
Abstract
Nonthermal irreversible electroporation is a new tissue ablation technique that consists of applying pulsed electric fields across cells to induce cell death by creating permanent defects in the cell membrane. Nonthermal irreversible electroporation is of interest because it allows treatment near sensitive tissue structures such as blood vessels and nerves. Two recent articles report that electrolytic reaction products at electrodes can be combined with electroporation pulses to augment and optimize tissue ablation. Those articles triggered a concern that the results of earlier studies on nonthermal irreversible electroporation may have been tainted by unaccounted for electrolytic effects. The goal of this study was to reexamine previous studies on nonthermal irreversible electroporation in the context of these articles. The study shows that the results from some of the earlier studies on nonthermal irreversible electroporation were affected by unaccounted for electrolysis, in particular the research with cells in cuvettes. It also shows that tissue ablation ascribed in the past to irreversible electroporation is actually caused by at least 3 different cytotoxic effects: irreversible electroporation without electrolysis, irreversible electroporation combined with electrolysis, and reversible electroporation combined with electrolysis. These different mechanisms may affect cell and tissue ablation in different ways, and the effects may depend on various clinical parameters such as the polarity of the electrodes, the charge delivered (voltage, number, and length of pulses), and the distance of the target tissue from the electrodes. Current clinical protocols employ ever-increasing numbers of electroporation pulses to values that are now an order of magnitude larger than those used in our first fundamental nonthermal irreversible electroporation studies in tissues. The different mechanisms of cell death, and the effect of the clinical parameters on the mechanisms may explain discrepancies between results of different clinical studies and should be taken into consideration in the design of optimal electroporation ablation protocols.
Keywords
Introduction
Permeabilization of the cell membrane through the application of very brief, high-strength electric field pulses characterizes the bioelectric phenomenon of electroporation. 1 –3 Electroporation can be of 2 types: reversible electroporation (RE), when the permeabilized (porated) cell membrane lipid bilayer reseals after the electric fields are removed, and irreversible electroporation (IRE), when the cell membrane does not reseal after the electric field is removed. 4 Cells survive RE and succumb to IRE. Interest in IRE has increased with the recent successful use of the technology for minimally invasive tissue ablation. 5 –7 Quantifying the effect of electric fields on cell survival is important for the design of optimal tissue ablation protocols with IRE.
Electric currents, passing through a biological medium, produce various effects simultaneously. These include electroporation and Joule heating. Nonthermal IRE (NTIRE) attempts to modulate the electroporation pulses in a way that selectively causes cell death by IRE while avoiding substantial thermal damage. 5,7 Nonthermal tissue ablation with NTIRE spares the tissue’s extracellular matrix and facilitates, thereby, treatment near sensitive structures such as large blood vessels, the pancreas, or the rectum. However, electric currents flowing through biological matter produce, in addition to electroporation and Joule heating, a number of other effects. These include electrolysis, ionthoporesis, and electro-osmotic flows. The phenomena of electroporation 8 –15 and the phenomena of electrolysis 16 –25 were both used in the past for tissue ablation, each separately. However, in 2 recent articles, we show that various optimized combinations of electrolysis with electroporation can increase the extent and control of tissue ablation over protocols designed for each modality separately. Specifically, Phillips et al 26 show that the electrolytic products generated during electroporation can extend the electroporation tissue ablation into the reversible electroporated region of tissue. In the study of Phillips et al, we show that RE can augment tissue ablation by electrolysis. Obviously, combining electroporation and electrolysis sagaciously can be used to augment and optimize tissue ablation. However, reviewing the findings in those articles triggered concern that the results of earlier studies on NTIRE may have been inadvertently tainted by unaccounted for electrolytic effects. More critical—are there circumstances in which there is tissue ablation by IRE alone without electrolytic effects?
