
Abstract
Male breast cancer (MBC), one of the rare types of cancer among men where the global incidence rate is 1.8% of all breast cancers cases with a yearly increase in a pace of 1.1%. Since the last 10 years, the incidence has been increased from 7.2% to 10.3% and the mortality rate was decreased from 11% to 3.8%. Nevertheless, the rate of diagnoses has been expected to be around 2.6% in the near future, still there is a great lack in studies to characterize the MBC including the developed countries. Based on our search, it is evidenced from the literature that the number of risk factors for the cause of MBC are significant, which includes the increase in age, family genetic history, mutations in specific genes due to various environmental impacts, hormonal imbalance and unregulated expression receptors for specific hormones of high levels of estrogen or androgen receptors compared to females. MBCs are broadly classified into ductal and lobular carcinomas with further sub-types, with some of the symptoms including a lump or swelling in the breast, redness of flaky skin in the breast, irritation and nipple discharge that is similar to the female breast cancer (FBC). The most common diagnostic tools currently in use are the ultrasound guided sonography, mammography, and biopsies. Treatment modalities for MBC include surgery, radiotherapy, chemotherapy, hormonal therapy, and targeted therapies. However, the guidelines followed for the diagnosis and treatment modalities of MBC are mostly based on FBC that is due to the lack of prospective studies related to MBC. However, there are distinct clinical and molecular features of MBC, it is a need to develop different clinical methods with more multinational approaches to help oncologist to improve care for MBC patients.
Introduction
Globally cancer is one of the leading non-communicable diseases and is responsible for a majority of death in both males and females. Therefore, it is considered as main barriers in increasing life expectancy and decreasing mortality worldwide.1,2 One of the globally identified most burdensome is the breast cancer (BC) and responsible for higher incidence of death in females. 3 Even though BC in male is rare/uncommon type of cancers, the global incidence rate is reported as 1.8% of all BC cases 4 with a yearly increase in a pace of 1.1%4‐8 where the incidence in Indian population is also similar to the global rate.9,10 Till the hormones influence the differentiation during the puberty, breast tissues in both male and female are identical. 11 Boys during their pubertal age will have increased level of estrogen along with a 30-fold increase in testosterone levels. Estrogen stimulation of the growth of breast tissue will normally be antagonized by the androgen in males. Hence, male breast is normally characterized as fat mass in sub-cutaneous area along with residue in sub-areolar tissues of the ductal region. 12
BC in men is one of the rare/uncommon forms of malignancy and is not fully understood. A unimodal peak at the age of 71 years reported in male based on age distribution in men with BC might be delayed diagnosis due to low suspicion 7 whereas, in women a bimodal distribution with peaks at 52 and 71 years of age were identified. 13 Identified risk factors for most of the BC cases in both sexes are unknown. Though comparative studies on the risk factors of BC in women and men are inadequate, certain factors like BRCA2 mutations had been ascertained to be a common risk factor for both sexes.
Male breast cancer (MBC) accounts for a small fraction of all BC cases and presents unique challenges in terms of prevention, early detection, and management. One of the key aspects in preventing MBC involves understanding the risk factors associated with its development. One of the major risk factors concerning MBC is the genetic predisposition, and is reported that inherited germline variants in BRCA1 and BRCA2 account for approximately 2% and 10% of MBC respectively with a life time risk in men harboring BRCA1 and BRCA2 mutations is 1.2% and 6.8%. 14 In light of this, genetic counseling and testing are strongly recommended for individuals with a family history of breast and ovarian cancers. 15 Cautious use or avoidance of estrogen-containing hormone replacement therapy is advisable for men with a history of conditions such as gynecomastia or other breast-related issues, as this can help in reducing the risk of MBC. 16 Moreover, promoting lifestyle modifications is crucial in MBC prevention. Encouraging men to maintain a healthy body weight, engage in regular physical activity, and limited alcohol consumption not only contributes to their overall well-being but also plays a role in lowering the risk of BC, mirroring the benefits observed in women's BC prevention strategies.
