
Abstract
Laparoscopic cholecystectomy is widely considered as the treatment of choice for acute cholecystitis. The safety of the procedure and its minimal invasiveness made it a valid treatment option for a patient not responding to antibiotic therapy. Our research shows that patients positively assess this treatment method, but the world’s tendency is to turn to a more sophisticated method utilizing robot-assisted surgery as a gold standard. Providing patient with minimally invasive surgical procedures that utilize the state-of-the-art equipment like the da Vinci Robotic Surgical System underscores the commitment to high-quality patient care while enhancing patient safety. The advantages include minimal invasive scarring, less pain and bleeding, faster recovery time, and shorter hospital stay. The move toward less invasive and less morbid procedures and a need to re-create the true open surgical experience have paved the way for the development and application of robotic and computer-assisted systems in surgery in Poland as well as the rest of the world.
Introduction
The use of technological advancements in the field of medicine is an evolving phenomenon. The year 1988 saw the introduction of laparoscopic surgery that utilizes camera to perform the operation. The first computer-assisted surgery was performed in 1996. Computer-assisted surgery enables an interface between the surgeon and the patient being operated. This interface then reviews the surgeon’s actions in order to repeat the actions, guarantee the patient’s safety, and then transmit these actions to a remote device that actually performs the surgical operation.
Dr Marescaux used Computer Motion’s ZEUS Robotic Surgical System (Computer Motion Inc), a voice-activated robotic system composed of 3 robotic arms operated by the surgeon from a remote console. Two of the arms hold the requisite surgical instruments and are manipulated by a joystick on the surgeon’s remote console; the third arm operates the camera and is voice controlled. 1 A high-speed fiber-optic service links the surgeon to the robotic system, which is located just a few feet away from the operating table. 1 The world’s first successful attempt of cyber surgery took place on September 7, 2001, when Dr Jacques Marescaux utilized a computer in New York City to manipulate a robot in Strasbourg, France, to remove the patient’s gallbladder during Operation Lindbergh. 1 Dr Marescaux was not in a hospital; he was located in an ordinary building. Meanwhile, his patient and the robot were in a hospital in Strasbourg accompanied by 2 other doctors prepared to intervene if necessary. 1
The setup of Operation Lindbergh was as follows: the surgeon in New York worked at the robot control station, with a computer transmitting his commands. Using a headset, he talked to the team in France while viewing the patient on a video screen in New York. All the equipments (including computers, videoconferencing equipment, and audio equipment in both New York and France as well as the robot, the camera, and the robot command station) were connected so that the robot responded to the surgeon’s commands in real time, with no significant delay in the transmission of sounds or images. 2
In addition to the ZEUS machine used in Operation Lindbergh, the other popular remote robotic surgery system was the da Vinci system (from Intuitive Surgical, Sunnyvale, California). 2,3 With the da Vinci system, the surgeon sits at a remote console and controls the robotic arms that function like a surgeon’s hands in real time. The robotic “hands” are actually capable of some movements and maneuvers that would be difficult, if not impossible, for a human wrist and hand to accomplish and also operate with maximum precision during the surgical procedure. 3
The da Vinci system responds to manual commands, but robotic arms of ZEUS are able to respond to both manual and voice commands. 3 Moreover, to move the robotic hands efficiently, the da Vinci system utilizes InSite Vision (Intuitive Surgical), a network of fiber-optic cables, which provides stereoscopic vision. 2 –5 This 3-dimensional stereoscopic vision further distinguishes da Vinci from ZEUS, which only provides the surgeon with 2-dimensional images. 1,3,5 –7
Regardless of the distinct capabilities of both sets of the surgical robotic equipment, da Vinci and ZEUS have a lot in common besides their higher price. 1 –3 For example, each instrument consists of 2 robotic arms that are adept at fine motor work. 3
