
Abstract
Objective:
To investigate the efficacy of cytokine-induced killer cell-based immunotherapies in patients with advanced malignant solid tumors and the difference in clinical efficiency among 3 kinds of cytokine-induced killer cell-based immunotherapies.
Methods:
One hundred forty-six cases with advanced solid tumor, 230 cycles of cytokine-induced killer cell-based immunotherapies, were involved in this study. T-lymphocyte subsets, carcinoembryonic antigen, and adverse reactions were recorded.
Results:
CD3+ T lymphocyte, Th, NKT, and Th/Tc were increased after cytokine-induced killer cell-based treatment, from 55.67 ± 3.64 to 84.12 ± 5.15, 26.56 ± 4.47 to 42.76 ± 3.68, 1.82 ± 0.58 to 7.08 ± 0.92, 0.79 ± 3.64 to 1.35 ± 0.20, respectively (P < .001). Carcinoembryonic antigen was decreased from 398.39 ± 219.16 to 127.26 ± 153.41 (P < .001). Difference values were greater than 0 (P < .001). Difference value of carcinoembryonic antigen was obviously less than 0 (P < .001). There was no obvious difference in all variations between cytokine-induced killer cell and DC+CIK groups (P > .05). The highest amount of CD3+ T lymphocyte and Th was recorded after at least 4 cycles of immunotherapy. And CD8+ T/CD4+ T also began to decrease after 4 cycles of immunotherapy. Difference value of T lymphocyte and Tc of patients with surgery is higher than that of patients without surgery.
Conclusion:
Cytokine-induced killer cell-based immunotherapy is capable of increasing T-lymphocyte subsets, recovering cellular immunity without severe side effects, and is suitable for different kinds of solid cancer. Clinical efficiency of cytokine-induced killer cell-based immunotherapy is influenced by many factors such as surgery, stage.
Keywords
Introduction
According to the International Agency for Research on Cancer, about 14.1 million patients were diagnosed with cancer and 8.2 million people die worldwide every year. In China, about 3 million were diagnosed with cancer and 2.2 million die every year. 1 Surgical resection, chemotherapy, and radiotherapy are the 3 conventional ways of treating cancer. Unfortunately, these methods can be limited by many factors, such as multifocality, poor postoperative recovery, adverse effect, multidrug resistance, and so on. 2 In recent years, an increasing number of clinical studies have shown that cytokine-induced killer (CIK) cells–based immunotherapy can lead to promising antitumor effects in various cancers. 3 –9
Dendritic cells (DCs) are the most powerful antigen-presenting cells (APCs) that enhance the antitumor effect of CIK cells in antigen-specific cytotoxic T-lymphocyte response. 10 –12 Relevant specific antigen is presented to T cells through the major histocompatibility complex (MHC) molecules mainly by the DCs. Cytotoxic T lymphocytes recognize the MHC–tumor antigen complex and therefore kill the antigen-expressing tumor cells. 13 Cytokine-induced killer cells are lymphocytes induced and cultured with multiple cytokines to obtain antitumor activity. 14 The CD3 and CD56 double-positive T lymphocytes (NK-like T lymphocytes) have been testified to be the main effectors of CIK. 15 Studies have shown that CIK cells can specifically recognize and destroy tumor with minimal adverse reaction, mainly due to its independence of T-cell antigen receptor and MHC molecules. 2,14,16 –19 Recent studies showed that CIK-based immunotherapy prolonged overall survival and improved the quality of life of patients with hematological malignancies. 20 There were also clinical studies about cellular immunotherapy for patients with solid tumor. 21,22
However, the clinical efficiency of CIK cells–based immunotherapy in the management of solid tumors is not as observable as that in hematological malignancies. Hence, the purposes of this study were to investigate the efficiency of CIK cells–based immunotherapies, including CIK cells alone, DC and CIK combined therapy (DC+CIK), and DC cocultured with CIK therapy (DC-CIK), in advanced solid tumors in the aspects of recovering cellular immunity, reducing chemotherapy adverse reactions, and improving patients’ status and quality of life and hopefully provide valuable supportive information of adoptive immunotherapy for solid cancer treatment.