Early detection and screening are vital components in the management of MBC. It is imperative to educate men about the importance of self-awareness when it comes to their breast health. This includes encouraging them to perform regular breast self-examinations and promptly reporting any unusual findings to a healthcare provider. Additionally, routine clinical breast examinations by healthcare professionals play a crucial role in detecting MBC, particularly among individuals at higher risk. Even though mammography is considered to be a common screening tool for BC, it is reported that mammography in men is highly sensitive and specific, which might lead to high negative predictive value.17,18 Bearing in mind the limitations of using mammography to diagnose MBC, it is worthwhile to consider using appropriate diagnostic tool such as genetic counselling for men those with elevated risk factors, including family history of BC or known genetic mutations 19 for early detection and to increase the chances of treatment success.
The primary approach in managing MBC involves surgery encompassing mastectomy, which involves the complete removal of the breast, or breast-conserving surgery, depending on the need. Additionally, the management of MBC may entail to adjuvant therapies, which includes chemotherapy, radiation therapy, and hormone therapy, with the focus of reducing the risk of recurrence. The post-treatment phase of MBC is marked by a focus on follow-up and survivorship care. Regular follow-up examinations are essential to monitor for any signs of recurrence or potential complications arising from the treatment received. Additionally, emphasizing lifestyle management is vital in enhancing the overall well-being of MBC survivors. Furthermore, participation in cancer support groups or survivorship programs can offer MBC survivors an invaluable source of emotional support and a sense of community. These support networks provide a safe space for individuals to share experiences, exchange advice, and navigate the unique challenges that come with surviving MBC, fostering resilience and improving the quality of life for those on to the survivorship journey.
Epidemiology
The incidence of MBC will greatly differ with geographic areas and race.14,20 It is reported that in comparison to the Asian Countries, the frequency of MBC is much higher in the North America and Europe. 21 The epidemiology of MBC has changed significantly over the last 10 years. The American Cancer Society (ACS) reported that the estimated new cases of MBC in the year 2019 as 2670 with 18% mortality rate. 13 Subsequently it has been reported that rate of MBC diagnoses was expected to be around 2.6% in the year 2023 of all newly diagnosed cases with an estimation of 3200 men would be diagnosed and reported that the occurrence of MBC has been raised from 7.2% to 10.3% over the last 10 years and the mortality rate was decreased from 11% to 3.8%. 22 The incidence and 5-year survival rate of MBC in the last 20 years is depicted in Figure 1.

Incidence and 5-year survival rate of MBC in the last 20 years.
According to the SEER data, a significant raise in the rate of MBC, which exceeds at least 25% higher than that of women has been reported. 23 The ACS has predicted almost 2800 new cases in the United States with 530 deaths by the end of the year 2023. 24
Etiology
In spite of the increase in the global rate of MBC in the last 3 decades, 25 studies showing the etiology, prognosis, and treatment is seldom available, as most of the population-based studies and clinical trials focused on MBC is very limited. 26 However, guidelines for the treatment and clinical management for managing MBC are being used those which have been developed and followed based on female BC. The risk of BC in men increases with increasing age of an average between 60 and 70 years, with most cases happening in men over the age of 50 years old.22,27,28 The 5-year survival rate for MBC in India is estimated to be around 56%.29‐32 Even though there are no solid evidences stating the mechanism of MBC, some reports have reported that MBC are more likely to express high levels of either estrogen receptors (ERs) or androgen receptors compared to female with a minimal or no expression of HER2.7,23,33
Identified risk factors for the cause of MBC are familial history, radiation exposure of the chest in the past, engorged breasts, exposure to estrogen, overweight, inherited gene mutation (BRCA1 and BRCA2), and certain medical conditions, including cirrhosis, obesity, Klinefelter syndrome, and so on, may increase the risk. Moreover, certain lifestyle behaviors, such as smoking, over consumption of alcohol, and less or no physical activities could also increase the chances of developing MBC. Men diagnosed with BC typically present with a lump in the breast or nipple discharge and may also include rash, itching, or pain in the breast area.29,34
Risk Factors
As like female BC, factors including genetic, endocrine compounds, and other environmental risk factors are considered as the major risk factors that can cause MBC. The known risk factors for the cause of MBC are given in Figure 2. A recent review by Fentiman has reported that BRCA2 mutation carriers and individuals with Klinefelter's syndrome are the 2 significant cohorts responsible for up to 15% of MBC cases. 35 Moreover, the risk of BC increases at least 2-fold in case of family history and it can be considered as the main predisposing factor. 10 Considering the epidemiological prospective, BC in men most closely resembles the BC in post-menopausal women but the clinical and pathological characteristics are different from each other. Additionally, BC in men has poor prognosis in comparison with female breast cancer (FBC) because of the symptoms appear in unconventional stage in men,36‐39 where the scenario remains to be the same even decades. Hence, the increase in age is directly proportional to the risk of BC.