The study reported here is a reexamination of some of the earlier research on tissue ablation with IRE, in the context of our recent findings, on the combination electroporation and electrolysis. 23,24 To this end, we have examined the occurrence of electrolysis in some of our earlier studies on NTIRE. We find that, indeed, some of the earlier NTIRE experiments were affected by electrolysis, in particular the research with cells in cuvettes. However, we also found that there are substantial domains of irreversible electroporated ablated tissue in which there is no effect of electrolysis.
Materials and Methods
The goal of this study is to evaluate the occurrence and possible effects of electrolysis in previously reported studies in which cell damage was attributed to NTIRE. To this end, we have revisited NTIRE studies performed with: (a) cells in conventional electroporation cuvettes 28,29 and (b) the first in vivo studies on NTIRE. 8,9 Two experimental setups were employed. To examine the electrolysis during cell electroporation in cuvettes, we have used a standard electroporation system, ECM 830 electroporator (BTX, San Diego, California), with a typical 2 mm electroporation cuvette. The experiment and the experimental systems were a duplicate of the earlier NTIRE studies. 28,29 Specifically, we filled the same size cuvettes used in the previous studies with the same solution, albeit without cells, and applied the electroporation protocols used in Miller et al and Rubinsky et al. 28,29 However, in this work, we measured the changes in pH in the cuvette, immediately after the delivery of the electroporation pulse sequences using an Oakton Instruments (PH 450) meter (Vermonth Hills, Illinois) with a microcombination pH probe MI-414B (16 gauge, tip 6 cm length; Bedford, New Hampshire) pH probe.
For the second set of experiments, we employed a physiological saline-based agar gel phantom to simulate the in vivo experiments in Rubinsky et al and Onik et al studies. 8,9 To construct the phantom, 0.5% Bacto-Agar (Fisher Scientific International Inc. [Hampton, New Hampshire]) was mixed with 9 g/L NaCl (Fisher Scientific) in distilled water. The solution was then brought to boiling and poured into Petri dishes. A pH colorimetric indicator (RC Hagen A7815 pH Wide Range; Hagen, Canada) was mixed into the gel prior to solidification. Two stainless steel needle electrodes (NanoKnife,AngioDynamic, New York) were inserted into the solid agar gel, perpendicular to the outer surface, to a depth of 1 cm and at a distance between them prescribed by the in vivo protocol we emulate. The experimental setup is shown in Figure 1. The NTIRE electric pulse sequences employed in Rubinsky et al and Onik et al 8,9 studies were applied to the electrodes, and the colorimetric changes in pH were recorded with a Cannon EOS Rebel T6i DSLR camera (Cannon, Japan). The white balance of the images were adjusted to fit the agar gel color to enhance the visibility of the margin of the pH changes affected region near the electrodes. The range of the pH-stained area around the anode was from saturation, pH 1, near the electrode, to approximately pH 6 on the outer edge of the stained area (Figures 2C, 3B, and 4B). The range of the stained area around the cathode was from saturation, pH 12, near the electrodes, to approximately pH 8 on the outer edge of the stained area (Figures 2C, 3B, and 4B). The outer edge of the anode stain represents an acid pH of approximately 6, and the outer edge of the cathode stain represents a basic pH of approximately 8. We have used the color matching card provided by the manufacturer to determine the approximate pH range. Electrolysis-related tissue ablation studies have shown that electrolysis-induced tissue ablation correlates well with changes in pH. 19

Experimental setup.

Re-examination of results with pig liver tissue ablation with a 4-electrode configuration in Rubinsky et al. 8 Comparison between (A) the isoelectric field lines [V/cm] in a 4-electrode tissue ablation experiment (figure 1B in Rubinsky et al 8 ), (B) the ablated tissue histology (figure 3A in Rubinsky et al, 8 and (C) the results from a pH dye stained gel experiment using 4 electrodes in the same configuration and with the same protocol as that in Rubinsky et al. 8 The stained area experienced changes in pH. The location of the electrodes is marked by blue crosshairs.

