
Abstract
Introduction
The prognosis of patients with uveal melanoma is related to several factors, including local or extraocular extension of the disease. Up to 50% of the patients with initial diagnosis of uveal melanoma develop metastases within few years and the liver represents the main site of metastatic spread. Patients with metastatic disease have a generally poor prognosis and few treatment options are available. In the last decades, the role of interventional radiology has expanded the range of treatment options and different minimally invasive liver-directed therapies were developed for liver metastases from uveal melanoma. The purpose of our systematic review was to analyze and review techniques, outcomes and safety of targeted-liver minimally invasive therapies in patients with metastatic uveal melanoma.
Methods
According to PRISMA criteria, an extensive literature research (including more than 1600 articles) was finalized to collect the main articles on minimally invasive therapies. Based on the inclusion and exclusion criteria, 26 studies were selected for inclusion in the present systematic review (20/26 articles were retrospective studies, 6/26 articles were prospective studies). We collected data on 955 patients underwent the following procedures: radioembolization, transcatheter arterial chemoembolization, transarterial immunoembolization, percutaneous hepatic perfusion and thermal therapies.
Results
Among procedures analyzed, the median overall survival was 16 months, the median progression-free survival was 8.2 months, while the median overall response rate was 39%. Post-procedure haematologic and gastrointestinal adverse events were predominant after percutaneous hepatic procedures.
Conclusion
To date, different minimally invasive therapies are available for the treatment of metastatic uveal melanoma. Studies on percutaneous liver-directed therapies have demonstrated improvement in outcomes, prolonging overall survival and progression-free survival, and with an acceptable safety profile.
Keywords
Introduction
Uveal melanoma (UM) is the most common primary intraocular malignant tumor in adults with an incidence of 5-7 cases per million person-years in Europe and in the USA. 1
UM arises from neural crest-derived melanocytes precursors of the uveal layer of the eye, and it involves in descending order of frequency the choroid (90%), the ciliary body (7%) and the iris (3%).2,3 To date, three different histologic types of uveal melanoma are described: spindle cell type, mixed cell type and epithelioid cell type, the latter being related to a more severe prognosis.4,5 Although the diagnosis of UM is almost exclusively clinical and ophthalmological, radiologic imaging techniques play a crucial role in the detection and characterization of the tumor, in the evaluation of the local extent of the disease and in the identification of distant metastatic lesions. 6 The prognosis of uveal melanomas is related to several factors, including histopathologic features, genetic and molecular patterns, local or extraocular extension of the disease. Epithelioid cell type, monosomy 3, ciliary body invasion are the main prognostic factors associated with worst prognosis and higher risk of metastases.6-8 Furthermore, patient overall survival mainly depends on tumor size, extraocular spread, and distant metastases. In the last decades, significant improvements in the local treatment of UM were made through the development of globe-sparing therapies. However, approximately 50% of the patients with initial diagnosis of UM develop metastases within few years during the course of the neoplastic disease. 9 Systemic metastases of UM may be widespread and disseminated disease has a generally poor prognosis and few treatment options. In the setting of a predominantly haematogenous spread of the tumor, the liver represents the main site of metastatic spread followed by lung, bone, kidney, skin, lymph nodes and, less frequently, brain. The presence of metastatic disease represents the main cause of death in patient with uveal melanoma and the development of liver metastases represents a key clinical determinant of patient survival. 10
Treatment of UM encompass both local and systemic therapies. Among the first, globe-sparing therapies aim to preserve vision function and to avoid metastatic spread of the disease; in particular, radiation therapies are preferred to surgery since no difference in the survival rate of patients were showed by different studies in the literature. 11 Enucleation is currently the treatment indicated for large tumors (basal diameter > 20 mm, thickness > 12 mm), for tumor involving the optic nerve and for tumor complications. Systemic therapies include chemotherapy, immunotherapy and molecular targeted therapies which are performed and reserved in metastatic disease. 12
The liver is the main site of metastases in patient with UM since neoplastic cells have an elective tropism for hepatic parenchyma due to tumor biology. 13 Patients with liver metastases present a median overall survival of less than six months and a dramatic increase in mortality, making treatment options of this condition a crucial issue in the therapeutic pathway of the disease.14,15 Surgical resection of liver metastases is reserved for selected cases and suitable in a low percentage of patients since metastatic disease often involves both liver lobes with multiple lesions at presentation. Currently, therapy of advanced disease mainly consists of chemotherapy and immunotherapy; however, the former has not yet proved to be really effective for metastatic disease, while, among the latter, important results were obtained with the development of Immune mobilizing monoclonal T-cell receptors Against Cancer (ImmTACs), fusion proteins that bind to a target antigen presented by human leukocyte antigen (HLA) of the cell.15,16 To date, tebentafusp, an ImmTACs, is the first approved treatment for adult patients with unresectable metastatic uveal melanoma and positive for HLA-A*02:01 leukocyte antigen.
In recent years, the role of interventional radiology has expanded the range of treatment options available for liver metastases from uveal melanoma. Liver-directed therapies encompass chemoembolization, radioembolization, immunoembolization, thermal ablation and percutaneous hepatic perfusions.17,18 Such minimally invasive therapeutic approaches have different advantages, allowing the release of therapeutic agents into the target lesions, the reduction of systemic toxicity and complication rate and the reduction of the length of hospitalization compared to more invasive alternative therapies. 11 Locoregional therapies also aim to stabilize liver metastatic lesions and to arrest the disease progression.
The purpose of our study is to analyze and review techniques, common clinical practice, outcomes and safety of targeted-liver minimally invasive therapies in patients with metastatic uveal melanoma. Our work systematically reviews clinical trials, prospective and retrospective studies concerning this topic.