Risk factors of MBC.
Role of Lifestyle Factors, Diet, and Exercise
Several studies have highlighted the role of lifestyle and environmental elements in influencing the onset and advancement of the disease.40‐44 Among the risk factors, obesity through the hormonal mechanisms emerge as particularly noteworthy due to their potential causal connection with BC and the feasibility of modification.35,43 Further the studies have also stated that dietary factors, physical activities, and socio-economic status could also deserve for the cause of MBC.35,43 It is advised to limit saturated fats derived from red and processed meats, full-fat dairy products, and fried foods, as their high consumption is associated with an elevated risk of BC. 45 Furthermore, added sugars and processed foods, which are crucial to contribute towards weight gain and inflammation, are recognized risk factors for BC. 46 Additionally, excessive intake of alcohol is also linked to increased risk of BC. 47
Several studies have reported that eating more dietary fiber from various sources including whole grains, pulses, vegetables, and fruits can supply essential nutrients and antioxidants that bolster overall health and not only reduce the risk of BC in men but also improve the overall survival (OS) rate.48‐51 Incorporation of a diverse array of colors with a wide spectrum of essential nutrients could ensure prevention of BC. 52 Lean proteins sourced from poultry, fish, beans, lentils, and tofu provide essential amino acids necessary for cellular repair and maintenance. 53 Healthy fats, consumed from avocados, nuts, seeds, and olive oil, support overall well-being and help in reducing inflammation. 54 Omega-3 fatty acids, found in fatty fish like salmon, mackerel, and chia seeds, possess anti-inflammatory properties that may confer protection against BC. 55 Antioxidant-rich foods like berries, nuts, and dark leafy greens play a crucial role in neutralizing harmful free radicals in the body. 56
Green tea, containing compounds such as catechins, has been studied for its potential protective effects against BC. 57 Turmeric and curcumin, known for their anti-inflammatory and antioxidant properties, may also offer some protective benefits. 58 It is reported that compared to the omega-6 arachidonic acid, marine omega-3 fatty acids such as eicosapentaenoic acid and docosahexaenoic acid have demonstrated a lower associated risk of BC. Regular exercise is also crucial in this context. 59
Recent study has demonstrated the significance of heightened lipogenesis in facilitating the self-renewal and proliferation of BC stem cells. 60 Furthermore, it highlighted the efficacy of omega-3 fatty acids through targeting the site-specific pathways to exert their anticancer properties. 60 It is also reported that the combination of hydroxytyrosol, omega-3 fatty acids, and curcumin effectively alleviated inflammation, which is evidenced by a decrease in CRP levels, and furthermore the reduction in pain among patients experiencing aromatase-induced musculoskeletal symptoms. 61 Flaxseeds, abundant in fiber, are recommended for improving constipation as they aid in enhancing intestinal function, additionally, they contain omega-3 fatty acids. It is also reported that flaxseed either enhanced or sustained tamoxifen's effectiveness in reducing tumor growth through inhibiting cell proliferation and promoting apoptosis. 62
However, several studies have reported due to the germline mutations in the onco-suppressor genes such as BRCA2, p53, ATM, CHEK2, and PALB2, almost around 10% of the cases are hereditary in nature. More specifically it has been reported that mutation in PALB2 gene has at least 8-fold increased risk of developing MBC.63‐67 As reported above, Kaur et al, in the year 2019 revealed 13 novel missense mutations in 8 genes in MBC patients from Malwa region of Panjab, India. 68 Genetic profiling of men could be helpful via identification of genetic markers; those which are associated with MBC patients can be helpful in paving way for newer therapeutic strategies and furthermore to design site-specific agents.69,70 Table 1 shows the various genes and proteins that are more prone for mutation and their functions in MBC.
Genes and Proteins That are More Prone for Mutation and Their Functions in Male Breast Cancer.