Materials and Methods
Selection of Patients
This retrospective study was approved by the ethics committee of Yantai Yuhuangding Hospital (Shan Dong, China). One hundred forty-six patients diagnosed with malignant tumors at Yantai Yuhuangding Hospital were recruited. A total of 230 cycles of infusion collected from December 2011 to January 2015 were studied, including 172 cycles of CIK cells, 34 cycles of DC+CIK, and 24 cycles of DC-CIK (DCs were cocultured with CIK). Eligible patients presented with advanced solid cancers (III-IV) with surgery or not, without cardiac, liver, and renal dysfunction. Expected survival time can be more than 3 months. All patients were given the first-line standard chemotherapy according to the National Comprehensive Cancer Network guidelines and relapsed. Patients’ characteristics are listed in Table 1. Informed consents were signed by all individual participants included in this study.
Patients’ characteristics.
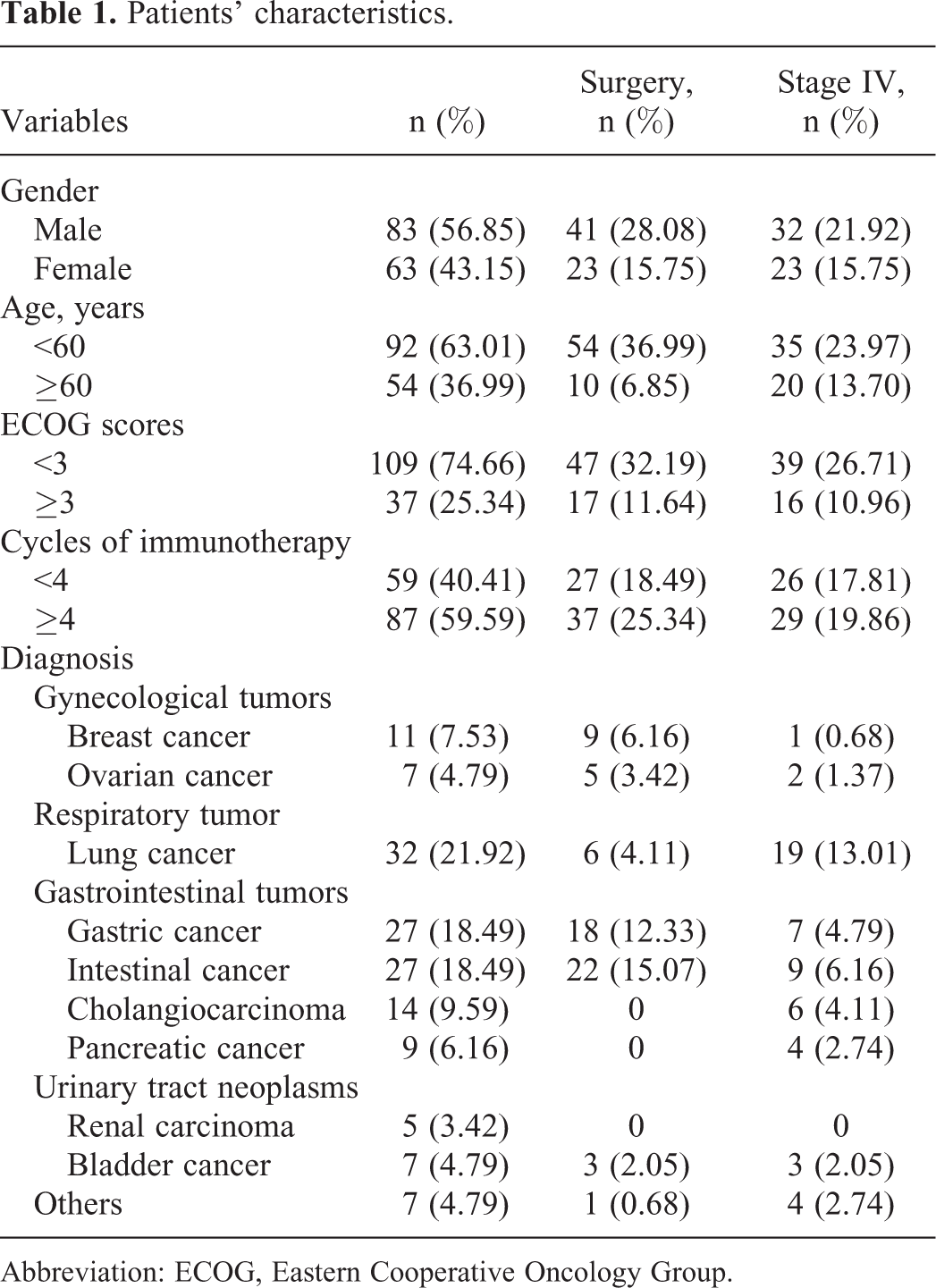
Abbreviation: ECOG, Eastern Cooperative Oncology Group.