Materials and Methods
Systematic Review
An extensive systematic literature search in the field of the treatment of liver metastases from uveal melanoma was performed in accordance with the “PICo” criteria and “Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA)” guidelines. The literature search included PubMed, Embase, Google Scholar, Cochrane Library and Medline databases and the following medical subject headings (MeSH) and keywords, associated with Boolean operators, were used to identify articles relevant to our purpose: “uveal melanoma metastasis/metastases” OR “choroidal melanoma metastasis/metastases” AND “liver”; “uveal melanoma” OR “choroidal melanoma” AND “liver metastases/metastasis”; “uveal melanoma metastases/metastasis” OR “metastatic uveal melanoma treatment” AND “interventional radiology”; “uveal melanoma metastases/metastasis” OR “metastatic uveal melanoma treatment” AND “percutaneous therapy/therapies”. The “PICo” items formed the basis of the research question and included the following information: P (patients with diagnosis of uveal melanoma and with evidence of liver metastases on cross-sectional imaging), I (minimally invasive treatment of liver metastases from uveal melanoma), C (comparison between different interventional radiology procedures), O (effectiveness outcomes, overall survival, adverse effects and adverse effects limiting effectiveness of treatment), S (retrospective study, clinical trial phase III, randomized controlled phase III trial, prospective pilot study, retrospective cohort analysis, multicentric randomized trial, phase II trial reports, other prospective studies).
The literature search was performed from January to November 2024. The study protocol of our systematic review was registered in the International Platform of Registered Systematic Review and Meta-Analysis Protocols-INPLASY (registration number: INPLASY202520101). Our study did not directly involve humans, and therefore did not require the Institutional Review Board approval of our Institution.
Eligibility Criteria
Only human studies, articles written in English and those where the entire content was accessible were included in the present review. No interval in the search period was specified. Study design required as inclusion criteria were prospective, retrospective observational or cohort studies with more than ten patients. Case report, case series, narrative or systematic review, meta-analysis and guidelines were considered as not eligible and were excluded. Exclusion criteria were also: articles written in other language than English and those whose entire content could not be accessed; articles that were not compatible with the aims of our research due to the use of not specific MeSH and keywords and recurring articles from the same authors on the same procedure.
Patients
The study population inclusion criteria were as follows: adult patients (aged 18 or older) with a histologically confirmed diagnosis of uveal melanoma; patient with detection of hepatic metastases determined by liver directed cross-sectional imaging examination; patients not eligible to surgical treatment. The exclusion criteria were: patients with cutaneous melanoma or with tumors other than UM; patient with autoimmune disease or immunosuppressed; patients without radiological abdominal imaging; patients with an Eastern Cooperative Oncology Group (ECOG) performance status >2.
Intervention
In the present review only studies focusing on the minimally-invasive liver-directed therapies were included: radioembolization (selective internal radiation therapy – SIRT / transarterial radioembolization - TARE), transcatheter arterial chemoembolization (TACE), transarterial immunoembolization (TAIE), percutaneous hepatic perfusion (PHP) and thermal therapies were analysed in each study selected. Combination of the aforementioned therapies was also allowed. Patients underwent others liver surgical therapies were excluded from the study.
Outcome Measures
Regarding the type of treatment, materials, techniques, technical and clinical success were analysed for each procedure. Whenever possible, data on specific materials used for subgroups of patients undergoing treatment were indicated. The statistics on technical success, clinical success, and complications were compared when available. Study outcomes parameters evaluated were: overall survival (OS), progression-free survival (PFS), overall response rate (ORR), and safety. According to the National Cancer Institute, OS is defined as “the length of time from the date of the start of treatment for a disease, such as cancer, that patients diagnosed with the disease are still alive”, PFS is defined as “the length of time during and after the treatment of a disease, such as cancer, that a patient lives with the disease but it does not get worse” and the ORR is defined as “the percentage of people in a study or treatment group who have a partial response or complete response to the treatment within a certain period of time”. 19 Furthermore, predictors for prolonged OS were also analyzed. PFS and OS were measured from date of first treatment until disease progression or death or last follow-up. The median ORR was determined based on Response Evaluation Criteria in Solid Tumors (RECIST) using cross-sectional imaging (CT and/or MRI). Complications and adverse events reported in the included studies, with or without clinical implications, were analysed during follow-up period; they were also standardized with the Common Terminology Criteria for Adverse Events (CTCAE v5.0) system, which classified the severity of side effects into 5 grades. 20 Adverse events and complications were also divided into minor (grade 1-2) and major (grade 3-4-5).
Study Selection
All included articles based on keywords and MeSH were examined by two different reviewers among authors and disagreement over the literature data were settled through discussion among the other authors. In doubtful cases, articles were included in this stage named “uncertain” and required the evaluation of the full text to make the final decision. First author, year of publication, design of the study, patients enrolled, type of procedure, outcomes and complications were extracted from each study. For each group of patients, age, sex (male or female) and the ECOG scale were identified. Data were recorded using Microsoft Excel database (Microsoft Corporate, version 2403, Redmond, WA, USA).
Based on the aforementioned keywords and MeSH, 1651 records were identified and of which 105 were removed because they were duplicated or because the full-text was not available. 104 articles were removed because they were systematic review or meta-analysis and 238 articles were excluded because they were case reports or case series or editorials or guidelines. 104 articles were also removed because written in a language other than English and 190 articles were removed because were studies on animals. From the analysis of the titles and abstract, 1091 articles were identified as potentially to be included; subsequently, 1073 articles were removed as they were not relevant for the purpose of our study. Based on the inclusion and exclusion criteria, the articles considered for our research were reduced to 18 papers. Further 8 articles have been added analysing cross-references from previous included studies. The systematic review of the literature was finally conducted on a total of 26 articles.21-46 The whole process of selecting studies based on the inclusion and exclusion criteria is summarized in a flow-chart illustrated in Figure 1.

Flow-Chart Illustrating Selection Process Of The Articles Included In The Systematic Review.