Comparison between (A) the isoelectric field (V/cm) lines in a 2-electrode tissue ablation experiment (figure 1A in Rubinsky et al 8 ) and (B) the results from a pH dye stained gel experiment using 4 electrodes in the same configuration and with the same protocol as that in Rubinsky et al. 8 The stained area experienced changes in pH. The location of the electrodes is marked by blue crosshairs.
Results
Table 1 was obtained in a study with the experimental parameters of Rubinsky et al. 29 A 2-mm cuvette was used, and the solution was pH-buffered saline with an initial pH of 7.5. The highlighted columns 3, 4, 5, and 6 from left are the new data. They are, respectively, time of exposure to electric field, charge delivered in units normalized to the first row, total time the cells in the reference study 29 have resided in the cuvettes (this is also the time when the pH measurements were taken in this study), and the measured pH at the end of the experiment. The time of exposure to the electric field is an experiment parameter. The charge in Coulombs was calculated from the fundamental definition of charge, which is current in Amperes multiplied by time in seconds. We assumed that the electrical resistance of the saline in the cuvette is the same in all the experiments. From this assumption, the normalized charge ratio between the experiments in the first row and the rest of the experiments scales as the ratio of the product—voltage, in Volts, multiplied by time of exposure to that voltage in seconds—for the different experiments. The total time the cells in Rubinsky et al study 29 resided in the cuvette is evaluated from the time length of the experiments listed in Rubinsky et al. 29 It should be emphasized that in the original study, the cells were removed from the cuvette, immediately after the end of the electroporation protocol delivery, and inserted in a buffered pH solution. Removing the cells from the cuvette and inserting them in the pH-buffered solution has taken several seconds. Therefore, the uncertainty in the time of exposure of the cells to electrolytic products, listed in column 5 from left, could be several seconds. This uncertainty could introduce a significant error in the evaluation of time of exposure to the products of electrolysis in experiments with electric fields of 2000, 1500, and 1000 V/cm, and the first 3 rows are given in Table 1. The pH data are the measured average pH from 3 repeats and the standard deviation. The pH was measured at the end of the electroporation field delivery protocol and represents the pH that would have existed when the cells in Rubinsky et al study 29 were removed from the cuvettes for viability processing. The table shows that the pH has changed in all the experiments and has become basic. The most relevant observation to this study is that in the experiment with an electric field of 125 V/cm, the charge delivered was 24 times larger than in the experiment with an electric field of 2000 V/cm, and the exposure to the higher pH was more than 2 orders of magnitude longer.
Electrolytic Effects in the Results of an Electroporation Study With PC3 (Prostate Adenocarcinoma) Cells Reported in Rubinsky et al.29,a

aThe highlighted columns are the electrolysis relevant data.
Table 2 was obtained in a study with the experimental parameters of Miller et al. 28 A 2-mm cuvette was used, and the solution was pH-buffered saline with an initial pH of 7.5. The highlighted columns 3, 6, and 8 from left are the new data. They are, respectively, charge delivered in units normalized to the first row of Table 2, total time the cells in the examined study have resided in the cuvettes, 28 and the pH at the end of our experiment. The charge in Coulombs was calculated as described previously. The time of exposure to the electric field is an experiment parameter. The total time the cells in Miller et al study 28 resided in the cuvette is evaluated from the time length of the experiments listed in that reference. In the original study, the cells were removed from the cuvette, immediately after the end of the electroporation protocol delivery and inserted in a buffered pH solution. Removing the cells from the cuvette and inserting them in the pH-buffered solution has taken several seconds. In this experiment, this uncertainty introduces a negligible error in evaluation of time of exposure to the products of electrolysis. The pH data are the average measured pH from 3 repeats and the standard deviation. The pH was measured at the end of the electroporation field delivery protocol and represents the pH that would have existed when the cells were removed from the cuvettes for viability processing in Miller et al. 28 The table shows that the pH has changed in all the experiments and has become basic. The most relevant observation to this study is that in the last series of experiments, the difference in time of exposure to products of electrolysis during electroporation with 1500 V/cm is significant and ranges from 0.9 to 242 seconds. The time of exposure and the charge also seem to correlate with viability.