The other risk factors include, exposure to estrogen as hormone therapy for prostate cancer; Klinefelter's syndrome, a genetic syndrome, which causes abnormal development of the testicles that produce lower levels of certain male hormones such as androgens and more levels of estrogen, a female hormone. Inflamed testicles (Orchitis) or removal of testicles (Orchiectomy) might also increase the risk of MBC. Certain medical conditions such as hormonal imbalance due to any liver diseases and obesity could also increase the risk of MBC.89,90 In addition to the above-mentioned risk factors, quite a few more that are related to occupational hazards such as hot working environments, working with chemical and hormonal synthetics, long-term exposure of ionizing radiations and electro-magnetic radiation and chemicals and its’ combustion products are also reported to increase the risk of developing MBC.91‐93
Types
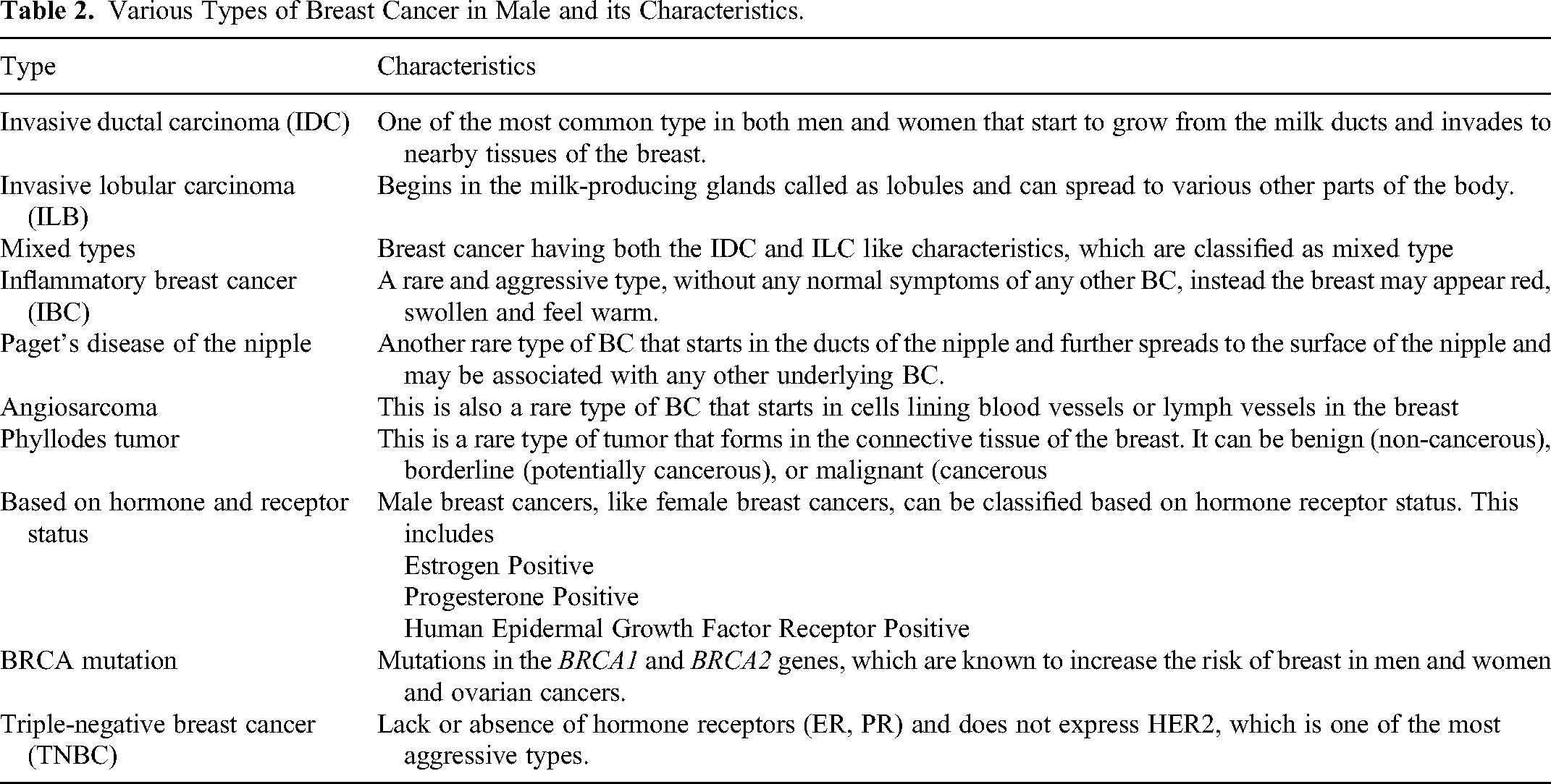
There are several types and subtypes of MBC classified based on various factors including histology, hormone receptor status, and genetic mutations. Various types of MBC and its characteristics are summarized in Table 2.