Definitions
In recent years, minimally invasive therapies have provided a viable alternative to more invasive surgical therapies and to systemic chemotherapy and aim to halt disease progression. Liver-targeted therapies encompass TACE, immunoembolization, hepatic perfusion and radioembolization. Such therapies allow high doses of chemotherapeutic agents to be delivered within the tumor and reduce the toxicity rate of systemic therapies. The following sections outline the main characteristics of minimally invasive treatments of liver metastases from uveal melanoma analyzed in the systematic review.
Transcatheter Arterial Chemoembolization (TACE)
TACE is a minimally invasive procedure which allows the administration of high concentrate dose of different chemotherapeutic agents (cisplatin, fotemustine, melphalan) directly into the tumor via a catheter through a percutaneous transarterial approach under digital subtraction angiography (DSA). Since liver tumors are nearly exclusively fed by the hepatic artery, TACE preferentially delivers the chemoembolization drug compound directly in the vascular bed of the tumor minimizing hepatic parenchymal injury; this allows the permanence of the drug in tumor site and the ischemia of the neoplastic tissues. Chemotherapeutic agents can be administered as a mixture with ethiodized oil (known as conventional TACE) or as an injection of microspheres/drug-eluting beads (known as DEB-TACE): in the first case, the administration of the chemotherapeutic agent is followed by embolization, typically with gelfoam or polyvinyl alcohol (PVA) particles, while in the second case 100-300 µ drug releasing spheres are used. Through the Seldinger technique, a 4 or 5 Fr curved catheter is advanced to selectively catheterize the celiac tripod and the common hepatic artery. Subsequently, serial arteriograms are performed to outline the downstream vascular anatomy. At this point, a guidewire and a microcatheter will advance in order to negotiate the arterial vessels that supply the tumor, allowing the release of the drug. After procedure, patients are monitored and they could be discharged in the same day or hospitalized for one night for observation. The post-procedural results will be obtained after at least a month and a second intervention could be performed at 4- to 6-week intervals if necessary. The main procedure-related complications include post-chemoembolization syndrome (up to 80% of patients), thrombosis, infection and non-target embolization. The median overall survival after TACE ranges between 9 and 21 months.16,47
Transarterial Radioembolization (TARE) - Selective Internal Radiation Therapy (SIRT)
The procedure consists of the transcatheter administration of small radioactive particles via the hepatic artery. The microspheres are deposited within microcirculation inside and around the tumor and cause the death of neoplastic cells through the effects of radiation, sparing the surrounding healthy liver parenchyma (or at least only a low and tolerable dose). Microspheres contain resin labelled with Yttrium-90 (a beta emitter with a maximum soft-tissue penetration of 11 mm) or Lipiodol labelled with I-131. The average tumor radiation doses exceeding 200 Gy are obtained. Before infusion of the microspheres, the extrahepatic branches are embolized. After the infusion, the catheter is removed and gamma camera images are usually taken using the Bremsstrahlung radiation produced by the beta particles to obtain images of where the spheres are located. However, in order to access both lobes of the liver, two separate procedures are usually performed at least four weeks apart to ensure that adequate liver function is maintained. 16
Percutaneous Hepatic Perfusion (PHP)
This is an innovative procedure in which the liver is endovascular isolated and perfused with a high concentration of melphalan, a chemotherapeutic agent. This technique was developed mainly for the treatment of liver metastases in patients without significant extrahepatic disease; the administration of a high-dose of chemotherapeutic drug to the liver maximizes the efficacy on metastases, but reduces its systemic toxicity. The procedure is performed in an angiographic suite under general anesthesia by a multidisciplinary team composed of an interventional radiologist, an anaesthetist and an extracorporeal perfusionist. The inferior vena cava is occluded using a double-balloon catheter placed through the common femoral vein. A catheter is inserted first via the femoral artery and then into the hepatic artery: at this point melphalan is administered (2.5-3.0 mg/kg of body weight up to a maximum dose of 220 mg at a rate of 0.4 mL/s) for approximately 60 min. An extracorporeal filtration system filtered the hepatic venous blood with melphalan, allowing the elimination of the drug, before the reinjection of the chemotherapeutic agent into the systemic circulation through a central venous access. During the procedure, an angiogram is performed to test flow in the hepatic artery, and vasodilator medications are applied if vasospasm is limiting flow.35,48
Transarterial Immunoembolization (TAIE)
TAIE is an emerging therapy in the treatment of metastases from uveal melanoma and it combines liver metastases ischemia with administration of granulocyte macrophage colony-stimulating factor (GM-CSF), inducing an inflammatory alteration in the tumor and peritumoral tissues leading to a systemic immune response against antigen cells exposed after ischemic injury induced by embolization. The result is an “in situ tumor vaccine”. In particular, a cytokine with immunostimulant action GM-CSF (granulocyte-macrophage colony-stimulating factor, glycoprotein mainly produced by activated T cells), emulsified in ethiodized oil, is administered at various doses, range from 25 to 2000 µg. This treatment is performed every four weeks until disease progression or unacceptable adverse events occur. Immunoembolization with GM-CSF is designed to enhance local and systemic immunity against tumor cells: immunostimulatory cytokines facilitate remodelling of the immunological environment in the liver. This procedure could follow embolization of the hepatic arterial branch that vascularizes the metastasis; subsequently, infusion of GM-CSF post-embolization may improve local antitumor immune response. 16
Other Percutaneous Therapies
Percutaneous loco-ablative thermal therapies were historically used to treat different metastatic diseases. Thermal therapies use percutaneous devices causing heat induction, cellular damage, and coagulative necrosis under local anaesthesia. Patients with uveal melanoma were successfully treated with Radiofrequency (RFA) and microwave (MWA) thermal ablation for liver oligometastatic (< 3 lesions) disease. RFA use one or multiple electrode/applicators inserted percutaneously under imaging guidance (US, CT, MRI) consisting of a closed-loop circuit that includes an RF generator (150-250 watt), an electrode needle and a dispersive electrode (grounding pad); an alternating current within the RF spectrum (300-500 kHz) causes ionic agitation and local heat (centrifugal ablation) through the Joule effect. The procedure time is 10 to 16 min. MWA use one or more applicators (needle-like elements) inserted percutaneously under imaging guidance and generating a closed circuit between two electrodes. Rapidly oscillating electromagnetic field around the applicator (900-2450 MHz) causes the rotation of water molecules (friction energy delivery mechanism) generating heat damage. The procedure time is under 10 min.