Electrolytic Effects in the Results of an Electroporation Study With HepG2 (Primary Human Hepatocarcinoma) Cells Reported in Miller et al.28,a

aThe highlighted columns are the electrolysis relevant data. The calculated charge is normalized with respect to Table 1.
Tables 1 and 2 show a substantial change in pH in every cuvette experiment. The results of the analysis for Tables 1 and 2 raised the concern that every IRE tissue ablation is contaminated by electrolytic products effects and that, in fact, there is no cell death from IRE alone. Therefore, we developed an experiment that could tell us if in our earlier studies on tissue ablation with NTIRE, there were regions in which the cell death could be attributed to IRE, only. Using the method described earlier for simulation of pH front propagation in tissue, we repeated the experiments in Rubinsky et al and Onik et al. 8,9
Figure 2 shows an evaluation of the possible extent of the pH fronts affected region during the tissue ablation study in figures 3 and 6 of Rubinsky et al. 8 The experimental configuration employs the pH dye-stained gel described earlier and consists of 4 stainless steel needles (NanoKnife, AngioDynamics, New York; gage 16), each one inserted into the gel at 1 apex of a 1.5 cm × 1.5 cm2 (Figure 1). Similar to the study reported in Rubinsky et al, 8 we applied 2500 V across each 2, adjacent on the side of the square, stainless steel needles. The pulses were of 100 microseconds duration separated by 100 milliseconds. Eight pulses were applied sequentially between each adjacent pair in a clockwise direction, similar to the experimental procedure in Rubinsky et al. 8 Consequently, each electrode served alternately, for 1 sequence as a cathode and for the second sequence as an anode. Figure 2 consists of 3 panels. Panel 2A shows the calculated isoelectric field contours. The figure was obtained from the solution of the Laplace equation and shows a superposition of the maximal fields at each location in the treated region. 8 This panel is a cleaned up version of figure 1B of Rubinsky et al. 8 Panel 2B is figure 3A from Rubinsky et al. 8 It shows the NTIRE ablated tissue between the electrodes. The important observation is that the entire tissue between the electrodes is ablated. However, it is interesting to notice, in the context of this study, that the macroscopic appearance of the ablated tissue near the electrodes is different from that in the center of the 4 needles lesion. Panel 2C is the result of our experiment. The stained regions around the electrodes are caused by the electrolysis-induced pH changes. Several interesting observations emerge. First, the pH changes in panel 2C are restricted to the vicinity of the electroporation needles, while the ablation in panel 2B occurs throughout the entire region braced by the electrodes, to the center of that region. Second, it seems that the region with a different macroscopic appearance of the ablated tissue near the electrodes in panel 2B has similar dimensions to those of the pH change marked dye area in panel 2C.
Figure 3 shows results from a gel study with 2 electrodes separated by 1.5 cm. The electroporation protocol consists of the delivery of eight 2500 V, 100-microsecond long 2500 V pulses at a frequency of 10 Hz. This experiment emulates the experiment in figure 1 panel A of Rubinsky et al. 8 In typical tissue ablation, it occurs for electric fields higher than about 500 V/cm (panel A of Figure 3). 8 The colorimetric indicator in the gel model, panel B, Figure 3, shows that the electrolysis products are found only near the electrodes. The center of the region braced by the electrodes is not contaminated by the electrolytic products.
Figure 4 shows the extent of the pH front affected region during the tissue ablation study in the prostate shown in figure 1 of Phillips et al. 27 We applied 1000 V across 2 stainless steel needles (NanoKnife, AngioDynamics, New York; gage 16) separated by 1.0 cm. Eight, 100-microsecond long pulses were applied at a frequency of 10 Hz. Panel A in Figure 4 (taken from figure 1 of Onik et al 9 ) shows that the tissue ablation in the prostate spans the region between the 2 electrodes. It is evident from the panel B, in Figure 4, showing the extent of electrolysis that, while the actual ablation occurred to the center of the region spanned by the 2 electrodes, the electrolytic front is restricted to the vicinity of the electroporation needles.