Both ZEUS and da Vinci have robotic arms linked to a control panel via a fiber-optic cable. 1,3,7 It is from the surgeon’s control panel that the surgeon is able to control the robotic instrument during a telesurgical operation. 4 –6 Therefore, unlike a traditional surgery where the operating doctor is physically required to be next to the patient with traditional handheld surgical equipment, in the robotic surgery the surgeon does not have to be anywhere near the patient. 2,3,7 This is highlighted in Operation Lindbergh. 1 As discussed earlier, the possible distance that can exist between the surgeon and the patient is limited by the inherent delay in the fiber-optic transmission, which continues to be refined. 4 –7
All these computer-based systems used in the operating theater and the electronic equipments and instruments are referred to as medical robotics and computer-assisted surgery (MRCAS) or more dramatically “the operating room of the future.” The MRCAS is used in a growing number of operating rooms around the world, largely as a result of the growing popularity of minimally invasive surgical (MIS) techniques. The MIS or a “keyhole” surgery is an alternative to the traditional open-incision surgery in a growing number of procedures. The MIS procedure also utilizes special instruments that can be inserted and manipulated through small incisions (sometimes no more than a few millimeters long) under remote optical or video guidance, greatly reducing patient trauma and recovery times and providing psychological comfort to patients. Patient’s safety is guaranteed not only during surgery but also during hospital stay.
The need to perform delicate surgical procedures safely in tight spaces where the surgeon cannot directly see what she or he is doing has created a growing market for devices that act as extensions of the surgeon’s eyes and hands: remote imaging, data processing and feedback, and robotics. Meanwhile, the MRCAS technology has been evolving as have been the medical and economic environments in which it is used. In the aging populations around the world, there is an increasing demand for a wide range of age-related surgical procedures such as heart, spine, general, and orthopedic surgeries. Technological advances have expanded the range of surgical procedures that can be performed using MIS techniques, making them accessible and safe to more people.
Materials and Methods
This research was conducted in public surgery clinics in Poland. The research described here was conducted in 6 health care units of Kujavian–Pomeranian province. These units were divided into 2 groups: group I—3 hospitals with the number of beds more than 400 and group II—3 hospitals with the number of beds less than 400. The research included 180 patients, that is, 30 from each hospital. We asked our patients how they assessed hospital equipment such as diagnostic machinery and other medical equipment. We also asked them how they assessed patient safety in the surgery ward during the minimal invasive procedure. Another question directed to the patients was whether the hospital in which they were staying was an institution worth of recommendation to a friend and whether the patient had a sense of safety during hospitalization.
We used Servqual method to test the patients’ satisfaction with regard to the safety, medical equipment used and their intention to recommend or return to the same hospital. This method tests the patients’ expectations regarding the service level in aspects of safety during minimal invasive surgery and patients’ safety during hospitalization.
Each patient underwent laparoscopic cholecystectomy. The average time of a patient’s stay at a hospital was 3 days. The research results were analyzed statistically. We used nonparametric statistical Spearman, Kruskal-Wallis, and Mann-Whitney U tests.
Results
The basic hypothesis—hypothesis zero in this study—was that there is no difference between the 2 groups (group I and group II) analyzed. In other words, all the patients treated in both the groups of hospitals expect the same aspects during their hospital stay, that is, safety during hospital care, new methods of treatment, use of modern equipment, and minimal invasive health care procedures. There is also no difference between the groups with regard to demographic data, especially sex and age, although there were differences with reference to the educational level of the respondents (ie, group I predominantly consisted of patients with university- and college-level education and group II consisted of patients with basic technical and high-school education). In spite of this, however, there were no statistically significant differences (P > .05). Demographic data of the patients are given in Table 1.