In MRI-guided laser-induced thermotherapy, a laser applicator generates an area of coagulative necrosis around the optical fibres tip device that disperses light energy; the destruction of tumor cells occurs directly applying thermal energy and limiting damage to surrounding tissues.15,30
Quality Assessment and Risk of Bias
The Newcastle-Ottawa scale was used to assess the quality and risk of bias of non-randomized studies (case control studies and cohort studies) included in our systematic review (Tables 1 and 2).49,50 The risk of bias for randomized studies was evaluated using the Cochrane scale (Table 3). 51
Risk of Bias based on Newcastle-Ottawa Scale.

Risk of Bias Based on Newcastle-Ottawa Scale.

Low 
High 
Some concerns 
Cochrane Risk-of-Bias Tool for Randomized Trials – RoB 2.

* Domain 1: risk of bias arising from the randomization process; Domain 2: risk of bias due to deviations from the intended interventions (effect of assignment to intervention); Domain 2 bis: risk of bias due to deviations from the intended interventions (effect of adhering to intervention); Domain 3: risk of bias due to missing outcome data; Domain 4: risk of bias in measurement of the outcome; Domain 5: risk of bias in selection of the reported result.
Results
According to the inclusion and exclusion criteria, 26 studies were selected for inclusion in the present systematic review. 20/26 articles were retrospective studies and 6/26 articles were prospective studies, one of which was a clinical trial phase I study, one was a clinical trial phase II study, one was a pilot study, and two were clinical trial phase III studies. We collected data on 955 patients, 445 male (46.60%), 510 female (53.40%), affected by uveal melanoma with liver metastases identified on cross-sectional imaging and subsequently underwent percutaneous minimally invasive treatment. The mean age of the entire population included in the study was 59.1 years (range, 19-89 years).
9/26 studies (497 patients) focused on PHP treatment, 8/26 studies (245 patients) on TACE treatment, 5/26 studies (102 patients) on TARE, 3/26 studies (93 patients) on TAIE, and one article (18 patients) on percutaneous laser-induced thermotherapy (LITT). All TACE and TAIE procedures were conducted under local anesthesia, while PHP procedures were conducted under general anesthetic; in TARE procedures, patients were placed under conscious sedation or general anesthesia. Different types of drugs and embolic agents were analyzed in all studies. In TACE procedures, chemotherapeutic drugs used were melphalan (dosage 1 mg/kg), fotemustine (dosage 50 mg/m2 of body surface), 1,3-bis-(2-chloroethyl)-1-nitrosourea (BCNU - dosage 200 mg), drug-eluting beads loaded with irinotecan (DEBIRI - dosage 100 mg of irinotecan loaded in 100-300 µm beads), CPT-11 (irinotecan) loaded drug eluting beads, cisplatin (dosage 70 mg/m2 of body surface). All TARE procedures were conducted using Yttrium 90 microspheres (the median and the mean dose delivered per patient was respectively 48.1 mCi and 45.02 mCi). In PHP, the drug used during the procedure was melphalan (dosage 3 mg/kg, max 220 mg per session). GM-CSF associated with ethiodized oil and gelatin sponge was the therapy used in all TAIE procedures. The use of calibrated microparticles (ranging from 250 to 700 µm), adsorbable gelatine sponge or ethiodized oil has been found in various studies, and in all TACE procedures chemotherapeutic agents were associated with embolizing agents. The median number of procedures per patient were 3.2 for TACE, 2 for PHP, 1.7 for TARE and 6 for TAIE.
The main characteristics of the studies included in this systematic review are summarized in the Table 4.
Main Characteristics of the Studies Included in the Systematic Review.

Among studies, post-operative outcomes and complications were evaluated during the follow-up period. Treatment response was assessed using cross-sectional imaging scheduled between 4 to 8 weeks after each procedure. The median overall survival (OS) was available for all articles analyzed and it was 16 months with a standard deviation of 6.7, while the mean OS was 16.4 months. The median PFS was available for 22/26 studies and it was 8.2 months with a deviation standard of 2.9, while the mean PFS was 8.1 months. The median ORR was 39% with a standard deviation of 0.2, and the mean ORR was 38%. The median OS was higher for laser-induced thermotherapy procedure (32 months), followed by TAIE (20.4 months), TARE (17 months), PHP (15.3 months), and TACE (13.5 months). The median PFS was higher for TAIE procedures (10.4 months), followed by PHP (8.4 months), TACE (6.6 months), and TARE (5.1 months). The median ORR was higher for PHP procedures (53%), followed by TAIE (32%), TARE (27%), and TACE (24%). The post-operative outcomes available for the studies analyzed in our systematic review are summarized in the Table 5.
Outcome Parameters Evaluated in the Included Studies.

Technical success was achieved in all procedures analyzed in the revised studies. Post-procedure adverse events and complications were divided into minor (grade 1-2) and major (grade 3-4-5), according to the Common Terminology Criteria for Adverse Events (CTCAE v5.0) system. The analysis of major adverse events was available in 25/26 studies (96.1%), while the analysis of minor adverse events was described in 14/26 articles (53.8%). Haematological toxicity (trombocytopaenia, anemia, leukocytopaenia) was the main major adverse event found in the revised articles, followed by liver toxicity. Post-procedure haematologic adverse events were predominant after PHP procedures. In six cases (five patients post-PHP procedure and one patient post-TACE procedure), adverse events were grade 5 and unfortunately led to an ominous outcome for patients. The major (grade 3-4-5) adverse events affected 812/955 patients with an overall rate of 85%. However, only a few of them required hospitalization and most of them resolved without sequelae. The overall mortality among liver-directed therapies was 1.2%; PHP was the procedure with the highest mortality rate (0.9%).