Comparison between (A) extent of tissue death (from figure 1 in Onik et al 9 ) and (B) results of electrolysis experiments in a gel model with a pH colorimetric indicator. The stained area experienced changes in pH. The electroporation parameters were eight 100-microsecond long pulses of 1000 V, delivered at 10 Hz. The location of the electrodes is marked by blue crosshairs.
Discussion
The data in Tables 1 and 2 show a substantial change in pH at the end of each electroporation experiment and indicate that in all our cuvette experiments, there was substantial electrolysis. The effect of products of electrolysis on cell death was studied in the past. The earlier landmark pulsed electric field studies of Sale and Hamilton report that, after performing a thorough study of possible electrolytic cell damage during electroporation, they found none. 30 –32 However, Saulis warned of the detrimental effect of changes in pH in electroporation studies in cuvettes, already in 1999. 33 It now appears that at least in studies on cells in conventional cuvettes, the findings of Saulis are correct. It is well established that the process of electrolysis, which occurs at the electrode surfaces around electrodes submerged in an ionic conducting media, can cause cell death. This fact was known and used in tissue ablation since the early 19th century. 34 The mechanism of cell death by electrolysis is chemical. New chemical species are generated at the interface of the electrodes as a result of the electric potential-driven transfer between electrons and ions or atoms. In physiological saline solutions, these chemical reactions yield changes in pH. Electrolysis can cause cell death by 2 factors: a cytotoxic environment developing due to local changes in pH as well as the presence of some of the new chemical species formed during electrolysis. Because the mechanism of cell death by electrolysis involves a chemical reaction, the lethal effects of the products of electrolysis are a function of (a) concentration of the products and (b) the time of exposure to those products. One important product of electrolysis that can cause cell death is Cl2(gas) at the anode. It is likely that the cause for a basic pH in our cuvette experiments is the Cl2(gas) leaving the solution in the form of a gas.
In our studies in Miller et al and Rubinsky et al, 28,29 we removed the solution with the cells from the cuvette immediately after the delivery of the pulses and mixed the solution with a buffered solution with viability dyes. Therefore, the products of electrolysis were diluted immediately after the application of the pulses. Considering that the removal of the cells from the cuvettes may have taken several seconds, this is the accuracy with which we can estimate the time of exposure to the electrolytic products in column 5 of Tables 1 and 2. The primary goal of the study reported in Rubinsky et al 29 was to establish “electroporation” parameters that cause cell death to facilitate in the design of optimal NTIRE protocols. The cell viability results in Table 1 (column 9) 29 were obtained by increasing the number of pulses for each electric field studied until maximal cell death was observed. The other constrain in those experiments was to not exceed the thermal ablation limit. It is evident that the lower the electric field, the larger the number of pulses required for complete cell ablation. We were actually surprised to find that the studies in Rubinsky et al 29 show complete cell death for electric fields of 500, 250, and even 125 V/cm. Electroporation with these electric fields is usually considered reversible. 33,35 Originally, we attributed the cell death to the number of pulses and some kind of unknown IRE, pulse number dependent phenomena. 29 However, the new experiments in Table 1 show that in all the cuvette experiments, there was a substantial change in pH. The toxic effect of electrolysis-induced changes in pH on cells is well established, 19,33 and this effect may have occurred in all the experiments. Cell death by electrolysis is a direct function of the charge delivered and the time of exposure to electrolytic products. 23 –25 In our earlier study, 29 cell death in cells electroporated by reversible electroporated-type pulses occurs when the charge delivered is larger by well over 2 orders of magnitude from the charge delivered during what are considered typical irreversible ablation electroporation pulses, 35 and the time of exposure to the toxic environment is as much as 24 times longer. Therefore, it is more likely that the cell death with RE kind pulses reported in Rubinsky et al 29 is due to the toxic effect of the electrolytic products generated in the cuvettes rather than some type of IRE phenomena. A thorough review of the various studies on IRE parameters was recently published in Chunlan et al. 6 That review points out that the conclusions of our study in Rubinsky et al, 29 concerning the range of electroporation parameters that cause IRE, are inconsistent with those of other studies, such as Miklavcic et al. 35 This reexamination of the study in Rubinsky et al 29 shows that indeed the cell death observed in cuvette studies in cells treated with RE-type parameters was most likely caused by a chemical electrolytic type cell damage rather than some unknown kind of IRE effect. Cell death from multiple pulses in the RE range of parameters is caused, most likely, from an electrolytic effect. This can have value in enhancing cell death from electroporation 26,27 but is not cell death from IRE alone.