Acquisition and Culture of DC, CIK, and DC-CIK Cells
Acquisition and culture of DC
Peripheral blood of 50 to 100 mL was collected and heparinized. Ficoll density gradient centrifugation was used to isolate the peripheral blood mononuclear cells, which were washed and adhered to plastic cell culture flask for 1 hour. Adherent monocytes were then differentiated into DCs by the addition of 500 U/mL recombinant human interleukin 4 (rhIL-4) and 1000 U/mL recombinant human granulocyte macrophage colony-stimulating factor for 7 days. Monocyte-conditioned medium mimic (100×) with 0.5µg/mL tumor necrosis factor α, 0.5µg/mL interleukin (IL) 1β, 15 µg/mL IL-6, and 100 µg/mL prostaglandin E2 was added to the DC culture flask to induce maturation on days 5 and 6, respectively. Matured DCs were harvested on day 7.
Acquisition and culture of CIK
The peripheral blood mononuclear cells isolated using the above-mentioned methods were cultured in fresh serum-free medium with 1000 U/mL interferon γ, at 37°C with 5% CO2 for 24 hours. Then, 100 ng/mL of anti-CD3 antibodies and 1000 U/mL of rhIL-2 were added to the medium. The medium was changed with the fresh IL-2-containing medium every 3 days. Sterility examination of each sample was tested on day 12. Cytokine-induced killer cells were affirmed to be free of bacterial, mycoplasma, or fungal contamination and then harvested on day 14.
Acquisition and culture of DC-CIK
Cytokine-induced killer cells were cocultured with autologous tumor lysate-pulsed DC with a proportion of 5:1 from day 7 to day 14 before final harvest.
Schedule of Immunotherapy Infusions
Cytokine-induced killer cell infusions were received at 2 consecutive days per cycle. Cells were transfused to the patients through superficial vein on days 14 and 16 after apheresis as a complete cycle. Interleukin 2 was administered after cell infusion at a dose of 1 × 106 U/d to promote CIK cell activity.
For DC+CIK protocol, DCs were transfused into patients via axillary lymph node subcutaneous injection on day 7 after apheresis for every cycle, and CIK cells were transfused into patients via superficial vein on days 14 and 16 as a complete cycle. For DC-CIK protocol, DC-CIK cells were transfused into patients via superficial vein on days 12, 14, 16, and 18 after the first apheresis for each cycle.
Schedule of Related Examination
Carcinoembryonic antigen (CEA) and T-cell subsets including CD3+ T lymphocytes, Th (CD3+CD4+T lymphocytes), Tc (CD3+CD8+T lymphocytes), NK (CD3−CD16+CD56+ lymphocytes), and NKT (CD3+CD16+CD56+ lymphocytes) were monitored 1 week before and after immunotherapy. Adverse reactions were noted from subjective description of patients during and after every infusion. Side effects of chemotherapy were also followed.
Statistical Analysis
Data are expressed as mean ± standard deviation unless indicated otherwise. Differences in a continuous variable were assessed by Student t test, or when data distribution was nonnormal, the Mann-Whitney U test was used. Difference is regarded as meaningful when P value was <.05. All data analyses were made by SPSS 21.0 software package (SPSS Inc, Chicago, Illinois).
Results
T-Lymphocyte Subsets Increased Significantly After CIK-Based Immunotherapy
Compared to the measurements prior to CIK treatment, CD3+ T lymphocyte, Th, NKT, and Th/Tc of the participants were increased from 55.67 ± 3.64 to 84.12 ± 5.15, 26.56 ± 4.47 to 42.76 ± 3.68, 1.82 ± 0.58 to 7.08 ± 0.92, and 0.79 ± 3.64 to 1.35 ± 0.20, respectively (P < .001). Carcinoembryonic antigen was decreased from 398.39 ± 219.16 to 127.26 ± 153.41 (P < .001). However, no obvious difference was observed in Tc, B lymphocyte, and NK (P > .05; Table 2).