Gastrointestinal symptoms followed by haematologic toxicity were the most prevalent minor adverse events (grade 1-2) among studies reporting this data. The number, rate and type of major and minor adverse events and complications described in the individual studies are collected in the Table 6.
Complications Rate and Adverse Effects After Liver-Directed Therapies.

*Grading according to National Cancer Institute Common Toxicity Criteria for Adverse Events, version 5.0.
**Not available.
Discussion
Uveal melanoma is the most common primary intraocular malignant neoplasm in adult and it encompasses three different histopathological subtypes characterized by different genetic and prognostic profiles. The prognosis of UM is strongly related to histopathologic features, genetic changes, and chromosomal alterations. Epithelioid cell type, monosomy 3 (gain of chromosome 8q), and driver gene mutations (BAP1), have the high metastatic risk and the worst prognosis with a 75% 15-year mortality rate. 6 Recent advances in molecular biology have also outlined specific gene mutations and chromosomal alterations, such as mutations in BAP1 (BRCA1-associated protein 1), CYSLTR2 (cysteinyl-leukotriene receptor 2), GNAQ/11 (G protein subunits alpha q/11), PLCβ4 (phospholipase C beta 4), and alterations in cellular signaling pathways (JAK/STAT, mTOR and β-catenin pathways).
In the last decades, important improvements were made in the local therapy of uveal melanoma. Enucleation and globe-sparing therapies allow the disease to be controlled and to prevent metastatic spread. However, up to 50% of the patients with UM develop metastases within few years despite successful treatment of the primary tumor. 52 Since the tumor develops rapid angiogenesis, uveal melanoma tends to metastasize haematogenously, more frequently to the liver and then to other organs. Metastatic disease has a severe prognosis, representing the major cause of death. 53 Therefore, the successful treatment of metastatic disease, and in particular of liver spread, improves the prognosis of patients. Unfortunately, most patients are not eligible for surgical resection at the time of diagnosis of extraocular involvement due to multifocality of liver metastases. Nowadays, the first-line treatment of metastatic uveal melanoma includes systemic chemotherapy and immunotherapy. The most widely used conventional chemotherapy agents are dacarbazine (gold standard), fotemustine, and temozolomide, although studies have also been conducted with regimens that have combined chemotherapy drugs such as bleomycin, vincristine, lomustine and dacarbazine (BOLD scheme) with IFN-alpha. However, combined regimen of chemotherapeutic drugs has not yet confirmed a clear synergistic activity at the expense of significant side effects. 54 Immunotherapy (nivolumab, pembrolizumab or ipilimumab) and checkpoint inhibitors have shown poor response rates in different trials and retrospective studies, as UM is a less immunogenic tumor compared to cutaneous melanoma. On the other hand, a new class of drugs, named immune-mobilizing monoclonal T-cell receptors against cancer (ImmTACs), has been developed, and a major breakthrough was in 2021 when tebentafusp was the first ever drug that in a randomized phase III trial showed a survival benefit over best alternative care. 15 Tebentafusp is a T-cell receptor-bispecific molecule targeting glycoprotein 100, a peptide–HLA complex on the target-cell surface, and CD3; this molecule resulted in longer overall survival than conventional chemotherapy and immunotherapy, and it is now approved for the treatment of adult patients with unresectable metastatic uveal melanoma and positive for HLA-A*02:01 leukocyte antigen. 55
Since metastatic UM has an intrinsic chemoresistance, percutaneous locoregional therapies have become increasingly relevant for the therapy of liver metastases from uveal melanoma; the reason is twofold: percutaneous treatments are minimally invasive therapies which can treat patient with comorbidities or in which surgical or systemic therapies are contraindicated; liver locoregional therapies allow the delivery of a concentrated dose of chemotherapeutic agents to metastatic lesions with a reduced systemic toxicity. 11 Furthermore, patients with multiple metastases are not candidates for surgery and systemic chemotherapeutic regimes are characterized by relevant side effects and often showed only marginal efficacy in metastatic uveal melanoma.
The aim of our study was to review the results and outcomes of percutaneous locoregional therapies directed to liver metastases from UM, and an extensive literature research was finalized to collect techniques, outcomes and safety of patients. In fact, while locoregional control of the primary tumor in the eye has achieved excellent results, the same has not been true for the control of metastatic disease, and especially for liver spread which gives patients a poor prognosis. Therefore, survival of patients with metastatic UM correlates strongly with disease control in the liver. In our study, we analyzed the median overall survival, PFS and objective response rate of various studies as outcomes parameters, in order to demonstrate how well these treatments work. We also focused on timing of follow-up period, on methods of hepatic radiological response, on techniques and toxicity of various procedures analyzed. The most robust collection of articles included in our systematic review focused on five different locoregional liver-directed therapies: TACE, transarterial radioembolization, PHP, TAIE, and percutaneous loco-ablative thermal therapies.
