
Abstract
Introduction
Volumetric modulated arc therapy (VMAT) has been widely employed for linear accelerator-based stereotactic body radiotherapy (SBRT) with high targeting accuracy facilitating complete eradication of tumors and protection of surrounding normal tissue due to its ability to deliver high doses to the target in a few fractions. 1 Due to its fast treatment time and lack of requirement for table movement, VMAT-SBRT can greatly shorten treatment time and improve the patient's experience. In recent years, the VMAT-SBRT technique has been used for multiple brain metastases, multiple lung metastases, and multiple liver metastases (MLMs). Clark et al 2 used the RapidArc technique to treat patients with 3-target brain metastases, including single-isocenter or third-isocenter configurations and showed that the single-isocenter VMAT protocol provides comparable consistency to the multiisocenter VMAT technique. Timmeren et al 3 conducted a dosimetry study using the single-isocenter and multiisocenter techniques in multiple lung metastases, and reported that the single-isocenter SBRT technique for lung patients with multiple targets results in clinically acceptable increases in normal lung dose. Our previous research 4 comprehensively evaluated the quality of single- and multiisocenter VMAT-SBRT for MLM and proposed a RapidPlan-based automatic planning (AP) approach for MLM SBRT. Compared with the manual plans, they concluded that AP-based plans have slightly improved quality, and the single-isocenter VMAT-SBRT approach could be used for MLM to reduce treatment time and patient comfort at the cost of a small increase in the mean liver dose.
However, many studies have shown that the target position accuracy has a greater impact on dose coverage in single-isocenter therapy than in multiisocenter therapy because the dose drops quickly outside of the target area and the distance between the planned isocenter and other target centers may be different.5–7 Some studies have simulated rotational errors for multiple brain targets and found that rotational setup errors should be evaluated carefully for clinical cases involving different isocenter distances and tumor sizes.8–11 Kyle et al 12 showed that high-dose liver SBRT is safe and effective in a multiinstitution study of the treatment of patients with 1 to 3 hepatic metastases. However, organ motion is a challenge in liver SBRT. Other studies have evaluated the dosimetric effects of baseline shifts on target areas and organs when using respiratory gating therapy. By simulating varying phase shifts of internal and external respiratory signals, Korreman et al 13 accounted for changes in respiratory baseline movements and the corresponding internal and external movements to reduce the margin of respiratory-gated radiotherapy. Schmidt et al investigated the dosimetric impact of tumor motion and anatomical changes during intensity-modulated radiotherapy of patients with nonsmall cell lung cancer. The applied margins require consideration of anatomical changes and respiratory baseline shifts. 14 To manage the uncertainty of target positions, active breathing control, deep inspiration voluntary breath-hold, abdominal compression, four-dimensional computed tomography (4DCT), and respiratory gating techniques have been implemented.15–20 Among them, 4DCT-guided gated therapy combines a couch with six degrees of freedom for position correction to allow for accurate and comfortable treatment of patients.21,22
The influence of respiratory baseline shifts is an important consideration for target dose coverage, especially for the 4DCT-guided gated-single-isocenter therapy technique for multiple-target liver SBRT. This involves monitoring the patient's respiratory cycle during the CT scans, and the movement of tumors in the liver can be tracked in the positioning images. 23 The influence of respiratory movement can be accurately compensated for when internal target volume (ITV), thus reducing the irradiated area. 20 Radiation emission is controlled by breathing time fusion control technology, which can further narrow the area of treatment and reduce radiation exposure to normal liver tissue. However, dose delivery without traversing the respiratory full-time phase has its limitations. Wang et al and Ruggieri et al conducted studies on SBRT treatment of brain metastases and showed that extending the treatment time would increase the position error, resulting in reduced accuracy of dose delivery.7,24 Therefore, to balance the factors of intrafractional tumor movement and dose transmission time, full-time phase or single-time phase treatment is not preferred, and usually, a 2 to 4-time phase is used.