Comparison of T-Lymphocyte Subsets and CEA Between Before and After CIK-Based Immunotherapy.

Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; CIK cells, cytokine-induced killer cells; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; T, CD3+ T lymphocyte; Th, CD3+CD4+ T lymphocyte; Th/Tc, ratio of CD3+CD4+T lymphocyte and CD3+CD8+T lymphocyte; Tc, CD3+CD8+ T lymphocyte.
aP < 0.05.
Comparison Between Difference Values of T-Lymphocyte Subsets, CEA, and Zero
Difference value (D-value) of CD3+ T lymphocyte, Th, NK, and NKT before and after immunotherapy was distinctly greater than 0 (P < .001). Difference value of CEA was less than 0 (P < .001). There were no statistically significant changes in Tc and B lymphocyte; P values were .08 and .07, respectively (Table 3).
Comparison Between D-Values of T-Lymphocyte Subsets and CEA, and Zero.

Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; D-value, difference value; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; T, CD3+ T lymphocyte; Th, CD3+CD4+ T lymphocyte; Th/Tc, ratio of CD3+CD4+ T lymphocyte and CD3+CD8+ T lymphocyte; Tc, CD3+CD8+ T lymphocyte.
aP < 0.05.
Side effects
The rate of transient fever (varied from 37.3°C to 38.7°C) and chill appeared in 17 patients including 4 patients with lung cancer, 6 patients with esophagus, stomach, and duodenum carcinoma, 1 patient with breast cancer, 1 patient with melanoma, 3 patients with cholangiocarcinoma, and 2 patients with pancreatic cancer, which accounted for 11.6% of all reported cases in this study. This result is similar to those reported recently by others, which discovered a 12.6% rate of the occurrence of transient fever (Table 4). Other adverse events such as nausea, vomiting, anorexia, and hair loss caused by chemotherapy were reduced significantly after treatment compared with those who underwent chemotherapy alone. And other side effects caused by immunotherapy were barely observable in this study.
Occurrence of Adverse Events of CIK-Based Immunotherapy Reported Before.

Abbreviation: CIK cells, cytokine-induced killer cells.
Difference value of T-lymphocyte subsets of the CIK and DC+CIK groups was higher than the DC-CIK group, but D-value of CEA in the DC-CIK group was the highest among the 3 groups. Comparison of T-lymphocyte subset and CEA between the CIK group and the DC+CIK group showed that there was no obvious difference in all variations between the CIK group and the DC+CIK groups (P1 > .05). Comparison of T-lymphocyte subsets and CEA between the CIK group and the DC-CIK group revealed that D-values of T lymphocyte, Th, and NKT of the CIK group were significantly higher than that of the DC-CIK group (P2 < .05). Comparison of T-lymphocyte subsets, CEA between the DC+CIK group and the DC-CIK group revealed that D-values of T lymphocyte, Th, and NKT were significantly higher in the DC+CIK group than in the DC-CIK group (P3 < .05). However, D-value of CEA in the DC-CIK group (absolute value) was higher than the CIK group and the DC+CIK group (P < .05; Table 5).
Comparison of D-Value of T-Lymphocyte Subsets and CEA Among 3 Groups of CIK-Based Immunotherapy.

Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; CIK cells, cytokine-induced killer cells; D-value, difference value; Group 1, CIK group; Group 2, DC+CIK group; Group 3, DC-CIK group; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; P1, P value of the CIK group and the DC+CIK group; P2, P value of the CIK group and the DC-CIK group; P3, P value of the DC+CIK group and the DC-CIK group; T, CD3+ T lymphocyte; Th, CD3+CD4+ T lymphocyte; Tc, CD3+CD8+T lymphocyte.
aP < 0.05.
Enhancement of T-lymphocyte subsets, D-value of T-lymphocyte subsets, and CD8+/CD4+ with increased cycles of immunotherapy
According to Figure 1, CD3+ T lymphocyte and Th were mounting to maximum after 4 cycles of immunotherapy. Difference values of CD3+ T lymphocyte and Th were at the highest after 4 cycles of immunotherapy (Figure 2). Similarly, CD8+T/CD4+T also began to decrease after 4 cycles of immunotherapy (Figure 3).

T-lymphocyte subsets increase with increased cycles of immunotherapy.