TACE is a well-established treatment in patients with multinodular hepatocarcinoma according to Barcelona Clinic Liver Cancer (BCLC) staging system; in liver metastasis from uveal melanoma, it has been used for thirty years and several different chemotherapeutic agents were tested for this procedure. One of the first TACE treatment was performed by Mavligit et al in 1988, who treated 30 patients with liver metastasis from uveal melanoma using cisplatin as chemoembolic agent and achieved an OS of 11 months and an ORR of 46%. 56 These encouraging results prompted many centers to perform such treatments and different chemotherapy agents were used. In our systematic review, we selected 8 studies focused on TACE treatment and the drugs used for chemoembolization were melphalan, fotemustine, 1,3-bis-(2-chloroethyl)-1-nitrosourea (BCNU), cisplatin, drug-eluting beads loaded with irinotecan (DEBIRI) and CPT-11 (irinotecan) loaded drug eluting beads. In our analysis, the median OS of patients underwent TACE was 13.5 months, with a median overall survival and ORR higher for patients treated with fotemustine, an alkylating agent introduced in the 1990s for the treatment of metastatic uveal melanoma. 57 This agent reaches high hepatic concentrations thanks to its short half-life and high first-pass liver extraction, as reported by Edelhauser et al in their retrospective analysis. 26 On the other hand, Gonsalves et al hypothesized the superiority of BCNU, a lipophilic agent, to water-soluble agents as the former easily dissolves in ethiodized oil becoming trapped within hepatic metastasis reaching higher drug concentrations; they also suggested reserving the treatment with BCNU for patients who progress following immuno- and radioembolization. However, their outcomes did not reach those of Edelhauser et al. 27 Most authors of articles included used cisplatin-based therapy for TACE procedure, although high cisplatin doses are characterized by frequent systemic toxicity affecting patient outcomes. 40 In the studies we analyzed, TACE was performed on an average of 4 times per patient, and the best sustained response was obtained after a median number of 2 procedures. 21 Nowadays, chemotherapeutic agents employed for TACE remains a matter of debate and there is no clear consensus on which drug to use as first choice.
Uveal melanoma is a radiosensitive tumor and radiation therapies on liver metastases have been studied by different authors. The endovascular administration of 90Y microspheres into the hepatic artery allows the release of high radiation doses inside the tumor. TARE can be used as first-line or salvage therapy for metastatic uveal melanoma to the liver. The median administered activity was 1.8 GBq in first-line therapy versus 0.5-1 GBq in the salvage therapy. The median OS of TARE was 17 months in the studies we analyzed, confirming promising results. Ponti et al underlined the importance of surveillance programs in order to intercept metastases amenable to treatment. They also demonstrated how subsequent systemic and liver-directed therapies after TARE could improve the OS, showing synergistic abilities. 23 On the other hand, in our study the ORR of TARE was the lowest percentage among procedures. A possible explanation of this result is that radioembolization was mainly used as salvage therapies in patients with advanced metastatic disease and who, therefore, already had a poor prognosis before treatment. Gastrointestinal toxicity represents the main adverse effects after radioembolization and strongly correlates with mucosal damage induced by radiation; supportive therapies and close follow-up are strongly recommended for these patients.
PHP is a complex procedure involving a multidisciplinary team, and we have found to be performed in only a few centers. In our systematic review, the median OS and the PFS was respectively 15.3 and 8.4 months for PHP, while the ORR was the highest among the various therapies, confirming a good tumor control. Furthermore, PHP is the only of the discussed treatments that has a phase III randomized controlled study with stronger scientific evidence than retrospective studies, and it could be a valid option in patients who cannot benefit or in whom treatment with tebentafusp has failed.
In the studies analyzed, patients performed more than one PHP procedures between 6 and 10 weeks after the first treatment, improving the percentage of ORR for this therapy. Long et al retrospective analyzed patients underwent PHP focused on predictors of survival in their study. In particular, high serum lactate dehydrogenase (LDH) level at the baseline was an independent factor associated with worse survival, while primary tumor radiotherapy was associated with improved survival, suggesting that best candidates for PHP with melphalan as first-line therapy were fit patients with LDH < 2x upper limit of normal values. 22 In the same direction, Cornelia et al in a recent study on 66 patients suggested that the early treatment of uveal melanoma hepatic metastases responds better than patients receiving PHP after other previous treatments. Even if the aim of PHP procedure is to administrate melphalan directly to liver metastases with limited systemic exposure, hepatic and haematological toxicities are common, with the latter as the most common post-procedure adverse events found in our study. Several factors are related with this data. First of all, although the use of last-generation filter systems, residual amounts of melphalan associated with the leakage of the chemotherapeutic agents from the double-balloon catheter system could inevitably enter the systemic circulation. In addition, hepatocytes retention of chemotherapeutic agents might lead to late liver toxicity. 28 Among different studies, the peri-interventional mortality of PHP was 1%–4%, with serious cardiovascular and neurological complications described as life-threatening. Therefore, the various authors focusing on PHP agree on reserving such treatment for fit patients with good health status, no cardiovascular pathologies and with liver-only metastatic disease, excluding patients with extrahepatic disease. 58
TAIE is an emerging therapy in the treatment of metastatic uveal melanoma and the results of our study have demonstrated a median OS of 20.4 months and a PFS of 10.4 months, the latter representing the higher value among procedure analyzed. Our results are in accordance with those of Yamamoto et al and Valsecchi et al who compared chemoembolization to immunoembolization, demonstrating that high dose of GM-CSF increased the OS of patients compared to TACE; TAIE also resulted in a delay in the progression of the extrahepatic metastatic disease.43,44 Furthermore, high-dose of immunoembolization agent, younger age of patients and regression of hepatic metastases were identified as independent predictors of longer PFS, becoming important prognostic factors to take into account when planning treatment. These results were in agreement with those of Sato et al, who also identified a GM-CSF doses > 1500 µg as a threshold correlated to longer OS and PFS. 39
Ablation therapies were recently studied by different authors. Thermal therapies of liver metastasis from uveal melanoma are limited to patients with oligometastatic disease (< 3 metastatic lesions) or to patients with lesions not responding to embolization. 15 Compared to surgical resection, ablative therapies allow to spare healthier peritumoral tissue, reducing complication rate and treatment-related costs. Unfortunately, no large patient cohort studies analyzed clinical and technical success and outcomes in metastatic uveal melanoma and most results are fragmented. 18 The few data in the literature considered only small cohorts of less than ten patients and even if reached promising results, were excluded from the present study because did not meet inclusion criteria we established. The study of Eichler et al was the only one included in our review. They demonstrated how MR-guided laser-induced thermotherapy (LITT) could improve median overall survival and obtain a local tumor control without significant rate of complications and side effects. However, LITT requires dedicated instrumentation with elevated costs, and nowadays it represents a highly specialized therapy performed in only few hospitals.
