIN were 64% and 47%, respectively. The PPV for low-grade CIN was 64% and 88% for high-grade CIN. The NPV for low-grade CIN was 87% and 41% for high-grade CIN.
Biopsy Results by LLETZ Expressed as Frequency (Percentage).
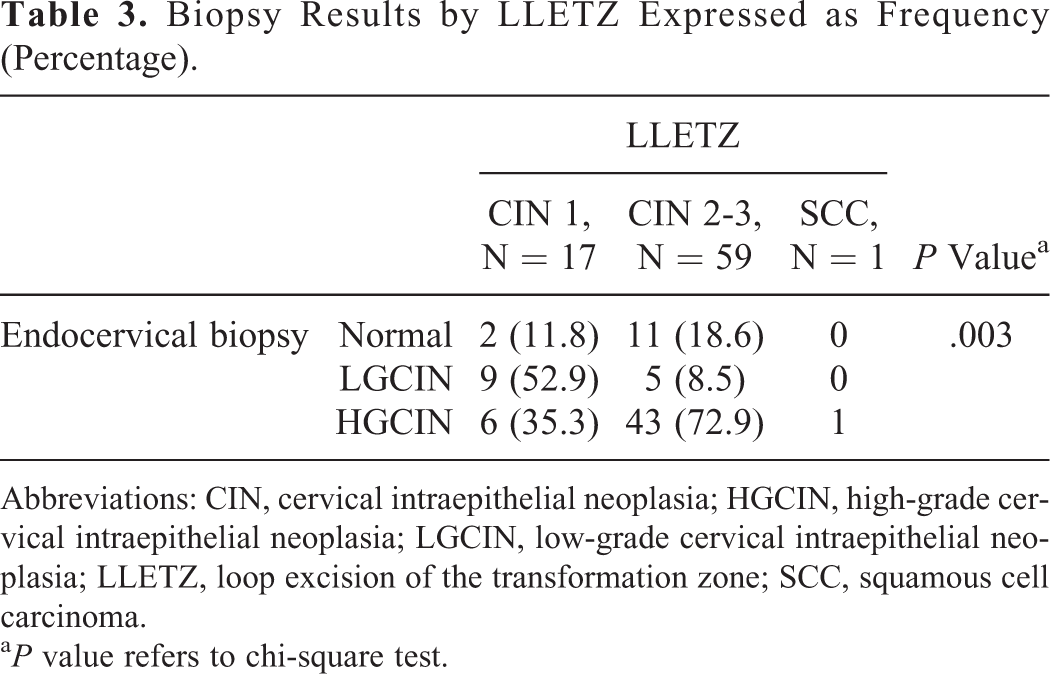
Abbreviations: CIN, cervical intraepithelial neoplasia; HGCIN, high-grade cervical intraepithelial neoplasia; LGCIN, low-grade cervical intraepithelial neoplasia; LLETZ, loop excision of the transformation zone; SCC, squamous cell carcinoma.
a P value refers to chi-square test.
Sensitivity, Specificity, PPV, and NPV of Endocervical Biopsy Considering LLETZ as the Gold Standard.

Abbreviations: HGCIN, high-grade cervical intraepithelial neoplasia; LGCIN, low-grade cervical intraepithelial neoplasia; LLETZ, loop excision of the transformation zone; NPV, negative predictive value; PPV, positive predictive value.
Discussion
In the present study, we show a statistically significant association between cervical cytology results and endocervicoscopic findings. Only 13 of 77 patients with abnormal squamous cells on cytology showed normal endocervicoscopy. These data suggest that endocervicoscopy is a reliable method to detect the TZ in patients with a type 3 TZ and potentially allows target biopsy.
It is worth mentioning that endocervicoscopy presents some limits similar to classic colposcopy. The presence of acetowhite endocervical areas does not necessarily mean abnormality because these could represent a normal physiological phenomenon such as immature squamous metaplasia. Conversely, the absence of acetowhite areas does not rule out cervical dysplasia.
The sensitivity (true positive rate) of endocervicoscopy with biopsy, as a diagnostic tool, is moderate/high (64%) for detecting high-grade CIN and moderate (53%) for detecting low-grade CIN. The specificity (true negative rate) is low/moderate (47%) for high-grade CIN and high (81%) for low-grade CIN. Seven patients with normal endocervicoscopy showed either low-grade CIN (3 patients; 27.2%) or high-grade CIN (4 patients; 36.3%) on direct biopsy. This means that 63.6% of patients with normal endocervicoscopic findings presented CIN on biopsy. When the results of biopsy were compared with LLETZ, relatively worrisome data emerged. According to our findings, while endocervicoscopy and biopsy showed a high NPV (87%) for low-grade CIN, the NPV for high-grade CIN was relatively low (41%).