Change in trend of D-value of T-lymphocyte subsets with increased cycles of immunotherapy.

Change in trend of CD8+T/CD4+ T cells with increased cycles of immunotherapy.
Comparison Between Groups of Patients Who Were Subdivided According to Diagnosis
All patients were divided into 4 groups based on the diagnosis: gastrointestinal tumors, respiratory tumor, gynecological tumors, and urinary tract neoplasms. Comparison of D-value of T-lymphocyte subsets and CEA among the 4 groups showed that there was no significant difference (P > .05; Table 6).
Comparison of D-Value of T-Lymphocyte Subsets and CEA Among Different Kinds of Cancers.
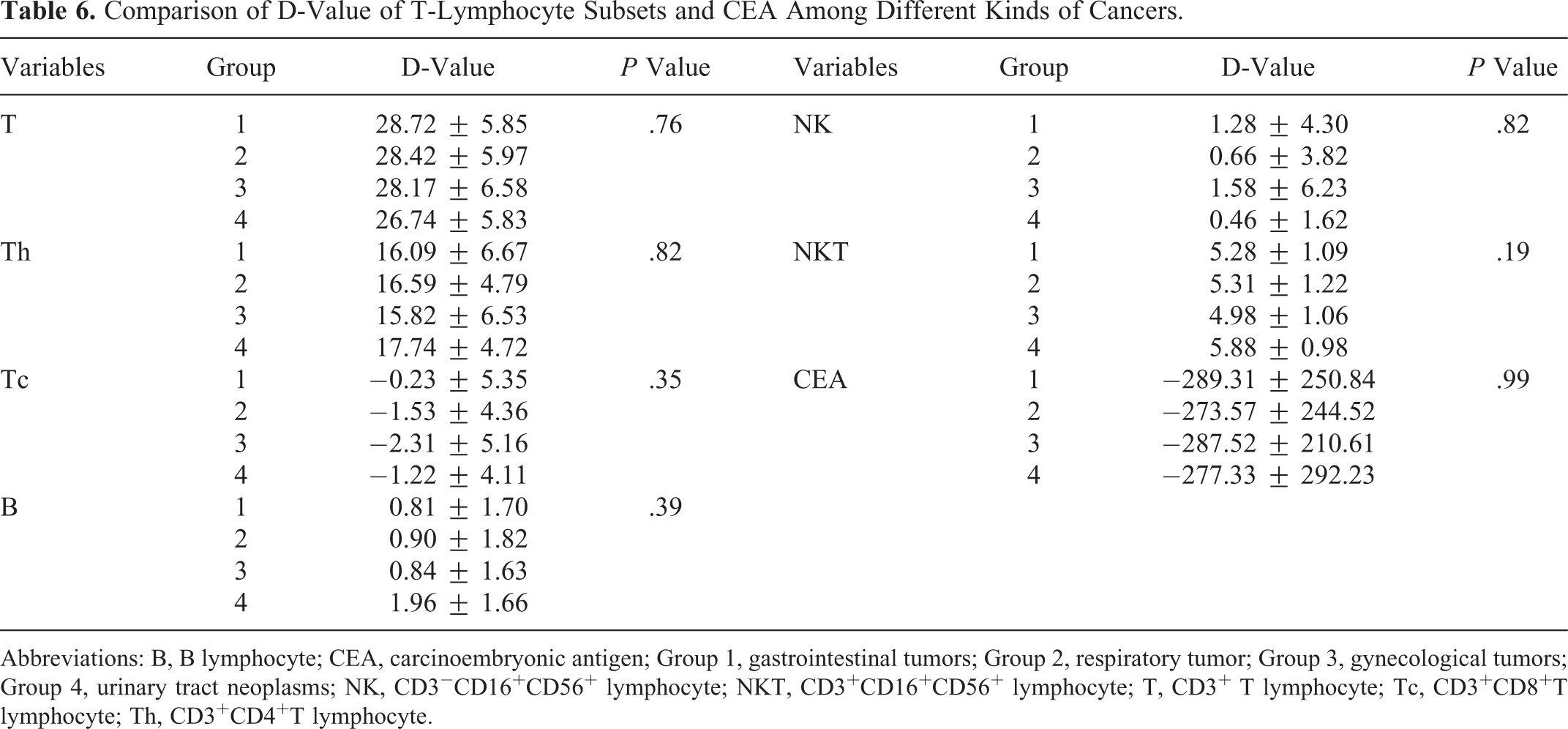
Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; Group 1, gastrointestinal tumors; Group 2, respiratory tumor; Group 3, gynecological tumors; Group 4, urinary tract neoplasms; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; T, CD3+ T lymphocyte; Tc, CD3+CD8+T lymphocyte; Th, CD3+CD4+T lymphocyte.