Various Types of Breast Cancer in Male and its Characteristics.
Ductal Carcinoma In Situ (DCIS)
DCIS in the breast is identified by a lesion confined within the breast ducts, devoid of invasive traits or metastatic potential. Pure DCIS comprises approximately 10% of all MBCs and constitutes less than 0.1% of all cancer types in men. Ensuring a prompt diagnosis of male carcinoma in situ and implementing effective clinical interventions are pivotal in averting its advancement into a more severe form, like invasive carcinoma. 94 It constitutes roughly 1% of all malignancies in men and accounts for 5% to 7% of MBC cases. 95
However, studies have reported that as like in women, majority of men have invasive ductal caricnomas,96‐98 which constitutes about 90% of all MBCs. 99 However, medullary, papilloma, and lobular are also implicated to be the other types. In spite of the low level of knowledge and awareness and stigmas towards MBC, in-situ ductal carcinoma is found desperately, which leads to delayed diagnosis and poorer patient outcomes. Approximately 90% of MBC expresses ER, and 81% expresses progesterone receptor (PR).100‐102 Comparatively papillary carcinoma is one of the most prevalent types and lobular carcinomas are rare. 103 However, a recent study by Chhabra et al, in the year 2021, showed around 81% of ER, 76% PR, 25% HER2neu, and 2% of TNBC in Indian population. 29 It is also reported that hormone receptor expression is more common in MBC when compared with FBC. 92 Hence, inhibition of these receptors could be usually predicted for the treatment and management of MBC, which will be discussed under the treatment modalities in the further sections.
Signs and Symptoms
MBC also shows some of the most common symptoms of FBC such as painless subareolar lump in the breast, nipple retraction called as flattening, nipple inversion where the nipple seems growing inward, fluid discharge from the nipple, redness or scaling of the nipple or breast skin.104‐106 It is also evidenced that there would be a single preponderance of left-sided versus right-sided disease similar to women. 106 Deficiency of established screening guidelines for MBC is directly reflecting on the delayed diagnosis of the disease. International Male Breast Cancer Program has reported that approximately 46.7% of men with this disease are reported to have at least one lymphnode at the time of diagnosis. 33 Chances of treatment success could be increased with early detection of the disease.
Secondary Malignancies due to BC
Development of the secondary malignancies due to MBC has increased risk of generalized malignancy in a secondary spot. A retrospective registry-based cohort study conducted at the UC Irvine by involving data from the year 1988 to 2023 with 1926 men aged 85 years or less diagnosed with primary BC. Out of the 1926 patients, 221 (11.5%) patients have developed a secondary cancer. 107 The development of second cancer is reported to be more particularly of a 2nd primary cancer of the breast, cutaneous melanoma, and stomach cancer compared with general population. However, younger men are more prone or at high risk of developing second malignancies. An earlier study had reported that 17% of MBC patients have developed prostate cancer out of the total 69 MBC cases identified.107,108 This might be due to the use of aromatase inhibitor (AI) to treat MBC, which could increase the serum testosterone levels and could enable the growth and proliferation of prostate cancer clones. 109 It is also reported that the other frequent secondary spot for the development of cancer in MBC patients are leukemia, pancreas, small intestine, and rectum.104,110
Diagnosis
Studies have reported that lack of knowledge and awareness of the disease and delay in diagnosis are the major reasons that usually BC in men are diagnosed at later stages that would pave way for the overall poorer prognosis.111,112 Recommendation from the American College of Radiology strongly suggests the bilateral ultrasound evaluation for younger aged men (<25 years) with palpable mass, whereas bilateral mammography for men older than 25 years of old. 113 On identification of any lumps or suspicious area in the breast, complete family history with physical examination may lead for distinguishing the BC and to choose the better choice of diagnosis and treatment modalities. Evidences of lumps or suspicious areas with any further possible spread especially the enlarged lymph nodes under the arm by felling the texture, size, and its relationship to the skin and muscle could be diagnosed by complete breast physical examination. Irregular, hypoechoic retro-areolar masses with variable vascularity are some of the most common finding on the ultrasound evaluation whereas similar speculated and radio-dense irregular retro-areolar masses on mammography. 114 Mammograms in diagnosing MBC were reported to have 92% to 100% sensitivity and 90% to 96% of specificity. 19
