
Abstract
The aim of the study was to perform cryosurgery on a primary breast tumor, coupled with simultaneous peritumoral and intratumoral tracer injection of a blue dye, to evaluate lymphatic mapping. We explored the ability of our strategy to prevent tumor cells, but not that of injected tracers, to migrate to the lymphovascular drainage during conventional resection of frozen breast malignancies. Seventeen patients aged 51 (14) years (mean [standard deviation]), presenting primary breast cancer with stage I to IV, were randomly selected and treated in The Rudolfinerhaus Private Clinic in Vienna, Austria, and included in this preliminary clinical study. Under intraoperative ultrasound, 14 patients underwent curative cryo-assisted tumor resection en bloc, coupled with peritumoral tracer injection, which consisted of complete tumor freezing and concomitant peritumor injection with a blue dye, before resection and sentinel lymph node dissection (group A). Group B consists of 3 patients previously refused any standard therapy and had palliative tumor cryoablation in situ combined with intratumoral tracer injection. The intraoperative ultrasound facilitated needle positioning and dye injection timing. In group A, the frozen site extruded the dye that was distributed through the unfrozen tumor, the breast tissue, and the resection cavity for 12 patients. One to 4 lymph nodes were stained for 10 of 14 patients. The resection margin was evaluable. Our intraoperative ultrasound-guided performance revealed the injection and migration of a blue dye during the frozen resection en bloc and cryoablation in situ of primary breast tumors. Sentinel lymph node mapping, pathological determination of the tumor, and resection margins were achievable. The study paves the way for intraoperative cryo-assisted therapeutic strategies for breast cancer.
Keywords
Introduction
The therapy for breast cancer is multimodal. 1 –3 Surgery is considered a central method, but the rate of postsurgical recurrence is an ongoing issue. 4 –6
Cryoablation for primary and secondary breast cancer is well known. 7 –9 Surgical resection of a frozen tumor has also been previously proposed for primary and secondary breast cancer. 10 –12 Percutaneous cryoablation is an efficient treatment method for advanced or recurrent breast cancer. 13 –15 Cryosurgery is used as an adjuvant during surgical resection of solid tumors. 16 –22 Therapeutic fluids, like mixtures and suspensions of tracer and active drugs, have also been interstitially coinjected during cryoablation to increase the local efficacy of cytotoxic agents at the tumor margin on transplanted tumor models. 23,24 However, the timing of the injection of drugs relative to freeze–thaw sequences and the route of injection are still under debate. 25
At our institutions, we use various cryosurgical procedures on patients presenting with primary breast tumor, metastatic or not, or with recurrent breast cancer, 7,10,13,26,27 regardless of their age. The cryo-assisted tumor resection (CATR) en bloc was initially pointed out by Korpan, 9,10,26,27 and tumor cryoablation (TCA) in situ is similar to what has previously been described for the management of liver tumors 16 –18,28,29 or for the recanalization of airway structures. 18,19,22 The objective is to trap tumor cells in the frozen mass, which is momentarily deprived of blood and lymph flow, to prevent the intraoperative dissemination of malignant cells during tumor manipulation locally, regionally, and systemically. 26,27 The unresectable tumors are always treated using cryoprobes as an ablative and palliative tool. 9,10
For the surgical management of regional lymph nodes, axillary exploration and lymph node dissection will usually be performed with preoperative sentinel lymph node mapping using a radioactive tracer followed by sentinel lymph node dissection (SLND). 30 Due to the cost and constraints of lymphoscintigraphy, we have elected to perform the intraoperative injection of a blue dye for sentinel lymph node mapping during our cryo-assisted procedure. In this article, we report our initial experience with this procedure.
To our knowledge, this is the first study to look at the transport and locoregional distribution of a dye injected into a breast tumor, subjected to simultaneous cryo-assisted resection and cryoablation. Our primary objective was to define the conditions and to evaluate the feasibility of injecting a peritumoral dye tracer into tumors undergoing cryosurgery. The flow and transport of patent blue vital (PBV) dye and methylene blue (MB) were evaluated using intraoperative ultrasound (IOUS) imaging. We also wanted to determine whether and how the procedure affected normal surgical workflow, in particular lymph node mapping, tumor characterization, and margin status determination.