Comparison of D-value of T-lymphocyte subsets and CEA with surgery or not in gastrointestinal tumors
Patients with gastrointestinal tumors were divided into 2 groups based on whether the participant was surgically intervened. Difference value of T lymphocyte and Tc of patients who underwent surgery was higher than that of those without surgery (P < .001 and P = .042, respectively). However, D-values of Th, B lymphocyte, NK, NKT, and CEA were not significantly distinct (P > .05; Table 7).
Comparison of D-Value of T-Lymphocyte Subsets, CEA With Surgery or Not in Gastrointestinal Tumors.
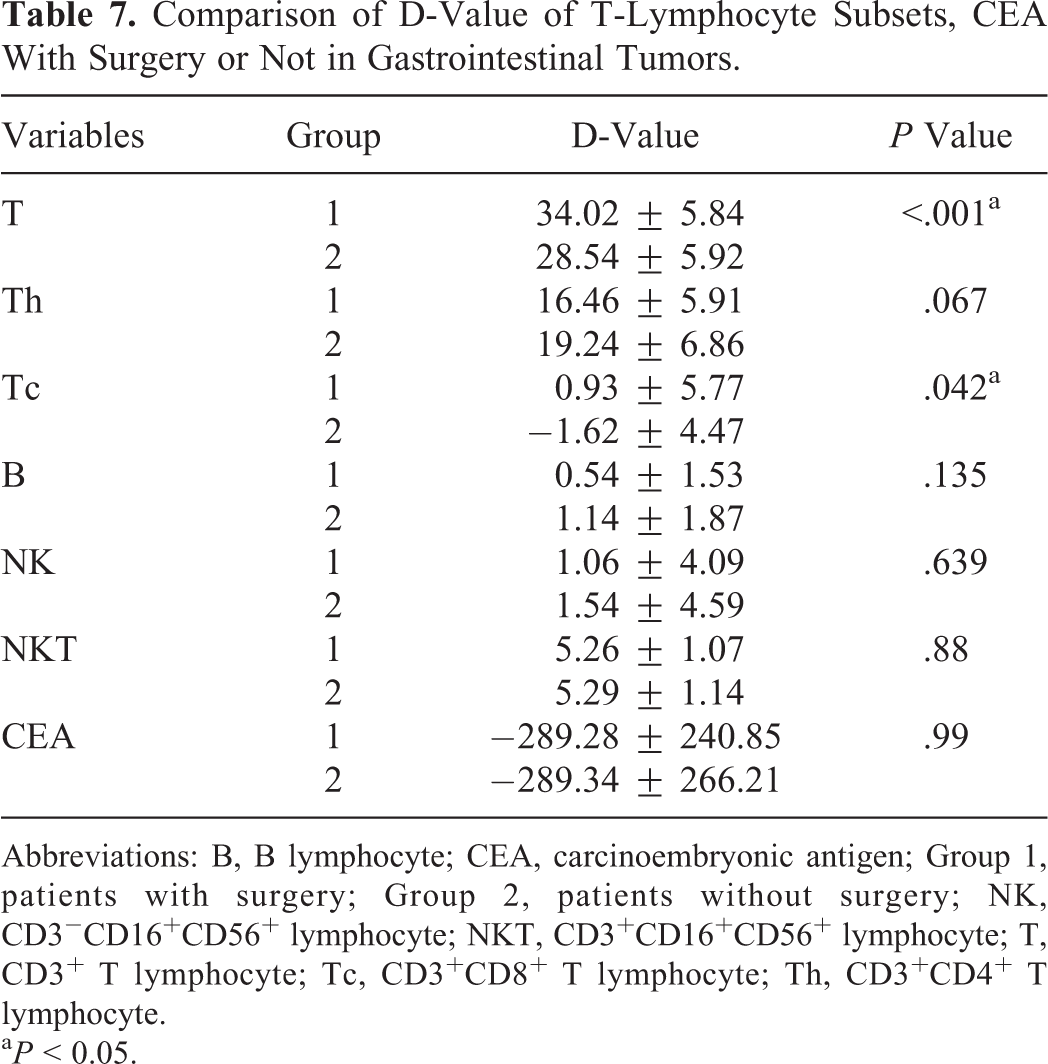
Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; Group 1, patients with surgery; Group 2, patients without surgery; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; T, CD3+ T lymphocyte; Tc, CD3+CD8+ T lymphocyte; Th, CD3+CD4+ T lymphocyte.
aP < 0.05.