Additionally, various breast biopsy methods such as fine needle aspiration (FNA) to differentiate malignant from non-malignant type of breast disease in men, 115 core needle biopsy (CNB), surgical biopsy, and lymph node biopsy can also be employed. However, identification of specific markers those associated with MBC via., molecular profiling could pave way to discover and/or identify newer therapeutic strategies. Chatterji et al have systematically reviewed the existing prognostic MBC marker data for a period of 29 years and reported that consolidated all existing prognostic biomarker data in MBC spanning genetics, transcriptomics, proteomics, and epigenetics, and phenotypic features of prognostic value from articles published over a 29-year period (March 16, 1992, to May 1, 2021). 116 Additionally, they also reported 4 epigenetics-based clusters from the relative promoter hypermethylation levels of RASSF1A, GSTP1, WIF1, RARB, and MAL. Notably, cluster 3 associated with mutated BRCA2. The authors have also reported that a subgroup analysis on BRCA2-mutated MBCs can be separated into 2 clusters based on the hypermethylation levels of GSTP1, MAL, and RASSF1A. 116
A new horizon in understanding of cancer biology has been attained with the multi-omics molecular characterization of cancer. Despite, a major confounding factor that hampers a vigorous and reproducible tool involving bioinformatic analysis is that the diverse types of cells which are not only limited to the cancerous cells but also to the tumor microenvironmental cells those are adjacent to the normal cells could also present in biopsy of any tumor. 117
Turajlic et al have reported that a snapshot of the genetic landscape of most of the cancer types could be determined using the next-generation sequencing with an insight of the cancer genomics approach which could emerge newer evolutionary patterns. 118 The authors have also stated that an evolutionary framework could be a powerful tool to understand not only the cancer progression and/or the treatment failure but also could be a predictive tool to assess the tumor behavior and strategize treatment support. 118 Similarly, Siavoshi et al have also reported that analysis of multiple gene differential expression profile datasets by using Gene Ontology (GO) and Kyot Encyclopedia of Genes and Genomes (KEGG) for protein–protein interaction (PPI) network analysis could be used to define the hub genes. 119 Furthermore, the authors have also stated that Gene Expression Profiling Interactive Analysis (GEPIA) could be used to determine the relative mRNA expression of the hub gene, and thereby a prognostic gene signature can be identified. 119
Hence, in the current review we have sought the PPIs of 20 different proteins that play major role in MBC which has been sorted out based on the STRING mapping (Figure 3).

Protein–protein interaction of all 20 proteins in MBC using STRING.
It is clearly evident that BRCA2, BRCA1, and PALB2 form a complex involved in exchanging DNA strands during DNA repair. CHEK2 and PTEN collaborate in suppressing tumor growth through their regulation of the PI3K-Akt signaling pathway. TP53 and RAD51C work together in DNA repair and apoptosis. RAD51D, NBN, and ATM are all involved in the homologous recombination process of DNA repair. STK11 and CDH1 regulate the Hippo signaling pathway and regulate cell growth and apoptosis. MRE11A, MLH1, MSH2, and MSH6 form the MutL complex and control DNA mismatch repair. PPM1D and RAD51 form a complex and function in the DNA damage response. RAD50 and BARD1 work together in DNA repair by coordinating single-stranded breaks.
Treatment Modalities
Owing limited information available regarding the treatment options for men diagnosed with MBC, currently the treatment strategies for MBC are mostly based on the FBC guidelines.117,120 Even though the disease characteristics are similar to FBC, with the understanding of the distinct clinical features, treatment strategies for MBC require a specific clinical approach. 121 Therefore, in the recent years involving men in BC clinical trials are growing. Several studies have reported that OS of MBC is comparatively lower than FBC.122‐124 In contrast to the above studies, it is also reported that on comparison with women, men have a slightly better or equivalent disease-specific survival.125,126
Various modalities those are currently being practiced for the treatment of MBC have been shown in Figure 4.

Treatment modalities for the MBC patients.
Based on search of literature, the treatment for early stage or non-metastatic MBCs includes the following127‐130:
Surgery Radiation therapy Chemotherapy Hormonal therapy Modified radical mastectomy Axillary lymph node dissection Sentinel node biopsy
Earlier, Scott-Conner
106
and his colleagues have also reported that men with BC would also be treated with:
Beside which, the other options may include breast conservation or nipple-sparing of skin-sparing mastectomies. With respect to the limited number of studies and data for the use of chemotherapy to treat MBC, clinicians would prefer to assess the typical factors that has similar features of the FBC with early-stage of the disease.
