
Abstract
At external beam radiotherapy, stereoscopic X-ray imaging system is responsible as tumor motion information provider. This system takes X-ray images intermittently from tumor position (1) at pretreatment step to provide training data set for model construction and (2) during treatment to control the accuracy of correlation model performance. In this work, we investigated the effect of imaging data points provided by this system on treatment quality. Because some information is still lacking about (1) the number of imaging data points, (2) shooting time for capturing each data point, and also (3) additional imaging dose delivered by this system. These 3 issues were comprehensively assessed at (1) pretreatment step while training data set is gathered for prediction model construction and (2) during treatment while model is tested and reconstructed using new arrival data points. A group of real patients treated with CyberKnife Synchrony module was chosen in this work, and an adaptive neuro-fuzzy inference system was considered as consistent correlation model. Results show that a proper model can be constructed while the number of imaging data points is highly enough to represent a good pattern of breathing cycles. Moreover, a trade-off between the number of imaging data points and additional imaging dose is considered in this study. Since breathing phenomena are highly variable at different patients, the time for taking some of imaging data points is very important, while their absence at that critical time may yield wrong tumor tracking. In contrast, the sensitivity of another category of imaging data points is not high, while breathing is normal and in the control range. Therefore, an adaptive supervision on the implementation of stereoscopic X-ray imaging is proposed to intelligently accomplish shooting process, based on breathing motion variations.
Keywords
Introduction
In radiotherapy, the final purpose is to deliver the prescribed radiation dose to the entire volume of tumor while keeping the adjacent normal tissues safe against high radiation dose. In external beam radiotherapy (EBRT), several strategies were developed to minimize the planning target volume (PTV) margin taking into account target localization precision during treatment and also between treatment fractions. 1 For PTV minimization, serious concerns raise for tumors located at thorax and abdomen regions and move mainly due to respiration. In this condition, considerable margins seem to be added around the PTV as treatment site to cover the tumor displacement, and therefore, normal tissues surrounding the target may irradiate unnecessarily. 2
For compensating tumor motion error, many research efforts have been done to save nearby normal tissue against high dose and to adequately conform dose distribution onto moving tumor that yields proper target localization and dose delivery modification. The simplest way is breath holding to immobilize the tumor motion that requires patient cooperation. 3 –5 As an alternative, respiratory gating strategy was proposed to reduce PTV margin by limiting radiation exposure to a predefined phase of the breathing cycle. 6 –9 The third solution that is under development is to conform therapeutic irradiation on moving target continuously by following the target using dynamic beam such as robotic radiosurgery system. 9 –12 In the 2 latter cases, tumor motion must be tracked as real time using additional motion monitoring systems mounted at treatment room. 13
Real-time tumor tracing at both respiratory gating and tumor tracking strategies is implemented using continuous X-ray imaging such as fluoroscopy to directly track clips implanted near or inside tumor volume 10,14,15 or indirectly by means of an external respiratory signal extracted from surrogates to infer the tumor position. 16 –19 Fluoroscopy X-ray imaging technique seems to be the best method for direct monitoring of moving targets, but additional imaging dose received by patient in this method may be harmful for patients, which causes serious side effects. 20 As a solution, external surrogates technique was proposed to keep patient away from additional imaging dose in comparison with fluoroscopy system. In this technique, tumor position information is obtained by correlating internal tumor motion with motion data of external markers located on thorax and abdomen regions of patient’s skin using a consistent correlation model. 21 –29 Accordingly, the correlation model must be configured at pretreatment step using training data set. This data set includes motion information of external markers and internal tumor at synchronized fashion using (1) noninvasive optical tracking system (OTS) and (2) stereoscopic X-ray imaging systems, respectively. 16 –18 Although the correlation model was configured at pretreatment step, it is ready to predict tumor position over treatment time, feeding only by external marker motion as input. In this method, although there are uncertainties/errors associated with the correlation between external/internal data, the well-established procedure is widely used clinically. 16,18 A comprehensive study has already been done on the performance accuracy of available linear and nonlinear correlation models, considering the robustness and weakness of each model in our previous studies. 22
At radiotherapy with external surrogates, extracting tumor position information by means of stereoscopic X-ray imaging system must be intermittently continued during treatment for reaching 2 aims. First, the performance accuracy of the model is periodically controlled to be in acceptable range of positional uncertainty error by comparing model output with new position information of the tumor detected by X-ray imager, as benchmark. Second, the model has an opportunity to be updated or rebuilt using the most recent information of tumor motion data point and corresponding external markers data set. 22,30 The paired data points is accumulated to former external–internal training data set, and training data set with new added member is reshaped. Therefore, model update can be done using new synchronized external–internal data points to predict tumor motion more precise. It should be noted that the parameters of data clustering and model inference system are renewed during model updating. Several mathematical strategies can be utilized for model update using new training data set.