Patients’ Demographic Data.a
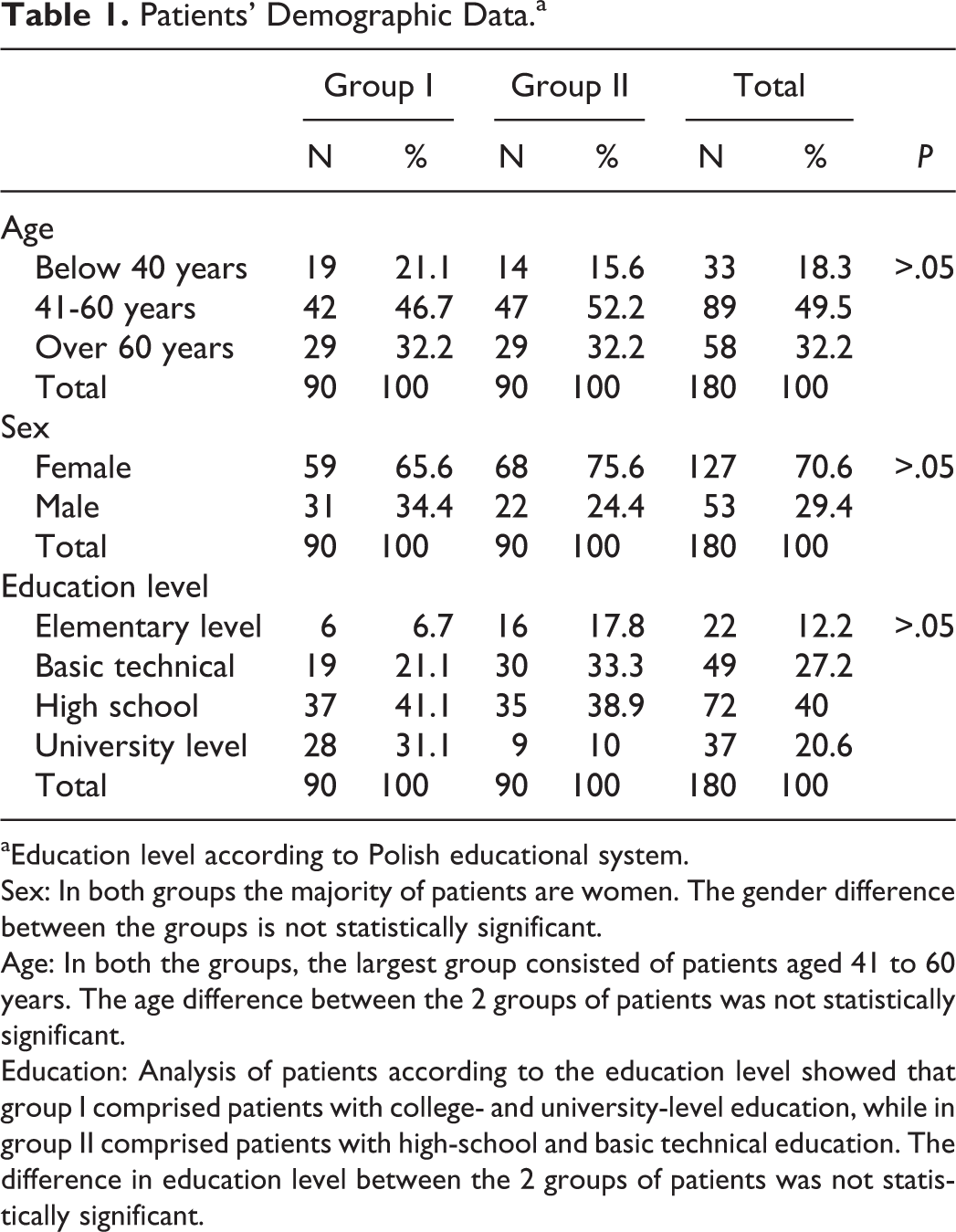
aEducation level according to Polish educational system.
Sex: In both groups the majority of patients are women. The gender difference between the groups is not statistically significant.
Age: In both the groups, the largest group consisted of patients aged 41 to 60 years. The age difference between the 2 groups of patients was not statistically significant.
Education: Analysis of patients according to the education level showed that group I comprised patients with college- and university-level education, while in group II comprised patients with high-school and basic technical education. The difference in education level between the 2 groups of patients was not statistically significant.