Materials and Methods
Patients
This study was conducted in The Rudolfinerhaus Private Clinic in Vienna, Austria. Seventeen patients aged 51 (14) years (mean [standard deviation, SD]), presenting with primary breast tumor at stages I to III or de novo stage IV breast cancer, 30 were randomly selected and treated in our institution (Table 1). All patients gave informed consent. In group A, 14 patients underwent curative CATR en bloc coupled with peritumoral tracer injection (PTI) under IOUS. Group B consists of 3 patients previously refused any systemic or local therapy (surgery, chemotherapy, or radiotherapy) and had palliative TCA in situ combined with intratumoral tracer injection (ITI).
Baseline Characteristics of Patients With Primary Breast Carcinoma.

Abbreviations: IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; SD standard deviation.
aTwo patients presented with aggressive tumor (G3, triple negative).
bOne local recurrence after adjuvant chemotherapy, hormonotherapy, and radiation therapy.
Twelve of the 17 patients had localized primary breast cancer, which was estimated to be resectable without neoadjuvant chemotherapy. Inflammatory breast cancer was specified in group A (n = 1) and group B (n = 3). Two patients have undergone previous systemic chemotherapy before the CATR en bloc. One patient presented with a large matted axillary nodal metastasis. The primary breast tumors were histologically verified as invasive ductal carcinoma in 15 patients and invasive lobular carcinoma in 2 cases with histological grades G2 (6/17) and G3 (11/17), according to the Nottingham histological score. Two of the 5 patients with stage III disease had aggressive tumor characteristics, that is, G3 and triple negative receptor status. 31 One patient with invasive ductal breast cancer had the medullary subtype, which is histologically G3 but with better prognosis. In group A, lymph nodes were histologically metastatic in 4 cases, with primary breast carcinoma followed by axillary lymph node dissection (ALND), level I to III (Table 2).
Lymph Node Staining and Pathological Status for the Surgical Group A.

Abbreviations: ALND, axillary lymph node dissection, level I-III; LN, lymph node; SLND, sentinel lymph node dissection.
Treatment Summary
The curative CATR en bloc, consisting of 14 patients (group A), had cryosurgery with simultaneous PTI of a blue dye. A few minutes after cryo-assisted tumor injection, the frozen breast tumor around the sharp demarcated ice margin was conventionally resected and marked with sutures for spatial orientation by the pathologist. The frozen tumor samples were then subjected to tumor characterization and margin evaluation. Axillary exploration and lymph node clearance were done by SLND on all 14 patients; frozen sections of the resected nodes were examined and a completion ALND was performed on 4 patients (group A). The palliative TCA in situ and simultaneous ITI, on 3 patients, were carried out without subsequent surgery (group B). These intraoperative therapies are summarized in Table 3. We assumed that the frozen zone of the tumor during cryoresection or cryoablation will behave as an exclusion zone for the injected tracer; the latter would move within the unfrozen peritumoral interstitial spaces and would be available for a migration into the draining lymphatics.
Cryo-Assisted Resection En Bloc and Cryoablation In Situ of Primary Breast Cancer With Concomitant Peri- and Intratumoral Tracer Injection.

Abbreviations: ALND, axillary lymph node dissection; dye, patent blue V or methylene blue; ITI, intratumoral tracer injection; PTI, peritumoral tracer injection; SLND, sentinel lymph node dissection; VPFC, volume percentage of freezing coverage.
aResection-ALND—the freezing of a massive matted lymph node that was simultaneously injected with dye before ALND.
Cryoprobe and Injection Needle
We used a cryogenic console and reusable metal cryoprobe, with liquid nitrogen as the refrigerant (CryoPulse, Kyiv, Ukraine). The cryoprobe tip, which comes in different freezing tip diameters (20, 25, and 50 mm), was selected to best fit the tumor surface on which it is centered, while insuring good contact with moderate pressure. A single cryoprobe was used per procedure. The lowest tip temperature of −180°C was reached after about 2 minutes of continuous cooling.