Apart from mathematical methods implemented for model reconstruction, some assessment is still lacking on the effects of imaging data points on tumor tracking accuracy. This attractive challenge includes the number of imaging data points (NID) required at pretreatment step and also during treatment. Moreover, the shooting time of X-ray imaging system for catching each new imaging data point is another challenging issue that can be investigated. In this study, we are interested to comprehensively investigate the role of stereoscopic X-ray imaging system on treatment quality enhancement for a group of real patients. This investigation is started from pretreatment step while initial training data set is gathering for model configuration and also during treatment while (1) model performance is testing and (2) model update is implementing, both using new captured external/internal data points. Moreover, additional imaging dose delivered by means of X-ray imaging system is also considered in this work. In ideal form, tumor motion must be tracked by means of a proper correlation model with highest targeting accuracy using the least imaging data points to minimize additional imaging dose received by patients according to ALARA (As Low As Reasonably Achievable) principle. Therefore, we expect to realize a trade-off between the performance accuracy of correlation model and additional imaging dose, both affected by stereoscopic X-ray system as imaging data points provider.
We then proposed that the test for tumor tracking accuracy may be done intelligently over treatment time in regard to regular periodic testing that is accomplished currently. Therefore, the time interval between the 2 consequent X-ray imaging data points will not necessarily constant and can change depending on breathing motion variations. By this way, the probability of model performance testing is increasing while external markers representing respiration signal record abnormal range of breathing motion amplitude.
In this work, motion database of a group of real patients treated with CyberKnife Synchrony module was utilized. 16 –18 We used adaptive neuro-fuzzy inference system (ANFIS) in synthetic form as correlation model for tumor motion tracking. 30 Among several available models, ANFIS was chosen due to its robustness with respect to state-of-the-art systems that has already been proven at our previous works. 24,30,31 Final analyzed results represent that the construction of utilized correlation model at pretreatment step and its performance during treatment depend highly on the NID and their capturing time. The degree of importance of some imaging data points is high, while their absence yields wrong motion tracking and this is due to high variability of breathing motion at some erratic cases. Moreover, there is a significant compromise between (1) tumor tracking accuracy affected by the number of stereoscopic X-ray shots and (2) the amount of additional imaging dose received by patients.
Materials and Methods
Patients Database and Motion Properties
In this work, the external–internal motion data set including respiratory and tumor position information of real patients treated with Synchrony Respiratory Tracking System integrated with the CyberKnife robotic linear accelerator (Accuray Incorporated, Sunnyvale, California) was utilized. 16 –18 The patient database is made available by the Georgetown University Medical Center (Washington, DC), and our patients in this study were selected randomly among total patient population with dynamic tumors in thorax and abdomen regions. External motion data set is gathered using an infrared OTS as responsible to monitor (around 25 Hz) 3 external markers located on a vest that covers rib cage and abdomen regions (Figure 1, upper right block). Therefore, external data consist of 3-dimensional (3D) position information of each marker as function of time. External motion data set represents respiration signal. In contrast, internal motion data set is 3D spatial motion of a clip implanted inside or near a tumor volume as representative of tumor motion. In some cases, a natural anatomical landmark with high contrast property (eg, bony structures) can be selected as internal marker. Internal motion data set is obtained by means of stereoscopic X-ray imaging system that visualizes implanted clip (Figure 1, upper left block). External–internal motion as paired data set is saved as log files in ASCII format. 18 It should be noted that the CyberKnife Synchrony system is able to track tumor motion relying on an external–internal correlation model between the motion of external infrared markers and internal implanted clip. 10 The time latency of CyberKnife robotic system ranges from 115 to 192.5 ms that is not problematic during treatment regarding model execution time and breathing cycle frequency. Table 1 reports the motion range of 3D external markers and implanted clip plus treatment time.

Block diagram of correlation model. Red pathway: model construction, green pathway: model update, and black pathway: model performance.
Motion Features of Tumors and External Markers of Selected Patients With their Treatment Time.