Figure 1 presents patients’ assessment of the medical equipment and treatment used during minimal invasive health care procedures. When we asked patients in both the groups about safety during hospital stay and how they assessed it in terms treatment using MIS, their response was similar to the one mentioned earlier. Patients in group I assessed safety a little higher than patients in group II. The differences, however, are small. The detailed assessment of patients is presented in Figure 2.

Distribution of average assessment of medical equipment in groups. Patients in both the groups assessed the medical equipment and treatment during minimal invasive health care procedures similarly.
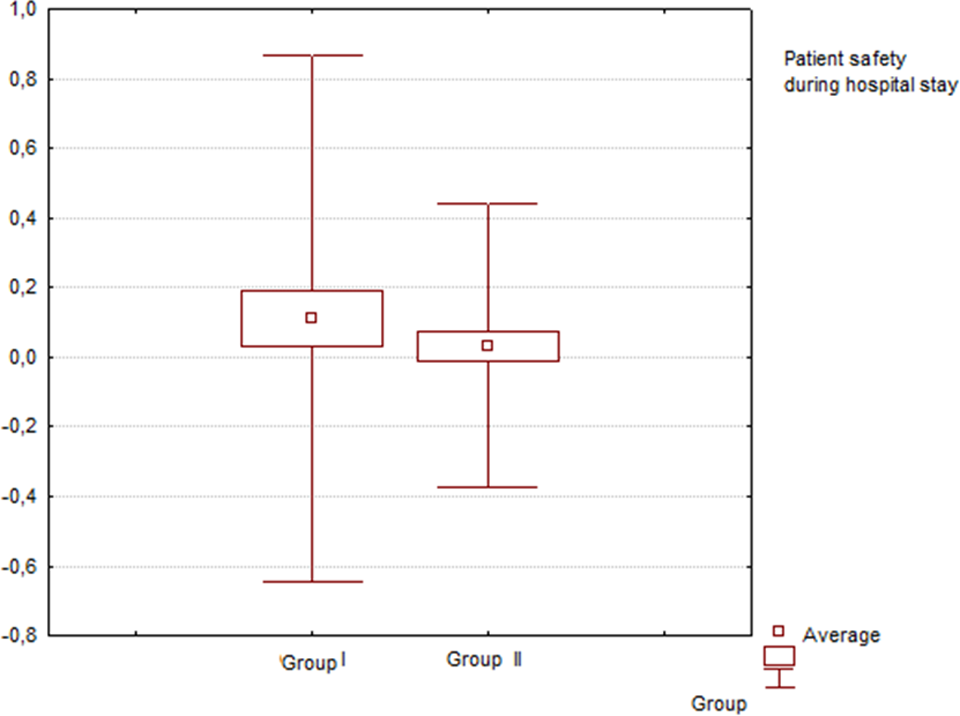
Safety and hospital equipment are important from patients’ point of view. These parameters were rated lower in group II and their safety was also rated lower. Mann-Whitney U test shows that there are no differences in the tested groups with regard to patient safety during hospital stay, although patients from group I assessed the safety in hospital as higher during minimally invasive surgery (difference in the order of .08).
It can be observed that patients appreciated the minimal invasive surgery and safety during such procedures, which is guaranteed by the technological progress. Advances in surgery have centered on minimizing the invasiveness of surgical procedures as a means to reduce patient morbidity and mortality. As a result, improvements in video imaging, endoscopic technology, and instrumentation have created MIS. In addition, working with traditional instrumentation compared to minimally invasive one often leads to muscle fatigue, exaggeration of hand tremor, and imprecision attributable to the length of the instrument shaft and the higher handle forces. The principal disadvantage of the conventional operation techniques is that freedom of movement is restricted. This restriction is attributable to 8 the confined operative field 9 and the instrument’s limited range of motion. 10
Using the advanced technology during surgery is also one of the arguments that influence patients’ willingness to recommend a hospital to the patients’ friends and family (Table 2).