This means that the probability that a patient without high-grade CIN on biopsy did not have this disease in LLETZ (NPV) was 41%. Endocervicoscopy and biopsy show a high PPV for high-grade CIN and a relatively high PPV for low-grade CIN. The probability that the diagnosis of CIN was confirmed on LLETZ (PPV) was 88% for high-grade CIN and 64% for low-grade CIN. However, the possibility that the entire lesion was removed by biopsy prior to LLETZ cannot be ruled out.
It is noteworthy that the data regarding SCC are unreliable because only 1 case was detected. Nevertheless, the reasons for failure to detect abnormal endocervicoscopic features of SCC, even in 1 case, need to be investigated more in depth. Since endocervicoscopy, as classic colposcopy, is an operator-dependent technology, human factors as a source of error cannot be ruled out. Nevertheless, it should be emphasized that the patient had a microinvasive SCC (FIGO stage 1A1) which can be misdiagnosed even in classic colposcopy. Furthermore, in case of previous damage to cervical mucosa (laser treatment, cold coagulation, cryotherapy), reparative re-epithelization might hide the undermining neoplastic process. The patient included in this study referred that 3 years before conization she had had outpatient treatment with no histological analysis; however, we were unable to find the details of treatment.
Management of patients with a type 3 TZ largely depends on cervical cytological/histological results. An unsatisfactory colposcopy following high-grade CIN warrants a diagnostic/therapeutic LLETZ. If colposcopic biopsy is normal and cervical cytology is less severe than high-grade CIN, then repeating cytology at 6 and 12 months, HPV testing at 1 year, or a cytology and colposcopy at 1 year are all acceptable strategies. 23
Cervical conization, in many instances, may not reveal a preneoplastic condition. Although LLETZ is widely regarded as minor surgery and can be performed on an outpatient basis, it is well known that this procedure carries significant morbidity and complications include cervical stenosis, bleeding, premature rupture of the membranes, preterm delivery, low birth weight, and an increased risk of caesarean delivery. 24,25
However, with regard to the preterm birth, relatively recent data show that women with a history of LEEZ have similar risk of preterm birth when compared with women with prior dysplasia but no cervical excision. 26 Endocervical curettage could represent an alternative to endocervicoscopy. However, curettage is an uncomfortable, relatively invasive and blind procedure, which does not allow determination of the exact topography of endocervical lesions or the possibility to carry out target biopsy. Additionally, it has been shown that endocervical curettage, with respect to endocervicoscopy, misses a non-negligible part of endocervical abnormalities. 19 Endocervicoscopy is an office-based technique with no anesthesia and/or analgesia requirements where instrumentation for traditional hysteroscopy is used. However, a few issues should be addressed. Endocervical curettage is a well-accepted and diffuse method, and the aim of our study was not to compare endocervicoscopy with biopsy and endocervical curettage because there are extremely limited data on endocervicoscopy in the literature. Our attempt was to design a study, which could focus on an innovative method.
Our data do not confirm the good performance reported in the previous study. 19 Although the number of patients in our study was relatively small, our findings showed that endocervicoscopic biopsy presents a low specificity/NPV to identify high-grade CIN and negative biopsy results should be interpreted with caution. This finding represents the weakness and limit of endocervicoscopic biopsy in daily clinical practice. Theoretically, underestimation of low-grade CIN might not constitute real harm for the patient while underdiagnosed high-grade CIN, due to its potential malignancy, cannot be underestimated. A high-grade CIN may hide an underlying microinvasive/invasive SCC. It is worth mentioning that since no patient with a clinical history of conization was included in this study, unsatisfactory colposcopy might be due to atrophy or unknown anatomy abnormality of TZ (Figure 3).

The summary of the results. This table summarize the relationship between the results of cytology, histology (biopsy and LLETZ) with endocervicoscopy findings.
Future studies with a large number of patients are warranted in order to analyze the causes of pitfalls in the diagnostic capacity of endocervicoscopy in patients with type 3 TZ and unsatisfactory colposcopy.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.