Abbreviations: SI, Superior-Inferior; LR, Left-Right; AP, Anterior-Posterior; LLL, Left Lower Lung; RLL, Right Lower Lung; RUL, Right Upper Lung.
Adaptive Neuro-Fuzzy Inference System Correlation Model
In this work, an ANFIS was utilized as a correlation model to adjust the position of the robotic linear accelerator according to the predicted tumor position. The implemented correlation model is a modified synthetic ANFIS model that was proposed at our recent study as most appropriate model including several data clustering algorithm for data mining. 30 The aim of choosing the modified version of synthetic ANFIS model is using the robustness of neuro-fuzzy inference system in tumor motion tracing with least uncertainty error, 31 which makes it adaptively suitable for our incomplete and highly variable patient motion data set on a case-by-case basis.
The proposed ANFIS model was developed in MatLab (The MathWorks Inc, Natick, MA) using the embedded toolboxes of neural network and fuzzy logic. The configuration, performance, and updating of this model have been illustrated in Figure 1.
As shown in this block diagram, the correlation model must be configured initially in pretreatment step before therapeutic beam irradiation using training data set (Figure 1, red pathway). In this step, internal tumor motion is correlated with external marker data set by classifying model learning and if-then rules extraction. Training data set that is gathered few minutes before treatment includes external marker motion data set in X, Y, and Z directions as the input of the model and the corresponding motion data set of internal implanted clip as model output in a synchronized form. Concerning implanted clip, it should be noted that at both fluoroscopy and external surrogate-based radiotherapy, since tumor volume has no enough visibility at taken images, internal marker(s) is implanted inside or near the tumor to represent a given point of tumor position with contrast enhancement.
The external motion data set is then arranged in a matrix with 9 columns representing the xM(t), yM(t), and zM(t) of each marker over time, where the number of rows (n) depends on data sampling time during treatment. In the same fashion, the internal clip data are written in another matrix with 3 × n size, depicting the xc(t), yc(t), and zc(t) of tumor position (Figure 2).

Matrices of external markers data set (left side) and internal clip data set (right side).
As seen in this figure, training data set has been shown in pretreatment step ranging from t1 to tn time at upper side of both matrices. When ANFIS was built at pretreatment step using training data set, the model is ready to track tumor motion as output, feeding only 3D external marker motion as input (Figure 1, black pathway). As illustrated in Figure 2, this part is started from tn+1 to tn+m of total treatment time.
Adaptive Neuro-Fuzzy Inference System Mathematical Structure
Adaptive neuro-fuzzy inference system mathematical architecture includes 5 layers. 31 Layer 1 consists of input nodes representing membership degrees. The value of each degree is determined by means of specific functions known as membership functions (MFs). These functions are generated by means of mathematical properties of clustered data implemented by different clustering algorithms on initial training data set. Data clustering 32,33 is utilized to organize a collection of data set into n clusters based on similarities among them. Several efforts had been done on different data clustering algorithms for MFs generation, whereas choosing proper strategies yields high accuracy of ANFIS model performance. 30 In fact, at layer 1, the participation magnitude of each input data point (external marker motion) is defined using MFs as graphical representation. In this work, we utilized a synthetic form of ANFIS model that includes several available data clustering algorithms to use the robustness of each clustering strategy, adaptively for each respiration motion pattern. 30 In layer 2, a numerical value known as firing strength is determined by means of AND logic operator (minimum selection criteria) using n if-then rules extracted according to the number of clusters. Third layer calculates the ratio of each ith rules’ firing strength to the sum of all rules’ firing strength, in their normalized form. Layer 4 is responsible to determine the contribution of each rule toward the total output. Layer 5 known as defuzzification step represents a single overall output by summing all incoming signals calculated at previous steps using centroid calculation method. It should be noted that in the proposed method, nonlinear premise parameters are tuned iteratively proportional with the error value emerged in correlating input–output data set in the fuzzy inference system of ANFIS structure.
Testing and Updating ANFIS Correlation Model
In order to guarantee the performance accuracy of our strategy in tumor tracing, the utilized model output must be checked with real position of dynamic tumor during treatment as benchmark, periodically. To do this, real information of tumor position is obtained with intermittent X-ray imaging system during treatment and the model output is then compared with detected position. As seen in Figure 2, a typical test data point has been shown at time tn+i during treatment time. The comparison result must be in acceptable range of positional uncertainty error, otherwise tumor motion tracking is not accurate and the therapeutic irradiation must be stopped.