Single-isocenter VMAT-SBRT improves treatment efficiency and patient compliance for patients with MLMs. However, to our knowledge, there have been no studies investigating the dosimetric effects of baseline shifts coupled with rotation errors in MLMs treated with single-isocenter VMAT-SBRT. Therefore, the purpose of this study is to investigate the dosimetric effects of baseline shifts combined with rotational error on single-isocenter, MLMs treated with 4DCT-guided gated SBRT. A retrospective multivariate analysis characterizes target coverage as a function of target size, distance from the point of rotation, the degree of rotational error, and the shift of baseline.
Materials and Methods
CT Simulation and Treatment Planning
Ten anonymized patients, each with 2 or 3 liver lesions, were selected retrospectively from our radiotherapy center, with approval from the institutional review board and ethics committee of Jiangxi Cancer Hospital (2023ky194). GE medical systems were used to acquire real-time position management (RPM) based 2.5 mm thick CT image slices with 10 respiratory phases (CT0, CT1, CT2, …, CT9) and transfer it to Eclipse (Version 15.5) treatment plan system (TPS). The gross tumor volumes (GTVs) were contoured on 4DCT by one senior radiation oncologist according to international guidelines. 25 The ITV encompassing the whole respiratory tumor motion area was generated on the union of GTVs, and the final planning target volume (PTV) was generated by uniformly expanding ITV with a 5 mm margin. Critical structures including the normal liver, heart, spinal cord, and kidneys were also contoured. The PTVs and the distance between PTV centroids were recorded for each case. Table 1 lists the detailed clinical characteristics of these patients.
Characteristics of the 10 Cases With Liver Metastases Enrolled in This Study.
Abbreviation: PTV, planning target volume.
Average intensity projections of image sets of 4DCT images were generated for dose calculation. Plans were created in Eclipse TPS (Version 15.5.12), and Acuros XB (Version 15.5.12) dose algorithm with a single isocenter technique, and the isocenter was placed at the centroid of all lesions. All treatment planning was conducted by one senior physicist who was experienced in liver SBRT plans, with review from other senior physicists. The prescribed dose was 40 Gy in 5 fractions. The VMAT-SBST plan was generated by 2 coplanar full arcs with the collimator angle set to 30°and 330°; couch angle of 0°; and jaw tracking was activated in the process of optimization to reduce multileaf collimator transmission or leakage based on island blocking principles. 26 The prescribed dose for each target volume is 40Gy, covering > 95% of each target volume, while also keeping the maximum PTV dose > 120% of the prescription dose. A 1.25 mm dose calculation grid was used. The organ-specific penalties and normal tissue objective function were used optimization to further spare normal tissue. The mean dose of liver-GTVs (Entire liver tissue minus the GTVs) was below 15 Gy, and the volume of liver-GTVs that received 17 Gy at most was above 700 cc.
In this research, we adhered to the STROBE guidelines as outlined in the Equator Network to ensure transparency and quality. 27
Motion Study
The models of baseline shifts and rotational errors were simulated about the plan isocenter using the Cartesian coordinate system, and all isocenter adjustments were made solely using the Eclipse TPS. For rotational errors, the rotation was measured around the x-axis by an angle α, around the y-axis by an angle β, and around the z-axis by an angle γ to displacement Pr (Xr, Yr, Zr) as shown in Equation (1).
28
The rotational errors ranged between 0° and 1.5°.

Evaluation of Dosimetric Indices
The percent isodose line relative to the prescription dose that covers 95% of the PTV (PTV D95) and the volume of the PTV covered by 95% of the prescription dose (PTV V95) were recorded for each target and distance of baseline shifts and degree of rotation. The values of D95 and V95 were calculated on the mean CT phase set in Eclipse using the same parameters as in the original VMAT-SBRT plan. The D95 and V95 values from Eclipse TPS were evaluated using generalized estimating equations (GEE) statistical analysis to assess their reliability and consistency.29,30 PTVs coverage rates were analyzed according to the corresponding target volume and the distance to the isocenter. The intrapatient correlations were accounted for by GEEs (eg, dosimetric cross-talk among closely adjacent PTVs). The effects of volume and distance on D95, at rotations of 0.5°, 1.0°, and 2.0°, and baseline shifts of 0.5, 1.0, and 2.0 mm, were characterized by multivariate linear regression
31
:

Statistics
Parameter estimates, P-values, and CIs were calculated. The identity link of the normally distributed data was evaluated using the Kolmogorov-type supremum test, which simulated the cumulative sum of residuals to assess goodness-of-fit. 32 The analysis was performed using IBM SPSS Statistics 20, and P-values of less than .05 were considered to be statistically significant.