121
With large tumors or nodal involvement and if BCS is anticipated, neoadjuvant therapy could be employed to reduce the tumor size for the feasibility of BCS.
131
Modified radical mastectomy is one of the most chosen surgical treatment for MBCs despite of radical mastectomy, where some of the less favored approaches including total mastectomy, and lumpectomy with or without radiation especially in patients of older age. 132 Recently, a large population-cohort study evaluated the data of 16,498 MBCs from the National Cancer Database and has reported that treatments involving surgical methods showed an improved rate of survival. 133 Oppositely, Yadav et al have reported a negative association with mastectomy. 134 However, both the studies have also reported that increase in age, black ethnicity, government insurance, accumulated comorbidities and later stage with high grade tumors were highly associated with worse prognosis and decreased survival.133,134 Despite, Yadav et al have reported that comparatively more male patients have underwent total mastectomy rather breast-conserving treatment, which is the most preferred option for female patients undergoing surgical treatment. 134 Moreover, 2 different studies from a European and USA Center have stated that sentinel lymph node biopsy is a reliable tool for the identification of nodal metastases.135,136 Considering that there is no strong evidence available for the use of radiation after mastectomy, adhering the guidelines for FBC is the current recommendations as shown in few of the single institutional experiences.137,138
Owing that hormonal therapy (HT) is considered to be the gold standard treatment option for hormone receptor positive in MBC, tamoxifen is characterized as adjuvant HT for 5 years which is associated to reduced risk of recurrence, representing by 51% in comparison to the treatment of FBC. 139 Aromatase pathway is responsible for about 80% of the total estrogen produced in male and 20% of which is produced by the testes. 140 Inhibiting the aromatase pathway that is responsible for the major production of estrogen could be one of the right choices of MBC treatment. However, studies focusing the role of adjuvant AIs in male patients is very limited. 141 A study by Eggermann et al has compared the adjuvant tamoxifen versus AIs and reported that the outcome in AI cohort was statistically not significant for both mortality risk and OS. 142 In general adjuvant chemotherapy could also be recommended on considering the age, high tumor grade, and/or the involvement of axillary nodes. However, it is also reported that adjuvant chemotherapy showed a statistically not significant results while considering lower time to recurrence and improvement of OS. 139 Based on literature search and the best of our knowledge, there is no data available related to the adjuvant use of trastuzumab in MBC treatment expect one case report with the speculation of its efficacy in metastatic disease. 143 The authors have also anticipated there is no specific biological reason for showing different activity of trastuzumab in MBC than in FBC, the use of trastuzumab and pertuzumab might be considered for treating HER-2-positive MBC. 143
In view of the greater number of MBC patients have hormone receptor positive, endocrine therapy using tamoxifen could be considered as first-line of choice while choosing the treatment option for the MBC patients. 144 AI could be used in combination with gonadotropin releasing hormone where the disease is progressed even after with tamoxifen treatment. 145 Recent studies have also emphasized a partial response with the use of selective ER degrader fulvestrant for the treatment of MBC.102,146,147 Agents targeting endocrine and other specific targets such as mTOR and CDK and its combinations are also suggested in treating MBC patients. The same chemotherapeutic agents and regimens that are being used to treat FBC could be used for metastatic MBC treatment.92,113,117,148
Targeted Treatments: Precision Medicine in MBC
The advent of targeted therapies marks a significant stride in the field of oncology. Yang et al has reported that, Epirubicin (EPI), upon entering the BC cells under the guidance of the targeting NKA-α1 peptide, exhibited a gradual release from the nanocarrier. 149 The controlled delivery and subsequent release of EPI within the BC cells resulted in significant inhibition of cell proliferation and migration in vitro and led to a substantial reduction in tumor volume in vivo. 149 The introduction of lumpectomy as a treatment for BC marked a significant advancement in disease management. Onik in 2004 has suggested that a procedure akin to a “male lumpectomy”—one that precisely targets the cancerous portion of the prostate gland while minimizing patient morbidity—is indeed feasible. 150 The authors have also stated that at a time when patients are faced with the choice between “watchful waiting” or potentially high-morbidity whole-gland treatments, such a focal approach would be a highly welcomed addition to the treatment options available. 150 Overall, the well-being and quality of life of individual patients could be successfully integrated into the general approach to cancer treatment, all while maintaining treatment efficacy.