We used an injection system with a 19-G Chiba spinal needle (1.1 mm) or a 25-G needle (0.5 mm) connected directly or to a 3-mL or 5-mL plastic syringe through an extension line. The needle and the fluid line were debubbled and primed before insertion into the tumor.
Ultrasound Imaging
Two ultrasound (US) systems, a Sonosite M-Turbo (Sonosite, Heliomed, Austria) and a Voluson 730 Expert (GE Healthcare Austria GmbH) with linear array transducers, were used for 2-dimensonal or 3-dimensonal real-time intraoperative needle injection. The ice block, along with an unfrozen breast tissue layer with a thickness of 34 mm (7 mm), determined the palpable limits of the resection plane. 32 Intraoperative ultrasound helped to evaluate the location of the frozen margin in the breast. 33
Dye, Dosing, and Site of Injection
We used 2.5% PBV, a small molecule (Molecular Weight 582.7 g/mol) that has tracing ability for lymphatic mapping of breast cancer, 34 for most of our study, and 1% MB in 3 cases. 35 All tumors received the same dose regardless of size. Since the frozen tumor was expected to behave as an impervious zone to a fluid coinjected in its vicinity, we hypothesized that a fixed amount of tracer (2 mL) should flow about and away from any tumor mass properly frozen.
Tumor Freezing and Dye Injection
The treatment planning consisted in preliminary evaluation of the number and location of freeze (FRZ) sites necessary to cover the tumor target with overlapping FRZ margins. For the patients in group A (n = 14), the IOUS-guided procedure consisted of a freeze–thaw–refreeze of the tumor to create an ice block that was resected according to our published protocol. 10 Blue dye was directly injected into an unfrozen zone of the tumor before the zone was engulfed in ice. For the patients in group B (n = 3), the tracer injecion was spritzed into the tumor tissue that remained unfrozen, and a similar freezing injection procedure was conducted without any associated conventional surgery. Tumors larger than 5 cm were treated at 2 to 4 contiguous locations. The FRZ sites were decentered so that the ice margins overlap happened in the tumor center, which could experience up to 4 freeze–thaw cycles. A single cryoprobe was used for each patient, and the cryoprobe was repositioned whenever necessary. Biopsies were taken in multiple sites including the tumor periphery.
The procedural steps for the patients in group A (Figure 1) are as follows: a conventional surgical approach to the tumor surface; a careful, gentle dissection of the tumor surface to minimize the disruption of the deep lymphovascular draining pathways; the selection of the appropriate cryoprobe that would best fit the tumor size and enable the central placement of its tip over the tumor surface; the positioning of the US transducer for the visualization of the tumor contours; the US-guided insertion of the needle tip at the tumor margin most distal from the probe, and in a direction that sets the needle shaft or tip at least 20 mm away from the probe tip; the verification of the needle lumen patency by injecting a few microliters of the selected tracer; and the initiation of the first tumor FRZ for three minutes (Figure 2A).

Procedural diagram of the cryosurgical approach coupled with peritumoral tracer injection. Double deep freeze (DDF) starts with first freeze (FRZ) concomitantly with peritumoral dye injection (PDI, dark blue arrow) and ice block formation (IBF, light blue color) before resection. This freeze-inject-thaw-refreeze procedure takes about 16 minutes from beginning to completion. The blue dye injected at the tumor margin (peritumoral) at the end of the first FRZ migrates diffusely into the TT and distributes widely into the BIP. After second FRZ (RE-FRZ), the ice block (IB) containing the TT is completely resected on an unfrozen breast margin with the following SLND. AF indicates axillary fat (yellow color); BIP, breast interstitium and parenchyma (yellow patterns); DSLN, dye sentinel lymph nodes; TP, tumor preparation; TR, tumor resection en bloc; TT, tumor tissue (gray patterns).