Results
Across the 10 cases and 22 lesions studied, the median and range of PTV volumes were 18.5 cc [4.15-85.93], and the mean and standard deviation were 24.5 ± 20.3 cc. Distances from each PTV centroid to the plan isocenter varied from a relatively small separation of 1.15 to 9.32 cm, with a median value of 6.8 cm. The mean and standard deviation were 6.2 ± 2.5 cm. Patient characteristics are displayed in Table 1.
In addition to the original 10 plans, each with 2 or 3 PTVs, an additional 15 simulated plans were generated by coupling baseline shifts with rotational errors. Target coverage was characterized by combinations of uniform baseline shift errors of 0.5, 1.0, 2.0 mm, and rotations of 0.5°, 1.0°, and 1.5° about all axes. D95 and V95 values are plotted as a function of the distance to isocenter in Figure 1. Coverage worsened substantially when the baseline shift errors were increased to 1.0 mm. D95 and V95 values were >95% for 77.3% of the targets, with approximately 11% of the targets falling below 90%. The D95 and V95 values were >95% in only 11.4% of cases when the baseline shift errors were increased to 2.0 mm. Figure 2 shows the values of D100 and V100 of GTV, respectively, which are plotted as a function of the distance to the isocenter. They show the same trend, ie, coverage deteriorating as baseline shift and rotation errors increase.
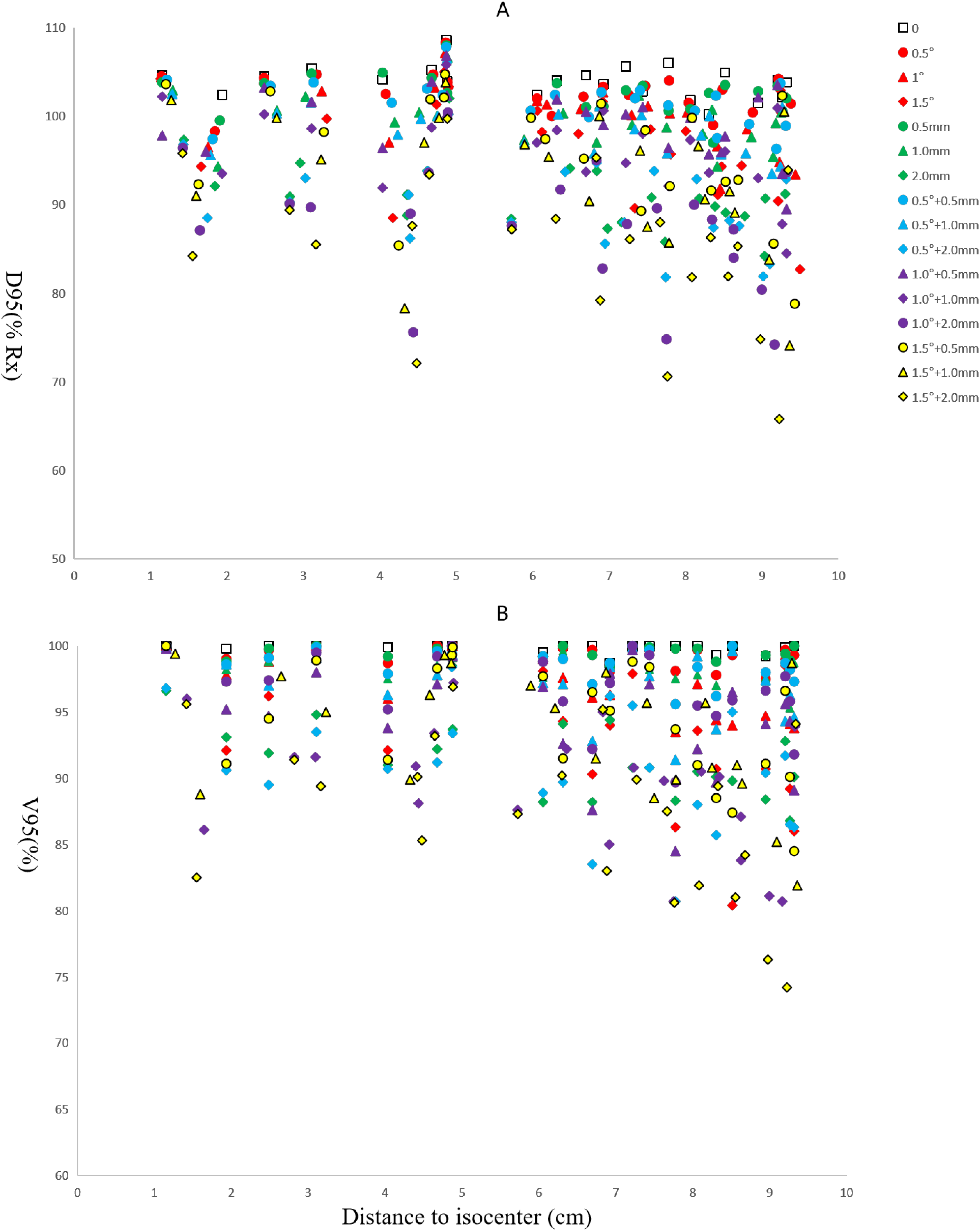
D95 (A) and V95 (B) are plotted as a function of PTV distance to isocenter and stratified by rotational error range from 0° to 1.5°.

D95 values are plotted as a function of GTV distance to isocenter and stratified by GTV volume at rotations of 0.5°, 1.0° and1.5°.