The results from experiments relevant to Miller et al 28 are displayed in Table 2. Here we also observe an increase in pH in all the experiments. The results shown in the first 5 rows of Table 2, in which we applied a single pulse, depict mostly similar cell survival for all the electric fields used. Because of the protocol, the time of exposure to the products of electrolysis was short (seconds) and therefore the cell death could be attributed to IRE. Comparing the last 3 experiments with the first 5 adds additional insight into the mechanism of cell death by electroporation and by electrolysis. Comparing the delivery of 1500 V/cm electric fields as 1 pulse and as 10 pulses (row 6) shows that the percentage of cell survival is not affected by the number of pulses, when the exposure to products of electrolysis is sufficiently short. The last 3 rows indicate that for an electric field of 1500 V/cm, the substantial reduction in viability is associated with a longer exposure to the higher pH solution (in addition to a larger number of pulses). Obviously, much more research needs to be done to verify this conclusion. However, it tentatively appears that the percentage of cell death is strongly related to time of exposure to electrolytic products during electroporation, even when typical IRE pulses are delivered. It is well established that IRE cell death exhibits a statistical distribution, that is, not all cells die during the application of a certain IRE pulse. 36 It is possible that the effect of electrolysis products is to cause the death of those cells that would statistically survive electroporation. A conclusion from the cell experiments is that the effects of electrolytic products cannot be ignored in designing NTIRE tissue ablation protocols. Furthermore, it appears that cuvette experiments are not a good model for designing NTIRE tissue ablation protocols. In general, all the NTIRE studies generated with cells in cuvettes should be reexamined for possible contamination with electrolysis effects.
An important attribute of NTIRE is that the mechanism of cell death involves only the permanent permeabilization of the cell membrane. This assumption is central to the electroporation treatment of sensitive tissue structures. The results from Tables 1 and 2 show that there are electrolytic effects in all the NTIRE experiments in cuvettes. This raises some important questions with regard to the clinical use of NTIRE. Does cell death from IRE alone exist? Does all cell death from electroporation involve electrolysis? Cuvette experiments cannot answer these questions in the context of clinical applications, because they are characterized by small dimensions. The products of electrolysis form near the electrodes and diffuse into the bulk of the solution. In small dimension cuvettes, the diffusion length is short. Tissue electroporation occurs at much larger length scales. We designed the experimental system in Figure 1 to answer the questions raised by the cuvette studies. The experiment mimics tissue NTIRE protocols using a tissue model based on a gel agar made of physiological saline. Gels made of saline are a good first order simulation of the electrical behavior of tissue 37 and are also used as a tissue model in research on the propagation of electrolytic products. 38 The physiological saline gel has a higher conductivity than most tissue and a greater ionic diffusivity. Typical values for normal saline gel electric conductivity is 300 mS/m, while the mean conductivity for all prostate type tissue at 100 Hz is 83 mS/m and 39 conductivity of liver tissue is 126 mS/m at 10 Hz. 40 Ionic diffusivity is proportional to electrical conductivity. 41,42 Gels also lacks the diluting effect of blood flow. Therefore, the quantity and the propagation in time of the products of electrolysis in a gel model could serve as an upper limit for the propagation and quantity of the products of electrolysis in tissue.