Immunotherapies: Unleashing the Immune System Against MBC
Immunotherapies have revolutionized cancer treatment by harnessing the body's immune system to recognize and eliminate malignant cells. 151 This approach has yielded extraordinary outcomes across various malignancies, prompting exploration in the realm of MBC. Immune checkpoint inhibitors (ICPIs), a class of immunotherapeutic agents, have shown potential in enhancing immune response against cancer cells. Recent trials investigating the efficacy of ICPIs in MBC have demonstrated encouraging results, warranting further investigation into their role as a viable treatment option.152,153 Combination therapies involving immunomodulatory agents, such as ICPIs with targeted treatments, have also emerged as a promising avenue. Studies have indicated synergistic effects, underscoring the potential of a multifaceted therapeutic approach in MBC.154,155
Biomarker-Driven Patient Categorization: Paving the Way for Personalized Therapy
The identification of specific biomarkers holds paramount importance in tailoring treatment strategies for MBC. Biomarkers serve as critical indicators, guiding therapeutic decisions and enabling a more personalized approach to patient care. Genomic profiling has emerged as a powerful tool in characterizing the molecular landscape of MBC. Studies have identified distinct genomic alterations in MBC, highlighting potential targets for therapy.156,157 Moreover, the integration of liquid biopsies for the detection of circulating tumor DNA (ctDNA) has shown promise in monitoring disease progression and identifying actionable mutations in MBC.158,159 This non-invasive approach offers a valuable avenue for real-time monitoring and treatment adjustment.
One promising avenue in targeted therapy for MBC involves the inhibition of hormonal receptors. ER positive MBC, though less common in men than women, represents a significant subset. Recent studies have highlighted the effectiveness of anti-estrogen agents like tamoxifen and AIs in male patients, emphasizing the importance of tailored hormonal therapies.160‐162 HER2-targeted therapies have shown remarkable success in HER2-positive BC cases. Although less prevalent in MBC, the presence of HER2 amplification necessitates targeted intervention. Studies exploring the efficacy of anti-HER2 agents like trastuzumab have demonstrated promising results in male patients, underlining the importance of targeted treatments in specific molecular contexts.163,164
Understanding the unique challenges and experiences faced by men with BC can lead to more effective and tailored treatment strategies. Some of the few key points that could be considered in such analysis have been summarized in Table 3.
Comparison Table for the Disease Progression, Treatment Responses, and Quality of Life in Male and Female Breast Cancer.

Future Directions
Men with BC have an increased risk of developing secondary malignancies, such as secondary primary BC, cutaneous melanoma, stomach cancer, leukemia, and prostate cancer. The use of AIs to treat MBC may contribute to the development of prostate cancer. Diagnosis of MBC involves a complete family history, physical examination, bilateral ultrasound evaluation for younger men, and mammography as well. Biopsy methods, including FNA, CNB, surgical biopsy, and lymph node biopsy, can help in diagnosing the disease. Screening guidelines for MBC are not well established, leading to late-stage diagnosis and poorer outcomes. Implementation of proper guidelines for MBC and early detection can improve treatment success.
Conclusion
In conclusion, MBC is a rare but increasingly diagnosed condition. The current study emphasizes the urgent need for increased awareness and understanding of BC in men. The identified risk factors, including genetic predisposition, environmental exposures, occupational hazards, and lifestyle factors, highlight the complex nature of MBC etiology has been comprehensively reviewed. Even though the diagnosis and treatment modalities for MBC encompass a range of options, the comparison shows that the guidelines for MBC largely rely on those developed for FBC. It is clear that even with the adjusted differences in patients’ clinical characteristics, the death rate in men is higher than in women across all stages of BC. Hence, there is a need for prospective studies specifically focused on MBC to provide more tailored approaches. Hence, there is an immediate need to develop different clinical methods with a multinational approach to further improve the care of MBC patients. Strategic studies aiming to identify novel biomarkers specific to MBC and advancements in targeted treatments hold the potential to improve outcomes and save lives. It is important to raise awareness, improve knowledge, and develop tailored strategies for the prevention, early detection, and treatment regimens for MBC.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.