Multiple GEE linear regressions showed that distance to isocenter and target volume were strong predictors of D95; all baseline shifts and rotations were found to have statistical significance. P-values, CIs, and parameter estimates are reported in Table 2. For the linear GEE models at baseline shifts of 0.5, 1.0, and 2.0 mm; and rotations of 0.5°, 1.0°, and 1.5°, the Kolmogorov-type supremum testing procedure showed adequate fit (all P > .05). The values of D95 are plotted against the distance to the isocenter and stratified by volume in Figure 3. The relative combined effects of distance and volume on coverage varied with baseline shifts and rotational error. At 0.5° and 1.0°, D95 increased by 1.62 and 8.05 times, respectively, for each unit increase in distance (cm), compared to the decrease per unit increase in volume (cc). At a rotational error of 1.5°, a unit change in distance had approximately 2.93 times the effect on D95 values compared to a unit change in volume. In the multivariate logistic regression model, both PTV volume and distance to the isocenter were significantly associated with V95 coverage rates >95% at all baseline shifts and rotational errors (Table 3). At 0.5° rotational error and baseline shift within 1.0 mm, the coverage of V95 rates was >95%. All targets had V95 values <95% when the baseline shift increased to 2.0 mm and rotational error increased to 1.5°. As an illustrative case, Figure 4 shows the dosimetric effects of a 2.0 mm baseline shift combined with a 1.5° rotational error. The minimum dose of a PTV is reduced to 60% of the prescription dose. The prescription dose of PTV D95 and V95 was only 70.6% and 80.6%, respectively.

Values of D95 are plotted against the distance to the isocenter and stratified by volume. The trend line is plotted as a guide for all PTVs that the coverage of the target decreased further with increasing the distance to the target.