Moreover, ANFIS model can be updated (rebuilt) using new tumor motion data point paired with corresponding external marker motion taken by OTS at the same time. The achieved new internal–external data point is added to initial training data set for finding new parameters of data clustering and inference system of ANFIS correlation model (Figure 1, green pathway). This helps us to trace tumor motion with a renewed model constructed by most recent external–internal motion information. Adding new paired external–internal data point will result new training data set as a requirement for configuring the model, more precise.
New training data set can be formed as two (1) accumulation and (2) nonaccumulation (or fresh) styles. In the first style, the number of new training data set is intermittently accumulated by adding new data points taken at each X-ray imaging shoot. In the fresh mode, when new data point is added to the former training data set, the oldest belonging data point of training data set is automatically rejected from the group at the same time, and therefore, the number of total training data set is always constant including recent information of tumor and external marker motions, correspondingly. It should be noted that in the second style, the number of new training data set can also be related to the number of initial training data set (gathered at pretreatment step) with a constant ratio.
At both accumulation and fresh modes, when paired external–internal data point participates as new member of training data set, new 3D pattern of data distribution is obtained, accordingly. This causes different data clustering strategies with new parameters extracted from MFs. Figure 3 graphically illustrates the role of new added data point on data set distribution and therefore cluster center for a typical marker.
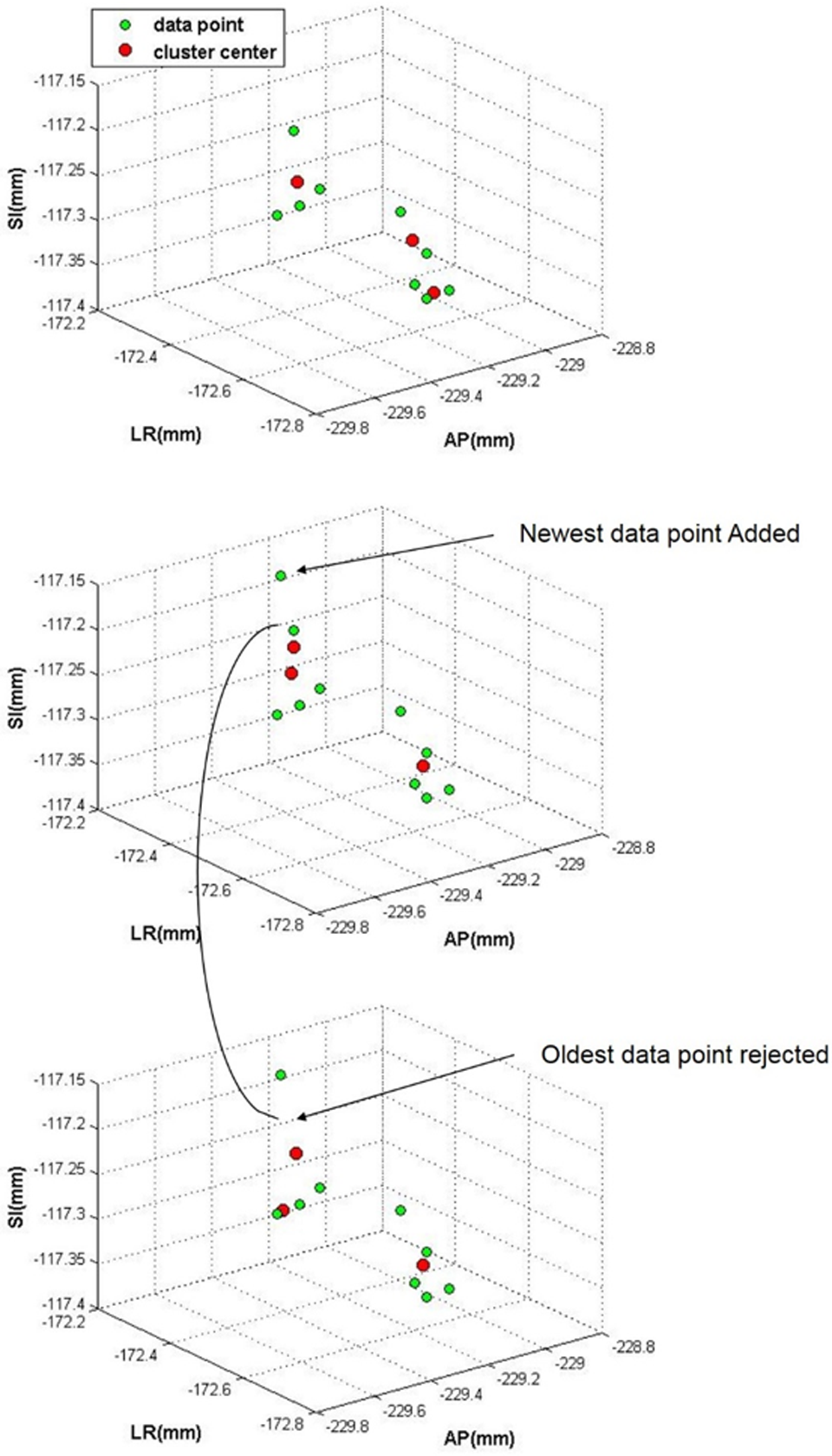
Three-dimensional (3D) spatial distribution of data points (green spots) and cluster center variations (red spots) implementing accumulation (middle panel) and fresh modes (lower panel).