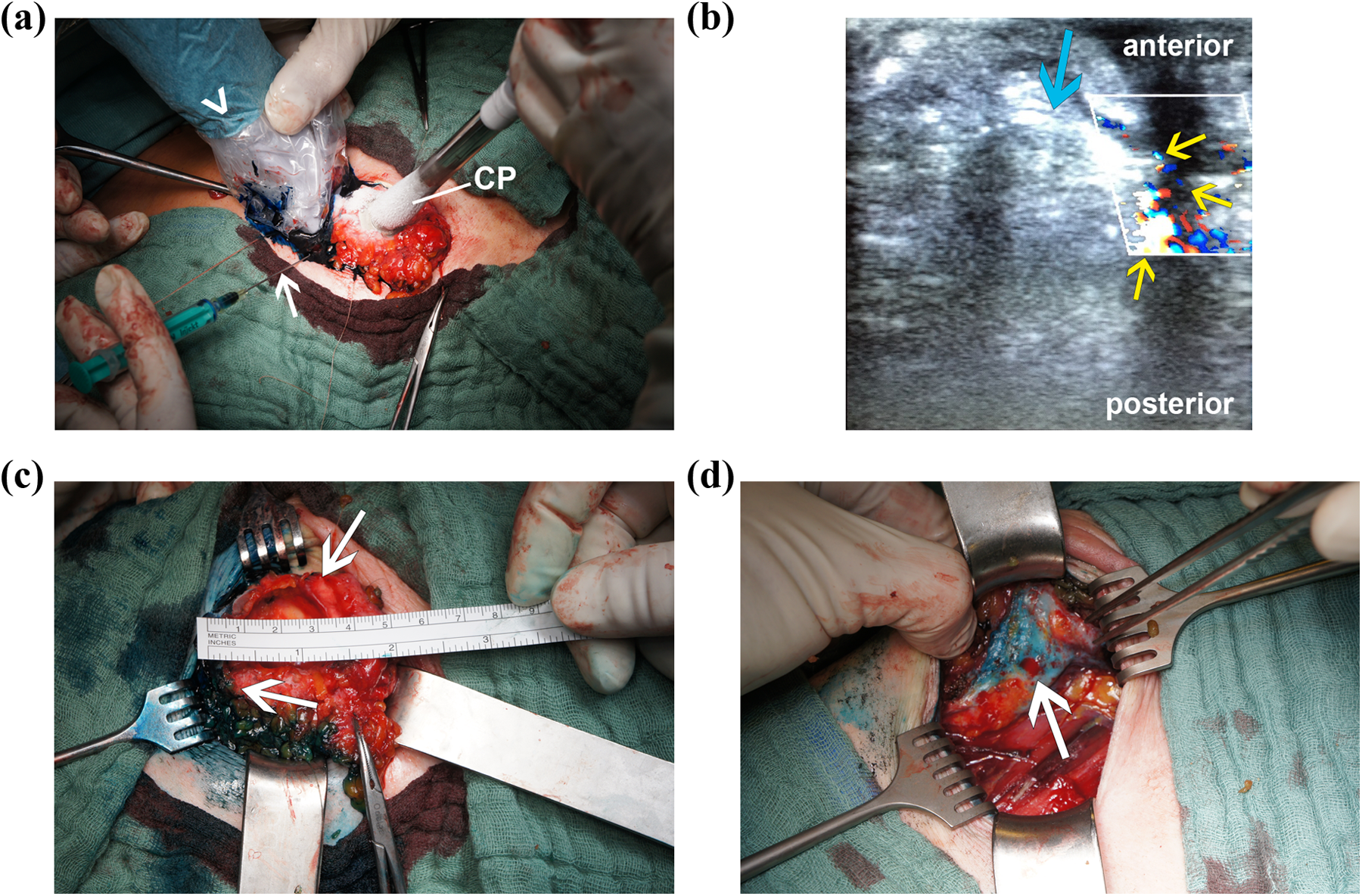
A-D, Cryo-assisted tumor resection en bloc and peritumoral tracer injection in patients with primary breast carcinoma. Intraoperative sequence showing cryo-assisted tumor resection en bloc, concomitant with peritumoral tracer injection of a breast tumor, located in the upper right outer quadrant (group A). A, The cryoprobe (CP) tip, 25 mm in diameter, freezes and sticks to the surface of a 19-mm-wide tumor and a margin of breast parenchyma. The injection needle (white arrow), inserted into a deeper, not yet frozen part of the tumor, at the tumor margin, is shown injecting 2 mL of patent blue vital dye under US imaging (white arrowhead). B, The longitudinal view sonogram shows the hyperechoic ice margin (blue arrow) at the anterior aspect of the tumor. The flow (3 yellow arrows) of the dye is detected at the posterior aspect of the tumor about to be frozen. A fluid dye channel, anechoic, is located between the ice margin and the breast tissue; C, The CP and the needle have been removed after the second freeze, but the tumor surface is still frozen and the blue staining is visible at the frozen tumor margin (arrows) just before the tumor resection en bloc. D, Sentinel lymph node dissection (SLND) reveals a stained node (arrow) in the axillary region. Some staining of the resection cavity is seen.