Figures 2, 3, and 4 are for experimental conditions in tissue, in which the tissue was completely ablated in the domain bounded by the electrodes. 8,9 While electrolysis occurred in all the experiments in Figures 2, 3, and 4, the products of electrolysis did not span the entire treated volume. The tissue experiments show complete ablation between the electrodes, while the extent of electrolytic products propagation is contained near the electrodes. Therefore, it is possible to tentatively conclude from this study that tissue ablation by IRE alone exists. Obviously this is not the only evidence that IRE as a mechanism of tissue ablation exists. This was also shown in other studies. 35 However, we were concerned that all our NTIRE experiments in tissue were completely contaminated by electrolytic products toxicity, like in the cuvette experiment. This study suggests that the results in Rubinsky et al and Onik et al 8,9 were only partially affected by electrolysis, near the electrodes.
All the studies reexamined in this article were performed for nonthermal ablation conditions. Therefore, in this study, the electrolytic processes of cell death occurred in a domain of electric parameters that cannot induce thermal damage. We applied electroporation pulses that are considered to belong to the domain of RE and IRE and noted cell death in the presence of electrolysis. The results suggest that the domain of tissue ablation by electroporation is made of IRE without electrolysis, IRE with electrolysis, and RE with electrolysis. The different mechanisms of cell death may affect cell and tissue ablation in different ways, and the effects may depend on various clinical parameters such as the polarity of the electrodes, the charge delivered (voltage, number, and length of pulses), and the distance of the target tissue from the electrodes. Each of these different mechanisms may have different applications for tissue ablation. Figure 5 is an attempt to summarize this understanding using a possible qualitative display of the different domains in which electrolysis and electroporation induce tissue ablation in a superposition effect, as a function of electric fields and delivery time. This figure is also relevant to the study in Phillips et al 26,27 and defines the domains in which the combination of electroporation products of electrolysis can be used for tissue ablation.
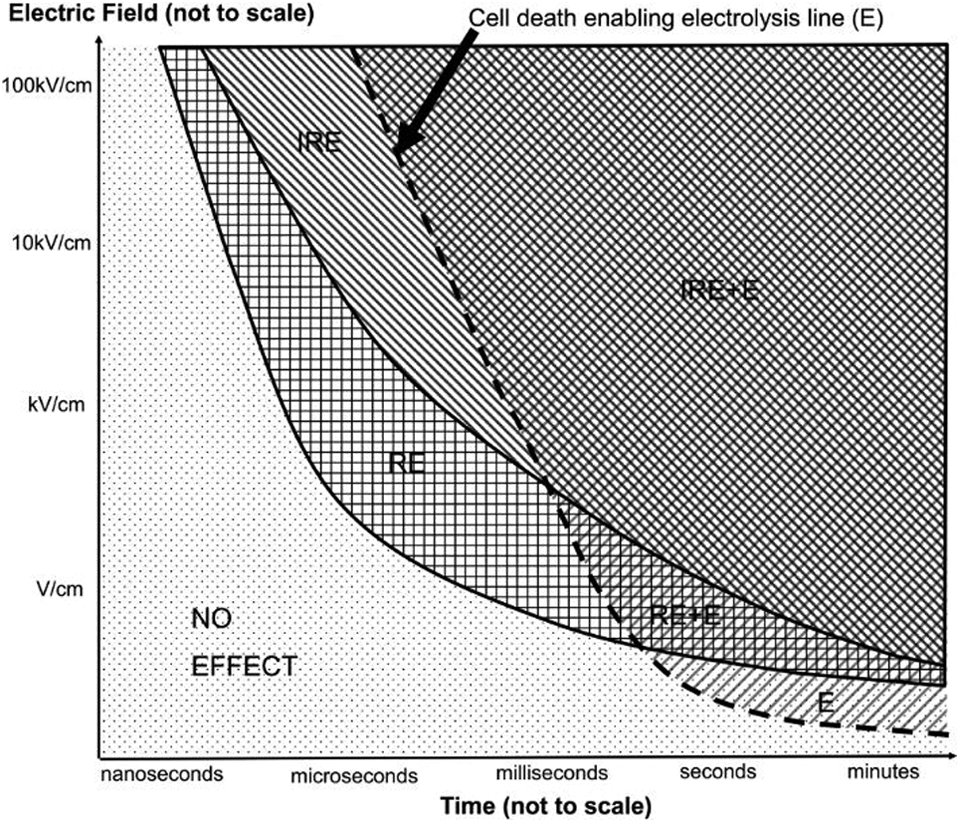
Schematic graph of tissue ablation domains as a function of electric field and time of exposure. E indicates electrolysis ablation; RE + E, combination reversible electroporation and electrolysis ablation; IRE + E, combination irreversible electroporation and electrolysis.