In this figure (upper side), data set including 9 typical data points was grouped into 3 clusters. The cluster centers (red points) were distributed on the basis of data points’ spatial distribution density. In the middle side of this figure, a new data point was added to the data set while keeping other data points save according to accumulation mode principle. In this condition, the cluster centers moved to new spatial positions. In the lower panel of this figure, the oldest data point taken at first time of data sampling process was removed and the number of total data points remains constant with 9. This condition illustrates fresh mode and cluster centers move to new positions. Accordingly, MFs’ parameters, as key components of ANFIS performance, change remarkably by changing cluster centers. Therefore, applying each mathematical mode can directly cause performance accuracy of ANFIS correlation model.
In this work, the performance accuracy of ANFIS model, reconfigured by both accumulation and fresh modes, was quantitatively assessed for tumor motion tracking. As a next step, we calculated targeting accuracy of our model using different NID. In contrast, additional dose delivered by imaging system is also calculated for each patient relatively. These calculation are then repeated for each patient of our patient group. We then assessed the consequences of shooting time for capturing imaging data points during treatment for 2 erratic and normal cases, while respiration motion is highly variable and in control, respectively.
Results
In our patient group, training data set ranges from 4 to 27 data points and imaging data set taken during the treatment time varies between 40 and 106 data points. In some cases, the numbers of training data (NTDs) points may be incomplete to represent a proper pattern of a whole breathing cycle as requirement for model learning. This drawback may reduce the accuracy of motion tracking mainly at the initial part of total treatment time. Table 2 shows root mean square error (RMSE) of correlation model as tumor tracking error versus different NTDs for 4 given patients while their NTD is low. In this table, RMSE was obtained using model output as predicted values and corresponding imaging data points as benchmark values calculated at the initial time interval of total treatment time. This time interval was assumed to be numerically equal with pretreatment time for each patient. As seen in this table, prediction model error is increasing while the NTD is reduced from 8 to 5.
The Effect of Few NTD on 3D RMSE of Correlation Model for 2 Patients.

Abbreviations: 3D, 3-dimensional; NTD, number of training data points; RMSE, root mean square error.
Table 3 represents RMSE of ANFIS correlation model while implementing 2 mathematical accumulation and fresh modes for model reconstruction. Moreover, required time for model reconstruction has been taken into account using fresh mode versus accumulation mode relatively. The averages of 3D RMSE for overall 7 patients are 1.49 and 1.46 mm implementing accumulation and fresh modes, respectively. As seen, model accuracy is almost same using both modes, but model reconstruction time is different. Since, tumor motion tracking must be done as real time during irradiation, model reconstruction during each update step must be taken into account to be less than OTS data sampling rate. It should be noted that based on our computational time analysis, model reconstruction time is always less than data sampling time at both fresh and accumulation modes using our in-room computer system.
3D RMSE of Correlation Model Constructed at 2 Accumulation and Fresh Modes Over 4 Patients.

Abbreviations: 3D, 3-dimensional; NTD, number of training data points; RMSE, root mean square error.
In order to investigate the effect of X-ray imaging data set on ANFIS model performance during the treatment, different NIDs were considered. Figure 4 shows RMSE of model output at 4 values of NID, while each NID varies relatively with 1:2, 1:3, and 1:4 ratio versus reference. This calculation was repeated for 18 patients at different NIDs.