Patient’s Willingness to Recommend a Hospital.a

aPatients from both the groups are willing to recommend a hospital—79.9% of all patients in group I and 80% of all patients in group II. The result is similar for both the groups. Minimally invasive surgery significantly influenced the patient’s willingness to recommend a hospital.
Patients from both the groups are willing to recommend a hospital—79.9% of all patients in group I and 80% of all patients in group II. The result is similar for both the groups, and we conclude that the quality of medical equipment and the safety of minimal invasive surgery significantly influenced the patient’s willingness to recommend a hospital.
Discussion and Conclusion
The results of this study indicate a few important points. In general, they point to the importance of the introduction of a new method of treatment in hospital practices and the need to introduce automated systems for operating theaters to improve surgeons’ comfort of work and patient’s safety. Patient’s safety during the treatment process in combination with high-tech equipment influences patient’s willingness to recommend hospital services. Similar point of view is also presented by other researchers.
Laparoscopic cholecystectomy is widely considered as the treatment of choice for acute cholecystitis, and it can be performed safely on selected patients. Surgery in patients with neutropenia, thrombopenia, and sepsis who have acute abdomen is however associated with a high mortality. Percutaneous cholecystostomy was described as a minimally invasive, image-guided procedure and has become an alternative treatment strategy for high-risk patients with acute calculous or acalculous cholecystitis who are unfit for emergency surgery. 11 –14 Also, percutaneous cholecystostomy could be used as a method for removal of the gallbladder which is a source of sepsis in unstable and ill patients. The safety of the procedure and its minimal invasiveness made it a valid treatment option for a patient not responding to antibiotic therapy. Our research shows that patients positively assess this treatment method, but the world’s tendency is to currently use more sophisticated methods and robot-assisted surgery as the gold standard.
Experiences from the US hospitals show that each year about 1 million people undergo gallbladder removal surgery, and 40% are women aged between 18 and 44 years. 15 This tendency is also visible in Poland, as exemplified by Kujavian–Pomeranian region. Women dominated in both the analyzed groups—70% of all respondents. John Harding, president and chief executive officer for Florida Hospital Tampa, observed that providing patient with minimal invasive surgical procedures that utilize the state-of-the-art equipment like da Vinci Robotic Surgical System underscores commitment to quality patient care while enhancing patient safety. The advantages include minimal invasive scarring, less pain and bleeding, faster recovery time, and shorter hospital stay. The move toward less invasive and less morbid procedures and a need to re-create the true, open surgical experience have paved the way for the development and application of robotic and computer-assisted systems in surgery in the world and also in Poland. Robot-assisted surgical systems have already been used in humans to perform procedures in cardiac surgery (internal thoracic artery, mitral valve repair, and total coronary bypass), 16 –19 general surgery (cholecystectomy, inguinal hernia repair), 16,20 and urology (radical prostatectomy). 21 –23 Systems such as the minimally invasive da Vinci Surgical System have been known to facilitate and improve the performance of endoscopic surgery by allowing surgeons to use open surgical movements and techniques while maintaining the benefits of access through keyhole incisions. 24 Robotics is being used for gallbladder surgery, endoscopy, and many other surgeries. 25
Robotic surgery works as follows: the surgeon looks into a viewfinder to see images being sent by a camera that is positioned inside the patient. Images show the surgical site and the surgical instruments. Controls, much like a joystick, are used by the surgeon to manipulate the instruments and perform the surgery.