Our device records the thermal history at the cryoprobe tip. It took 2 minutes to drop the tip temperature to −180°C. Our rule was to visualize or image the frozen margin located 8 to 12 mm outside of the tumor contours. Tissue temperatures were not taken. During cryoresection or cryoablation, we had efficient control over the ice front barrier effect with IOUS. The continuous delivery of the injected dye, introduced in the third minute of the cooling process, was imaged with color flow Doppler. After completion of the injection and the first FRZ, the cryoprobe was set to thaw. This heating was active for 45 seconds and passive for 8 minutes, allowing us to image the ice front extending to the posterior aspect of the tumor and to evaluate the migration of the dye around the tumor (Figure 2B). A second 3-minute FRZ was set without any dye reinjection and was immediately followed by the resection of the ice block (Figure 2C). The resection line was located in the unfrozen breast tissue at 34 mm (7 mm) from the ice block margin. Lymph node surgery was conducted according to the intraoperative sentinel lymph node mapping (Figure 2D) and/or the preoperative plan.
Gross Examination and Microscopic Analysis
The resected samples were tagged with sutures for orientation and then photographed. These tumor sections made in the operating theater allowed the evaluation of stain distribution through gross examination. The frozen sections also allowed for immediate pathological characterization of the tumor and for determination of the resection margin status as well as resected node status.
Statistical Analysis
The study groups were compared using t tests and results are presented as the mean (SD). A probability value of <.05 was considered to be significant.
Results
Blue Dye Injection Was Feasible and Imageable With IOUS During the Ice Block Formation Process
Delivery of the dye into the unfrozen part of the tumor was uninterrupted by the concomitant first freezing, regardless of needle size. Both freezing and dye delivery procedures were performed at their intended dose and duration for all cases. For both groups A and B, IOUS monitoring facilitated needle placement and demonstrated the presence and progression of the ice margin within the tumor and surrounding parenchyma in the anteroposterior direction. For the patients in group A, upon completion of the refreeze sequence, the tumor and 8 to 12 mm of breast tissue margin were frozen as intended before probe detachment and initiation of resection. However, proper needle tip positioning at the deep part of the tumor under IOUS took an additional 5 to 10 minutes for the first few patients and took under 5 minutes for the last. The 3-minute refreeze period after the first freeze-injection-and-thaw sequence increased the size of the ice block by a few millimeters without affecting the dye distribution observed after the first FRZ. 36 The presence of blood flow was not detected by IOUS flow imaging before cryosurgery. 33
The Dye Was Transported to the Ice Block Margin, Within the Tumor, and the Lymphatic Drainage
Our cryoprocedure that contacted and froze the tumor (Figure 2A) from its surface to its depth resulted in a lateral and anterior–posterior progression of the ice block, whose hyperechoic margin was readily visualized by US imaging. The flow of the dye was mapped by color Doppler at the ice margin during injection for both groups of patients (Figure 2B). Following dye injection, 10 of 14 patients (group A) had 1 to 4 nodes stained SLND. Of 4 patients who underwent ALND, 3 showed no staining and 1 showed a large matted nodal mass that was directly injected and not counted in the mapping. Lymph nodes were metastatic in 4 cases with primary breast carcinoma.