Comparison of D-value of T-lymphocyte subsets and CEA between stage III and stage IV in gastrointestinal tumors
Patients with gastrointestinal tumors were divided into 2 groups based on different stages: group stage III and group stage IV. Difference value of T lymphocyte of patients in group stage III was higher than that of patients in group stage IV (P < .001). Difference value of CEA (absolute value) in group stage III was higher than that of patients in group stage IV (P = .017). However, D-values of Th, B lymphocyte, NK, and NKT were similar (P > .05; Table 8).
Comparison of D-Value of T-Lymphocyte Subsets and CEA Between Stage III and Stage IV in Gastrointestinal Tumors.

Abbreviations: B, B lymphocyte; CEA, carcinoembryonic antigen; Group 1, group stage III; Group 2, group stage IV; NK, CD3−CD16+CD56+ lymphocyte; NKT, CD3+CD16+CD56+ lymphocyte; T, CD3+ T lymphocyte; Tc, CD3+CD8+ T lymphocyte; Th, CD3+CD4+ T lymphocyte.
aP < 0.05.
Discussion and Conclusion
In the past 20 years, CIK-based immunotherapies have been proved to be effective in a number of cancer types such as metastatic renal cell carcinoma, 30 gastric or colorectal adenocarcinoma, 2 and lung cancer. 31 Cytokine-induced killer cells are a heterogeneous cell population, including CD3+CD56+ cells, CD3+CD56− cells, and CD3−CD56+ cells. 32 Among them, CD3+CD56+ cells (NKT) are primarily responsible for non-MHC-restricted antitumor activity. 33,34
CD3−CD56+ cells behave similarly to conventional NK cells and express classical NK cell receptors. 35 Measurement of T-lymphocyte subsets can represent the clinical effect of CIK-based immunotherapy. Weng et al 36 examined the alteration in levels of T-lymphocyte subsets in peripheral blood of patients by flow cytometry and found that the percentages of CD3+ T, CD3+CD56+ T cells, and CD4+/CD8+ ratio were increased after CIK cell infusions (P < .05).
In our study, CD3+ T lymphocyte, Th, NKT, and Th/Tc were increased after immunotherapy (P < .001). Furthermore, CEA was decreased significantly after CIK cell infusions (P < .001; Table 2). And D-values of CD3+ T lymphocyte, Th, NK, and NKT were distinctly greater than 0 (P < .001). Difference value of CEA was obviously less than 0 (P < .001; Table 3). The population of T-lymphocyte subsets was increased by CIK cell infusions. It was suggested that the anti-tumor function of CIK cells was activated by binding with target cells. In other words, cytotoxicity against tumor cells was activated when the surface adhesion molecule leukocyte function associated antigen 1 (LFA-1) on CIK cells binded to LFA-1 ligands expressed on susceptible tumor cells. 37,38 Following adhesion, NK cell receptors, which are highly expressed on tumor cells, bind to their ligands, resulting in CIK cell activation that leads to degranulation and cytotoxicity against tumor cells. 39 Finally, tumor cell apoptosis by Fas ligand via the Fas signaling pathway was initiated. 33 Moreover, the migration and homing of CIK cells to tumors, tumor-draining lymph nodes, and spleen tissues 40,41 can also enhance the cytotoxic potential of CIK cells.