The study in this article and in Phillips et al 26,27 leads to new insight with regard to the design of optimal electroporation-based tissue ablation protocols. It is evident that electrolysis occurs in all electroporation protocols and must be considered. For completeness, we should add that our previous studies show that the electrolytic products at the anode are different from those at the cathode, and they yield different mechanisms of electrolytic damage. 26,27 The process of electrolysis causes, in addition to ion migration, electromigration of water and dehydration near the anode. The different mechanisms identified in this study and in our earlier studies 26,27 may affect cell and tissue ablation in different ways and the effects may depend on various clinical parameters such as the polarity of the electrodes, the charge delivered (voltage, number, and length of pulses), and the distance of the target tissue from the electrodes. All this suggests that the use of electroporation for tissue ablation is not trivial and should be used judiciously, with emphasis on a good understanding of the mechanisms involved.
Conclusion and Clinical Implications
We report the results of a study that examines the possible occurrence of electrolysis during electroporation protocols used for tissue ablation. The results show that in many protocols the changes in pH by the electroporation pulses is large and may have been the cause of cell death originally attributed to IRE. Earlier studies on NTIRE using cells may have reached wrong conclusions, and caution is recommended in using those conclusions for designing NTIRE tissue ablation protocols. However, the analysis of earlier NTIRE studies in tissue shows that there are substantial domains in which tissue is ablated by IRE alone without electrolysis and without thermal effects. A qualitative diagram that illustrates tissue ablation by electroporation with and without products of electrolysis was produced.
Current clinical protocols employ ever-increasing numbers of electroporation pulses to values that are now an order of magnitude larger than those used in our first fundamental NTIRE studies in tissues. 8,9 The different mechanisms of cell death and the effect of the clinical parameters on the mechanisms may explain discrepancies between results of different clinical studies and should be taken into consideration in the design of optimal electroporation ablation protocols. For instance, in our earlier article that reported nerve survival after NTIRE treatment in an animal model, we used only 8 pulses. 9 In contrast, the current trend in NTIRE is to use increasingly larger numbers of electric pulses, and there are many circumstances in which over 300 pulses are delivered on 1 electrode.
So far clinicians and scientists have difficulties understanding the effects of IRE on tissue. Electrolytic effects appear to be an integral part of electrotherapies. This adds a new parameter in the mechanisms of cell ablation by electroporation. It is conceivable that different electric “pulse sequences,” resulting in different degrees of reversible and IRE and electrolysis, might have advantages and disadvantages in specific tissues and organs, depending on the specific structure of the tissue and the sensitivity of the anatomical structures to be spared. More research is necessary to understand the implications for optimal tissue ablation protocols.
Footnotes
Authors’ Note
Liel Rubinsky, and Enric Guenther have contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors are employees of InterScience, Luzern, Switzerland - a company in the field of tissue treatment by electroporation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.