The patients in group B received palliative tumor freezing with intratumor injection of blue dye without surgery, so nodal staining was not evaluated for this group. The US color Doppler flow images for these patients revealed a dye flow pattern along the ice margin that was similar to what was observed for the patients in group A (Table 3). Breast tissue containing the hard tumoral ice block was easily dissected using our procedure and was subsequently resected during the melting step that followed cryoprobe removal. The intraoperative examination of the frozen sections allowed the detection of a single R1 margin in 1 of 14 patients (group A). The positive margin was immediately re-resected. The resection cavity was stained at times. Our freeze–thaw–refreeze procedure did not affect the postoperative histological or hormonal receptor status evaluation on formalin-fixed paraffin-embedded tissue sections (Figure 3A–C).

A-C, Gross examination of the resected samples. A, After thawing, the sample is sectioned along the anteroposterior axis corresponding to the freeze margin progression. Gross examination shows variable tumor staining, with more intense staining of the deep part of the tumor (arrow) and breast tissue staining in the direction of the breast tail (arrowhead). B, Another sample shows light staining of the anterior tumor side (arrow), where the cryoprobe was located, and an intense staining in the posterior deep part of the tumor (arrowhead) where the needle was located. In this region, the breast parenchyma is also stained. C, Typical microscopic alterations observed within the frozen core of a resected tumor. The tumor tissue is distinguishable and shows early signs of cryoapoptosis and cryonecrosis (C1) with enlarged cells (1), swollen eosinophilic cytoplasm, and shrunken nuclei (2). Isolated giant tumor cells are also visible (3). H&E staining, magnification: (C3) 200×.
The Procedure Was Well Tolerated and Uneventful for All Patients
There was no unintended freezing of breast structures. We did not observe any allergic or anaphylactic reactions during the injection procedure or in the postoperative period. Wound healing was uneventful.
Discussion
Cryoprobe-assisted resection of small breast tumors has been found to be useful for the localization and containment of tumor cells during surgical manipulation of the frozen mass. 10,26,28 The injection of fluids, 14 which leads to a safer or more effective tumor kill during cryoablation, 25 is widely used during these image-guided interventions. A tracer can be injected into the cryoablated breast cancer area up to 2 weeks after cryoablation, making lymphatic mapping possible during the resection of the necrotic tumor. 37 Our preliminary clinical study aimed to investigate these points during the performance of a conventional surgical procedure.
Our technique consisted of dye injection deep into the tumor margin during the freezing process, under IOUS guidance. The resulting solid ice block was immediately resected and the lymph nodes cleared. Our short study demonstrates that tracer delivery and intraoperative lymphatic mapping, which are essential components of an effective SLND, were feasible. However, the primary goal of the cryosurgical procedure, that is, the freezing sequence concomitant with PTI, was to initiate tumor freezing and perform dye injection into an unfrozen region of the tumor before it was entirely engulfed by ice. The precise needle positioning at the deep part of the tumor and the subsequent injection of the dye before needle cooling could be adjusted for each case through IOUS. 38 This start freeze-and-inject drug delivery strategy, which prevents the tracer from penetrating the frozen tumor, distributes a smaller volume of dye intratumor compared to a start inject-and-freeze delivery sequence, which would distribute a grander dye volume into the unfrozen tumor before freezing. Previous study 36 has demonstrated that such cryo-assisted drug delivery strategy has no effect on the intra- or extratumoral dye distribution.