In 24/26 (92.3%) studies analyzed, authors assessed the response to treatment using the Response Evaluation Criteria in Solid Tumors (RECIST version 1.0, 1.1 and/or modified RECIST). One month after completing the respective therapy, patients with UM were evaluated for treatment-related toxicity and disease progression. Radiological assessment for evaluation of tumor response was subsequently performed every 3 months with contrast-enhanced CT scans and/or gadolinium-enhanced abdominal MRI. Radiological imaging provides essential information about tumor control and treatment-related response and it is associated with superior survival of patients. 25 Furthermore, Carle et al and Valpione et al obtained a better ORR using mRECIST rather than RECIST 1.1, affirming the importance of radiological assessment based on viable tumor and not on changes in size alone.21,42
Uveal melanoma is a complex tumor characterized by poor prognosis in its metastatic form. Although different treatment options are available, there is no a clear consensus on which therapies should be performed as first line, second line, and so on. Different studies have demonstrated that minimally invasive liver-directed therapies have better outcomes prolonging overall survival and PFS when compared to systemic chemotherapy. However, recent researches have focused on the use of combined therapies, opening up new perspectives on further treatment possibilities. Surgical therapies combined with TACE or RFA were studied by different authors, obtaining interesting results in prolonging overall survival. Surgery could be also combined with other treatments such as TARE, TAIE, and isolated hepatic perfusion (IHP), additionally prolong survival of patients. Newer approaches were addressed on studying safety and efficacy of percutaneous liver-directed therapies, and in particular radioembolization, combined with targeted and immunotherapies, affirming the synergy of these therapies. Minor et al in a phase II multicenter clinical trial obtained a median overall survival of 26 months combining radioembolization with immunotherapy; the rational for this combination therapy is that radioembolization could create an immunogenic environment in the tumor strongly enhancing the efficacy of immunotherapy. 9 Shen et al studied cryoablation combined with transarterial infusion of pembrolizumab for the treatment of liver metastases from UM, reaching positive clinical results and a favorable safety profile. Ongoing clinical trials are investigating the optimal therapeutic strategy in patients affected by liver metastases from UM and the role of combination therapies has yet to be defined.59,60
To date, our work aims to be the first review analyzing large-scale studies on percutaneous liver-directed therapies of metastasis from uveal melanoma. Despite the poor prognosis of patients with metastatic UM, the use of minimally invasive therapies has implemented the therapeutic armamentarium available for this condition, achieving good outcome parameters in such a heterogeneous and aggressive neoplasm. The side effects of the various treatments must be kept in mind for proper management of their complications.
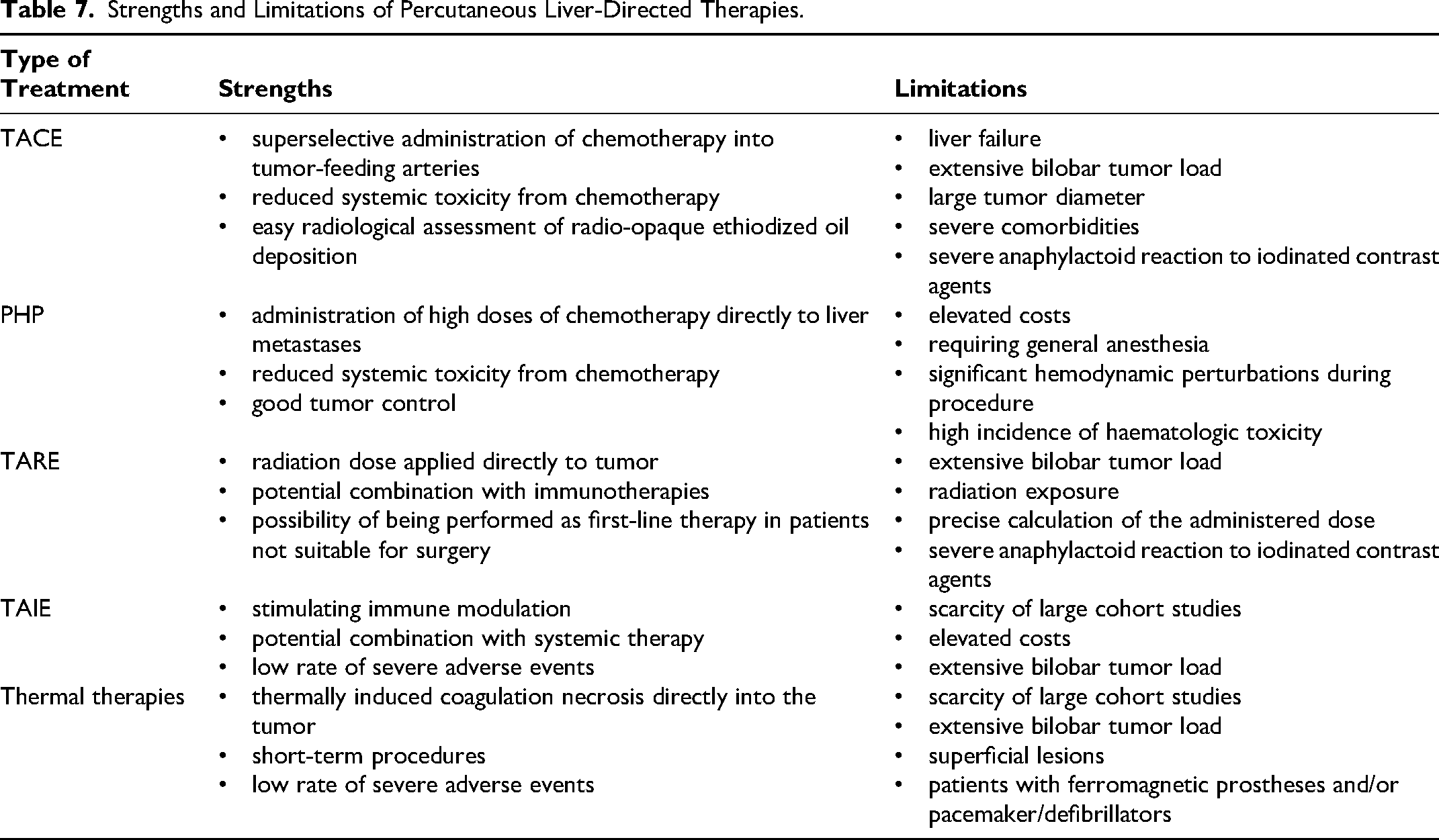
Potential strengths and limitations of each percutaneous liver-directed therapies reviewed in our study are summarized in the Table 7.