The term robotics is defined as the use of a robot to perform various functions. A robot has movable physical structure, a power source, a sensor system, and a computerized “brain” to control activities. In the future, surgeons will use robotics to perform surgical tasks. Robotics still requires the expertise of a surgeon to operate, but the instruments used by robotics improve the control, the precision as well as often minimize the invasiveness of the surgical procedures. In other words, the outcome of any surgery is directly associated with the surgeon’s skill. Highly skilled surgeons attain expertise through years of training and experience. Expertise with robotic surgery is limited and varies widely among both hospitals and surgeons. Although there may be some advantages to the use of robotics in general surgery, especially for operational treatment of cancer that requires extensive surgery and removal of lymph nodes, this study has shown that adding this expensive technology to a routine surgical care does not improve the outcome in a patient (outcome of the surgery), especially when compared and referred to the safety and effectiveness of the conventional surgery. Dharia et al 26 compared robotic surgery with open technique and found that there exists a significantly longer operative time if a robotic system is used (201 minutes in robotic surgery vs 155 minutes in open surgery). However, they observed a significantly shorter length of hospital stay (4 days in robotic surgery vs 35 hours in open surgery) and a faster return to normal routine for patients (11 days in robotic surgery vs 28 days in open surgery) in cases of medical procedures such as tubal reanastomosis. Nezhat et al 27 also noted longer average surgical time for robotic myomectomy (234 minutes) than that of laparoscopic myomectomy (203 minutes). The same author also found that postoperative complications were not significantly different between the conventional and robotic surgeries in case of a myomectomy procedure. Other researchers also 28 confirm that the robotic surgery lasts for a significantly longer time as an operational procedure than the conventional and laparoscopic surgeries. The time for robotic surgery is around 50 minutes longer than the conventional surgery, and it is the time that is required for docking and undocking the surgical robot. The MRCAS cannot replace doctors but can help achieve higher standards of hospitalization by reduced hospital length of stay and faster recovery time for patients.
Technologies that increase the precision and accuracy of surgery have obvious appeal to the general public. The structure of the hospital industry is changing due to the use of MRCAS as hospitals consolidate and other health care options such as walk-in surgical clinics become available to consumers. Private and government health insurers around the world are becoming more cost conscious, forcing hospitals to reevaluate their capital spending plans but strengthening the technologies that can reduce the cost of surgical procedures in the near future. In such a fast-moving field as medicine, there is a pressing need to develop and maintain an up-to-date base of market information in order to better understand the dynamics of the market for MRCAS devices and equipment that will influence patient safety. Experience from more specific objectives on medical market in the United States and Poland suggests that there is a strong need to start: to identify and evaluate the impact of demographic, economic, and other factors that will drive future demand for MRCAS devices that are an added value for patient care and also to identify promising new surgical procedures and products still in the development and testing stages and assess the probability that they will be commercialized successfully on the medical market within the next years.
Although many research articles are structured around specific technologies, they are largely nontechnical in nature. However, the specifics of medical market need more information both in medical and in technical perspectives and pertaining to patient safety. These are necessary for better understanding of the specifics of robotics in medicine and in minimally invasive methods for users and patients in the Polish health care system. Experience from many European countries shows that minimally invasive methods and robots such as the da Vinci system are very useful for patients and doctors. Although experience from the health care organizations indicated the legitimacy of the use of this new treatment method—especially in general surgery, cancer patients’ surgery, organ transplants with a family donor—the cost of this new method is too high and not refunded by Polish National Health care system. Also, most of the minimally invasive treatment methods are more costly in the short term; however, in a global aspect, the costs of patient treatment are similar to standard (open surgical procedure) but are safer for patients. Our study shows that the MIS is assessed by patients as safer, and the patients’ psychological condition after such surgery is better than those after a traditional surgery.
The revolution in surgery and communications is being implemented in hospital practices, starting with minimally invasive methods via robots. Robots are automated systems providing significant improvement in the accuracy of surgery. Robot-assisted surgery is a natural consequence of patient’s increasing expectations and implementation of new technology in the medical sector. In Poland, the aging population has expressed a demand for technologically advanced medical service, especially in areas such as orthopedic, general, and spine surgeries.