We could have performed the injection immediately postfreeze, but the dye would have only localized peritumorally around the frozen breast tissue. We purposely did not select this option since our strategy seeks to use the intratumor lymphatics for improved targeting of the actual lymphatic drainage of the tumor. 39,40 The staining of 1 to 4 lymph nodes in the axillary region for 10 of 14 patients in group A demonstrates the effectiveness of our technique regarding detection. We performed axillary dissection after the resection of the breast tumor ice block, that is, about 18 (2) minutes (range: 16-20 minutes). The time left for dye migration, about 20 to 25 minutes, was sufficient for the migration of the dye and is comparable to previously published data. 41,42
Previous studies have demonstrated that a dye can be injected intratumorally for breast cancer localization and sentinel lymph node mapping. 42,43 We chose a single intratumoral, rather than multiple peritumoral, injection based on the premise that the presence of intratumoral lymphatics and their role in lymphangiogenesis would better reflect the tumor lymphatic drainage. 37,39 Our results seem to confirm this hypothesis since the dye leakage was minimal with our procedure. The 2-mL tracer dose was fixed regardless of tumor volume; the dose was estimated to be available and sufficient for lymphatic mapping, due to the dye extruding effect of the frozen zone. Additionally, the small fluid volume and the injection rate would not adversely affect the ice growth or shape. 44
Our results show that both PBV and MB were able to stain at least 1 node in 4 of 14 patients (group A). This success rate is in the range of other studies that inject a similar dose of MB, fractionated at 4 points of the subareolar area 10 minutes before surgery. This shows that our double freeze procedure did not affect histological parameters significantly. Our freezing source, located at the tumor surface margin, generated asymmetrical isotherms resulting in various degrees of cell and tissue structural alterations, which are comparable to results from the use of a central intratumoral freezing source by Sahoo et al. 45 Although it is noteworthy that tumor markers cannot be reliably assessed after cryoablation, our innovative procedure in patients of group A with primary breast carcinoma allowed for pathological and hormonal receptor status evaluation.
Although our study contributes to laying the groundwork for intraoperative chemotherapy during cryosurgery, we are aware of its limitations. First, our study evaluated a limited number of patients and did not include a comparison group undergoing intratumoral injection of a tracer without cryosurgery. Although lymphatic mapping is possible with direct intratumor injection of a tracer, we could not evaluate the influence of the extruding effect of the ice volume on the transport of the dye to the lymphatic drainage, in part due to the large variation of the tumor volume in which the dye could disperse. Second, the tumor cell containment and the prevention of cell shedding theoretically permitted by our freezing technique could not be evaluated. We did not attempt to assess the location of lethal isotherm; indeed, we knew that the target tumors selected for resection would not be thoroughly killed since we were not allowing them (by design) to experience the vascular effect of cryosurgery; our cryosurgical technique calls for an asymmetrical distribution of the isotherms, therefore making any prediction of lethality quite complex; last, we considered that creating an ice block engulfing the tumor was necessary and sufficient to trap the tumor cells, create the fluid barrier, and inhibit cell division at the tumor margin (apoptosis). In short, we were trying to keep the cryo-assisted resection method simple to execute and safe. On a technical note, we were able to extract the frozen tumor during the thaw period following the refreeze sequence using palpation to assess the location of the frozen edge.
We recognize that we have been conservative with our use of the procedure. Our ability to conduct a conventional surgical procedure, lymphatic mapping, and pathological examination during and after our cryo-assisted technique paves the way for therapeutic strategies that aim to prevent or treat the dissemination of malignant cells. Lymphatic chemotherapy has already been shown to be safe and effective in improving disease-free survival and overall survival in patients with stage II to III breast cancer. 46,47 Our strategy could address locoregional minimal residual disease and infraclinic disease in a certain population of patients with breast cancer.
Conclusions
We have shown that our cryosurgical technique of repeatedly freezing deep tumors for en bloc resection or for in situ ablation of primary breast cancer, facilitated by IOUS monitoring, can be coupled with the simultaneous injection of dye tracers during conventional surgery, which then allows for lymphatic mapping. The frozen-and-thawed mass behaved as an exclusion-and-trapping zone for the tracers. The procedure did not affect margin status determination and had a minimal effect on tumor characteristics.
Footnotes
Abbreviations
Clinical Trial
Written informed consent was obtained from each participant in accordance with the World Medical Association Declaration of Helsinki. All 17 patients with primary breast cancer signed a declaration of consent for clinical study after detailed clarification with a surgeon (physician) about the purpose, manner, and course of events of the planned surgical treatment. This is documented in the clinical history of each patient in this preliminary clinical study.
Acknowledgments
The authors would like to thank all colleagues at the International Institute of Cryosurgery and medical personnel in the operating theater at the Rudolfinerhaus Hospital in Vienna, Austria, for their support and management of the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with reference to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.