Strengths and Limitations of Percutaneous Liver-Directed Therapies.
Limitations and Future Perspectives
Our systematic review presents various limitations. First and foremost, the analysis of the articles included in the present review was mainly based on retrospective studies, making clinical and statistic data inhomogeneous. Furthermore, bias common to all retrospective studies and data extrapolated from “mixed” series (randomized controlled trials and non-randomized studies) represent an important limit in terms of the scientific evidence. Different studies screened did not meet eligibility criteria of our systematic review since analyzed mixed series of patients with both cutaneous and ocular melanoma, causing the loss of cohort of patients with uveal melanoma underwent locoregional therapies. However, extrapolating data from these patients was difficult and could lead to significant sampling errors and incorrect data outcomes, and were therefore excluded from our study. Different articles included in our research have examined a combination of different systemic and minimally-invasive locoregional therapies, representing a limit in evaluating single therapy outcomes and safety. Nevertheless, uveal melanoma is a tumor that requires a multidisciplinary approach and a combination of different therapies is often necessary to improve patient survival. In this perspective, long-term efficacy of these therapies and further combined treatment strategies need to be studied and developed.
In literature, different articles analyzed prognostic factors of uveal melanoma, but to date there are no correlation studies between the histologic type of uveal melanoma and the response to the individual locoregional therapies. 61 This could represent an interesting future perspective and require further studies on this topic.
Prognostic factors of UM recently studied were biohumoral markers, and in particular LDH and neutrophil to lymphocyte ratio (NLR); these biomarkers were used as a prognostic index to predict OS in patients with metastatic uveal melanoma receiving immunotherapy, giving important information about the effect of a particular therapeutic intervention. 62 Characterization of the metastatic risk of patients with UM is now possible through the analysis of genetic profile and tumor derived material in the circulating blood. Different biomarkers, such as circulating micro-RNA (cmiRNA), circulating tumor cells (CTCs), and circulating tumor DNA (ctDNA), were analyzed as minimally invasive prognostic tests to identify the risk of metastatic spread, to guide earlier therapeutic interventions, and to monitor high risk UM patients. 63 A novel marker, named PRAME (preferentially expressed antigen in melanoma), has recently been related to an increased risk of metastasis and to a shorter time to develop metastasis. The tumor microenvironment and specific genes play also a crucial role in the development of metastatic spread of UM, and novel therapeutic strategies need to be performed to improve the prognosis of patients with metastatic uveal melanoma. 64
In recent years, artificial intelligence is revolutionizing several medical fields. Different prediction models have been developed to predict the risk of distant metastases and types of treatment in various tumors, including uveal melanoma. In particular, machine learning algorithms extract large amounts of numerical data, integrating them into predictive models to improve and refine radiological diagnosis and clinical management of patients. In UM, these models could predict distant metastasis and facilitate personalized treatment strategies. In their study, Wu et al have developed a detailed model to predict distant metastasis in patient with UM using multilayer perceptron (MLP) machine learning model by using different data inputs (primary site of tumor, grade, diagnostic information, therapeutic strategies); they also introduced an online web calculator assessing the risk probability of metastatic spread to establish a clinical and therapeutic decision on metastatic patients. 65
Conclusions
The therapeutic management of metastatic uveal melanoma represents a crucial junction in the history of this neoplastic disease. Minimally-invasive locoregional therapeutic options are currently available for patients with metastatic uveal melanoma and different retrospective and prospective studies on percutaneous liver-directed therapies have resulted in an improving of outcomes parameters (OS, PFS, ORR). Studies on ImmTACs have recently provided an overall survival benefit in patients with metastatic uveal melanoma, and currently tebentafusp is approved for patients positive for HLA-A*02:01 leukocyte antigen.
The radiological response (CR and PR) of metastatic disease after locoregional treatment should be determined based on RECIST using cross-sectional imaging (CT and/or MRI), and it was associated with an increase survival of patients. Therefore, in all patients with metastatic uveal melanoma the treatment strategy and timing of follow-up should be personalized, and the management of this tumor requires a multidisciplinary approach. Haematologic and gastrointestinal toxicities were the main adverse effects associated with minimally invasive liver-directed therapies and these should be kept in mind when evaluating patients undergoing such treatments. To date, no official guidelines have established the superiority of one specific percutaneous locoregional treatment over another in patient with liver metastasis from uveal melanoma, and more prospective randomized studies are needed to determine the optimal treatment strategy among available therapies.
Footnotes
Abbreviations
Ethical Considerations and Informed Consent
The study did not directly involve humans and did not require the Institutional Review Board approval of our department.
Author Contributions
Corrado Ini': Conceptualization; Data curation; Resources; Formal analysis; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Pietro Valerio Foti: Conceptualization; Data curation; Resources; Formal analysis; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Renato Farina: Conceptualization; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Francesco Tiralongo: Conceptualization; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Davide Giuseppe Castiglione: Conceptualization; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Marta Cannarozzo: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Corrado Spatola: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Emanuele David: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Stefano Palmucci: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Andrea Russo: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Giuseppe Broggi: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Teresio Avitabile: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Antonio Basile: Conceptualization; Resources; Investigation; Methodology; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.