Compared with other MIS approaches, robot-assisted surgery gives the surgeon better control over the surgical instruments and a better view of the surgical site. Also, patients assess hospital equipment better when the new technology and new technics of treatment are present, and the patients are more often willing to recommend hospital services to their family or friends. New technology gives surgeons new possibilities. Surgeons no longer have to stand throughout the surgery, do not tire as quickly, and their hand tremors are filtered out by the robot’s computer software. The surgical robot can also be used continuously by rotating surgery teams. This fact also has an influence on better hospital care when patients stay at hospital and patients’ safety is improved. There is also the argument that the robotic surgical techniques and all minimally invasive treatment methods benefit hospitals by reducing the length of patients’ stay, thereby enabling better cost management and improving the organizational culture of a hospital. This factor is driving demand for new technology in surgery and surgical robot systems. Since robotics provides surgeons with precise, repeatable, and controlled ability to perform procedures in tight spaces, it is increasingly in demand. The MIS and all robotic systems such as da Vinci system allow for improved outcomes in patients, such as minimal blood loss and tissue damage, smaller incisions, less scar tissue, decreased length of hospital stay and recovery time, diminished postoperative pain, and a faster return to normal activities. These are important facts from patient’s point of view.
Comparing robotic surgery and laparoscopic surgery, we note that robotic surgery is similar to laparoscopic surgery in the sense that surgical instruments are inserted into small incisions in a patient’s torso and manipulated by the surgeon. In robotic surgery, however, the surgeon sits at a console in the operating room and uses hand and foot controls to manipulate surgical tools attached to a robot’s arms. Both types of surgery may result in quicker recovery times, less blood loss, and less pain for patients, compared with traditional “open” surgeries performed through a larger incision. Robotic and laparoscopic surgeries (eg, in hysterectomy procedure and general surgery) are essentially equivalent with regard to the surgical treatment and clinical outcome of treatment. As reported at the Congress of the Society of Laparoscopic Surgeons, there were no differences between the 2 types of surgeries (robotic surgery and laparoscopic) with regard to the length of postoperative hospital stay, the amount of blood lost, and tissue damage. Also, many studies 29 –33 show similar results and confirm that robotic surgery is as safe and effective as laparoscopic surgery. During these 2 types of surgical procedures, blood loss is low and a patient’s hospital stay is shorter. In other words, studies in cases noted that none of the patients required a blood transfusion, and there were no complications directly related to blood loss. Robotic surgery is an excellent technology that may aid some physicians in the transition to a less invasive approach to surgery.
Typical indications for using a robotic surgery include patient’s and physician’s preference. Patient preference may be driven by patient-to-patient recommendation. Physician’s preference is based on the physician’s training and experience with each modality including traditional laparoscopy, open, and robotic methods. Learning and incorporating the robotic technique is certainly desired, as all surgeons should be familiar with the full spectrum of available methods for treating patients. However, physicians should not relinquish their hard learned and mastered traditional laparoscopic techniques. Robotic surgical system was developed to overcome the existing clinical constraints and to meet market demand for a more patient-friendly approach to surgery and patients’ better psychological condition after surgery. Patients themselves also assess the MIS and all robotic systems as important and safer for their health.
All MIS methods of treatment and robotics in medicine are showing great results in many ways, especially in the area of surgery. However, it should be remembered that surgical procedures are not the only place where robotics can be used in medicine. Developers are continuously working on new ways to allow robotics to perform tasks in hospital practices. One area that is especially promising is the control of diseases and the prevention of diseases being spread, that is, the areas that could be harmful for hospital personnel can be sterilized using robots. Some other types of procedures include sterilizing floors, delivering laboratory specimens, and pulling patients from stretchers to rooms. In the future, we can expect a significant development in information technology systems and new technology in medicine and an increase in the demand for robotics and new mechanical (automatic and fully controlled) systems working in organization such as hospital.
Footnotes
Acknowledgments
The authors would like to thank all contact persons from the participating hospitals of Kujavian and Pomerania region (Poland) for distributing and collecting the questionnaires and also the managers of those hospitals for agreeing to conducting this study in their hospitals.
Authors’ Note
Anna Rosiek and Krzysztof Leksowski contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.