Three-dimensional root mean square error (RMSE) of correlation model reconstructed with different number of imaging data points.
As seen in this figure, the 3D RMSE is approximately same for 4 cases and generally increases while NID decreases. Since, NID is obtained using stereoscopic X-ray imaging system as invasive method, different values of NID can be important for us due to additional imaging dose received by patients. Therefore, in this study, additional imaging dose received by patients was also considered. Table 4 shows the average of 3D RMSE of correlation model and relative imaging dose over all patients at 4 conditions while NID ranges from total to quadrant. As seen in this table, although the best accuracy of tumor tracking is achieved while using higher NID, additional imaging dose received by patients is maximized, which may be in oppose with ALARA principle. Reconsidering Figure 4, in some cases (eg patient 1, 3, 7, and 11), although NID value is reduced remarkably, RMSE or model performance error is almost unchanged, whereas additional imaging doses have been decreased. This point can be considered as beneficial issue for patients who receive less imaging dose while their tumor tracking can be done reasonably with maximum accuracy.
Average of 3D RMSE of ANFIS Model Over Selected Patients Using Different NIDs and Corresponding Total Imaging Dose at Each Condition.

Abbreviations: ANFIS, adaptive neuro-fuzzy inference system; 3D, 3-dimensional; NTD, number of training data points; RMSE, root mean square error.
As seen in Figure 4, some cases with least variation against NID have low RMSE. In other words, these patients are normal in breathing. In contrast, for erratic patients with larger error, RMSE varies against NID remarkably. It may be concluded that while patient breathing is not almost stable, a large NID must be taken during treatment to (1) provide required guarantee about model performance accuracy and (2) rebuild model structure rapidly for better tumor tracking. Therefore, an adaptive supervision can be implemented on respiratory system by means of stereoscopic X-ray imaging. By this way, X-ray shooting of stereoscopic system will be intelligently increased while breathing phenomena are getting out of normal stability condition. In order to investigate this issue, we focused on 8 patients considering a fraction of total imaging data points taken at (1) crucial time while breathing motion is unstable (sensitive imaging data points) and (2) normal time while breathing is almost normal (insensitive imaging data points). Patients were chosen without any concern to tumor type and its site. We calculated RMSE of the model by removing sensitive and insensitive imaging data points and compared the obtained results with the same calculations while using total imaging data set.
Tables 5 and 6 show the effect of sensitive and insensitive data points on model performance accuracy. As seen in Table 5, sensitive data points are important during tracking, while their absence will increase 3D RMSE. But the insensitive points don’t play important role at model accuracy and RMSE variations of model is almost negligible by removing them (Table 6). It should be noted that the fourth column of these tables (Available Imaging Data Points) is obtained by subtracting the number of sensitive (or insensitive) imaging data points from the total NID.
3D RMSE of Correlation Model Reconstructed by Total and Available Imaging Points.a

Abbreviations: 3D, 3-dimensional; NTD, number of training data points; RMSE, root mean square error.
aAvailable imaging data points = total imaging data points − sensitive imaging data points.
3D RMSE of Correlation Model Reconstructed by Total and Available Imaging Points.a

Abbreviations: 3D, 3-dimensional; NTD, number of training data points; RMSE, root mean square error.
aAvailable imaging data points = total imaging data points − insensitive imaging data points.
For better understanding of this issue, Figures 5 and 6 visually illustrate the performance of correlation model during a part of treatment time in the presence (upper panels) and absence (lower panels) of sensitive and insensitive imaging data points for 2 given patients, respectively. These figures show correlation model output as tumor motion (red line) in the anterior–posterior direction and some green spots as imaging data points detected by stereoscopic X-ray imaging system. Four consequent imaging data points (surrounded inside the dashed ellipse) were chosen typically as sensitive and insensitive data points. As seen in the upper panel of Figure 5, the presence of these points yields correct tracking while their absence results wrong tracking of tumor motion in an incorrect trajectory. As shown in the lower panel of Figure 5, the wrong motion tracking is continued with reaching to a new arrival imaging data point. In this time, the model is rebuilt and put in the right trajectory of tumor motion. In contrast, as seen in Figure 6, correlation model is almost correct at tumor tracking in the presence (upper panel) and absence (lower panel) of insensitive imaging data points. This is due to normal motion variation of patient breathing shown in Figure 6 in comparison with high variability of motion respiration of given patient shown in Figure 5.