Cellular immunity rather than killing malignant cells directly is the main mechanism of antitumor of CIK-based immunotherapy. In fact, CD3+ T lymphocytes, CD4+ T lymphocytes, and CD4+/CD8+ were lower in patients with cancer than that in healthy controls, and CD8+ T was increased in patients with cancer. These changes have become a valuable clinical immunosuppression index in treating patients with cancer. 42 For that reason, immunosuppression may be one of the most important factors for the development of malignant tumors, and improving cellular immunity by T-lymphocyte infusions could be the key strategy for antitumor activity. Increased ratio of CD4+/CD8+ T cells could be a target for improved antitumor ability and reduced risk of tumor recurrence. 43 Numbers of clinical studies with increased T-lymphocyte subsets can also add the possibility of our conjecture. 44 –46
Literature search of recent articles through PubMed revealed 1878 cases of malignant solid tumors treated with CIK-based immunotherapy for a comparison of the occurrence of adverse event. Table 4 shows transient fever is the most common event (about 12.24%), and most disappeared with or without treatment. This observation was similar to ours, in which 17 (11.64%) of the 146 patients had transient fever including 4 patients with lung cancer, 6 patients with esophagus, stomach, and duodenum carcinoma, 1 patient with breast cancer, 1 patient with melanoma, 3 patients with cholangiocarcinoma, and 2 patients with pancreatic cancer. Eleven of them attained normal temperature without any medical intervention. This suggested that CIK-based immunotherapy is safe and feasible for patients with solid cancer. Evidence provided by some clinical researches suggested that the capability of CIK-based immunotherapy could reduce or relieve adverse reactions caused by chemotherapy. 47 In our study, subjective description of patients’ own status was obtained by follow-ups after chemotherapy and CIK-based immunotherapy. It was assembled that adverse events such as nausea, vomiting, anorexia, and hair loss caused by chemotherapy were significantly reduced after CIK-based immunotherapy. It may be related to increased numbers of T lymphocytes through CIK infusion. However, the molecular mechanism was not clear.
Comparison of T-lymphocyte subsets and CEA between the CIK and DC+CIK groups showed that there was no clinically significant difference in all variations between the 2 groups (P > .05). When compared to the DC-CIK group, D-values of T lymphocyte, Th, and NKT were higher in the CIK group than that of the DC-CIK group (P < .05; Table 5). However, it’s not clear whether DC-CIK/DC+CIK is superior to CIK cells alone. Dendritic cell is the most powerful APC presenting specific antigen to T cells through the MHC molecules. Theoretically, CIK cells should exert better clinical performance in the presence of DC cells due to increased specificity, but our result is not conclusive; the clinical efficiency of CIK, DC-CIK, and DC+CIK in solid tumor requires further investigation.
A study by Jia et al aimed to evaluate the CIK cell therapy combined with chemotherapy in patients with advanced non-small cell lung cancer. It was revealed that the risk of adverse outcomes in patients receiving 4 cycles of CIK therapy was 0.38-fold (95% confidence interval: 0.14-1.13) compared to those of patients receiving less than 4 CIK therapy cycles. 48 In our observation, CD3+ T lymphocyte and Th were increasing remarkably from the fourth cycle to the sixth cycle (Figures 1 and 2), and CD8+/CD4+ decreased dramatically from the fourth cycle to the sixth cycle immunotherapy (Figure 3). Therefore, a minimum of 4 cycles of CIK treatment should be suggested in order to obtain better clinical efficiency.
According to our results, there was no statistically significant difference in patients with or without surgical intervention, except for the D-value of Tc lymphocytes. Ideally, CIK treatment after surgical removal of tumor cells should result in a much better clinical recovery, which our investigation failed to conquer. Similarly, better CIK activity was observed in stage III patients than in stage IV, evident by the observation of higher D-value of CD3+ T lymphocytes and CEA. Although these results were in accordance with our hypothesis, larger difference in all variables is required for a conclusive summary. In conclusion, CIK-based immunotherapy is capable of recovering cellular immunity, relieving chemotherapy adverse reactions, and improving quality of life without sever adverse effects. Four or more than 4 cycles of treatment should be suggested for better clinical outcome. And there was no significant difference of clinical efficiency between CIK and DC+CIK. DC-CIK was superior to CIK and DC+CIK in the fact of decreasing CEA.
Footnotes
Abbreviations
Authors’ Note
Hongjin Chu and Fengcai Du contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (project number: 30801338, 81071758), Natural Science Foundation of Shandong Province (2015GSF118142, ZR2015HL069), Yantai Science and Technology Program (2015WS018), and Yantai Yuhuangding Hospital Initiative Foundation for Young Scientist (201402).