Tumor tracking at the anterior–posterior (AP) direction over a fraction of treatment time (red line) and sensitive imaging data points.

Tumor tracking at the anterior–posterior (AP) direction over a fraction of treatment time (red line) and insensitive imaging data points.
Discussion
In EBRT, stereoscopic X-ray imaging system is responsible to give tumor position information as main component for motion tracking. Taking X-ray images by this system is intermittently continued during treatment to (1) control correlation model performance by comparing model output with detected tumor position and (2) to rebuilt model structure using most recent information of tumor and external marker motion. It should be noted that the model is rebuilt by renewing the mathematical parameters utilized at data clustering and fuzzy logic-based inference system of model structure. This may be helpful for us to use most precise prediction model at each update step.
In this study, we first assessed the effect of NTDs on model construction properly. As resulted from Table 2, the number of training data set collected at pretreatment step must be large to represent a proper pattern of whole breathing cycle. Otherwise, model learning and therefore rule extractions cannot be done precisely. We then assessed the effect of 2 available model reconstruction fashions based mathematically on accumulation and fresh technique. We realized that model performance accuracy is almost same using both indicated techniques during model reconstruction. It should be noted that although time intensive for model update is larger implementing accumulation rather than fresh, both techniques require less computational time against data sampling of OTS from external markers. Based on our recent quantitative assessment on ANFIS model reconstruction and execution time, there is no concern on this issue while OTS data sampling is always less than model reconstruction time, 30 and this is one of main beneficial point of ANFIS model that makes it promising for tumor tracking clinically.
We were also interested in the NID and shooting time of stereoscopic system for taking data point at each update step. To do the first part, we investigated the role of stereoscopic X-ray imaging system on treatment quality enhancement by implementing different NIDs. Based on analyzed results from Figure 4 and Table 4, NID is highly effective on the accuracy of tumor motion tracking while breathing motion is not normal. In this condition, a large NID can remarkably increase prediction model accuracy. In contrast, for patients with RMSE less than 0.5 mm, known as control cases with normal respiration (patient 1, 3, and 7), the fluctuation of 3D RMSE versus NID variations is negligible.
We then proposed an adaptive supervision on the operation of stereoscopic X-ray imaging to intelligently manage its shooting time based on breathing status. By this idea, taking X-ray images will be intelligently increased while breathing phenomena are getting out of normal condition. Therefore, the time interval between consecutive X-ray imaging points is not necessarily constant. To do this, external markers that are continuously monitored by OTS can represent normal or abnormal status of patient breathing. Using this technique, patients are saved against additional imaging dose while unnecessary imaging data points are not taken and tumor tracking can be done with reasonable accuracy (Table 4). Therefore, the proposed strategy will make a trade-off between the performance accuracy of correlation model and the additional imaging dose. In order to assess the proposed supervision technique, a fraction of imaging data points was considered (1) while breathing is out of control for erratic cases and (2) while breathing is normal. Final analyzed results represent that X-ray shooting time is very important during tumor motion tracking. The average of 3D RMSE over 8 given patients is increased from 2.46 to 3.21 mm in the absence of sensitive imaging data points that is significant, whereas this value ranges from 1.87 to 1.97 mm in the absence of insensitive imaging data points that is not a remarkable increment (Tables 5 and 6). Therefore, each imaging data points taken by stereoscopic X ray system has its unique importance degree that must be taken into account during tumor tracking at external surrogate-based radiotherapy.
Conclusion
In this work, a study was performed on the management of stereoscopic of X-ray imaging system as responsible for detecting tumor position information as requirement for motion tracking at EBRT. We analyzed the role of imaging data points on model construction at pretreatment step, model performance testing, and also model reconstruction at each updating step during treatment using a group of real patients treated with CyberKnife Synchrony system. Imaging dose of this system received by patient was another challenge in our work that we realized a compromise between the maximum accuracy of correlation model and minimum imaging dose received by patient at the same time. Moreover, as the main achievement of this work we found that the performance of X-ray imager can be implemented intelligently based on breathing motion variations. The results reported in this work proved that for an erratic patient with high variability of breathing motion, the time and the NID taken by stereoscopic X-ray system can remarkably affect on tumor tracking accuracy and therefore treatment quality enhancement. Future studies will investigate data mining processes on taken data set to improve correlation model accuracy for tumor motion tracking.
Footnotes
Abbreviations
Acknowledgments
The authors acknowledge Sonja Dieterich for providing access to the clinical database.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.