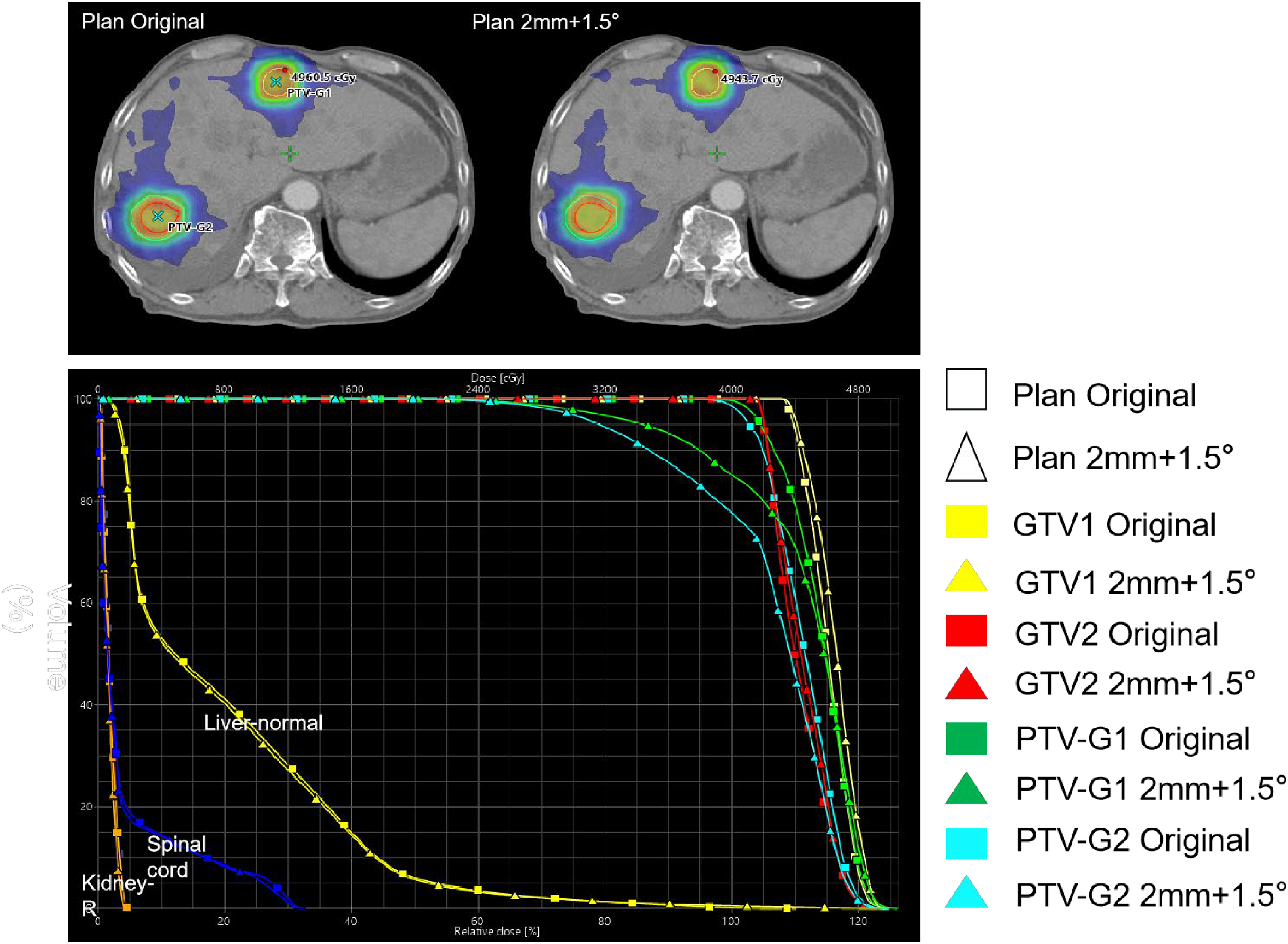
An original plan and the dosimetric effects of a 2.0 mm baseline shift combined with a 1.5° rotational error.
GEE Multivariate Linear Regression Model (Equation 1) for Predicting D95 as a Percentage of the Prescription Dose.
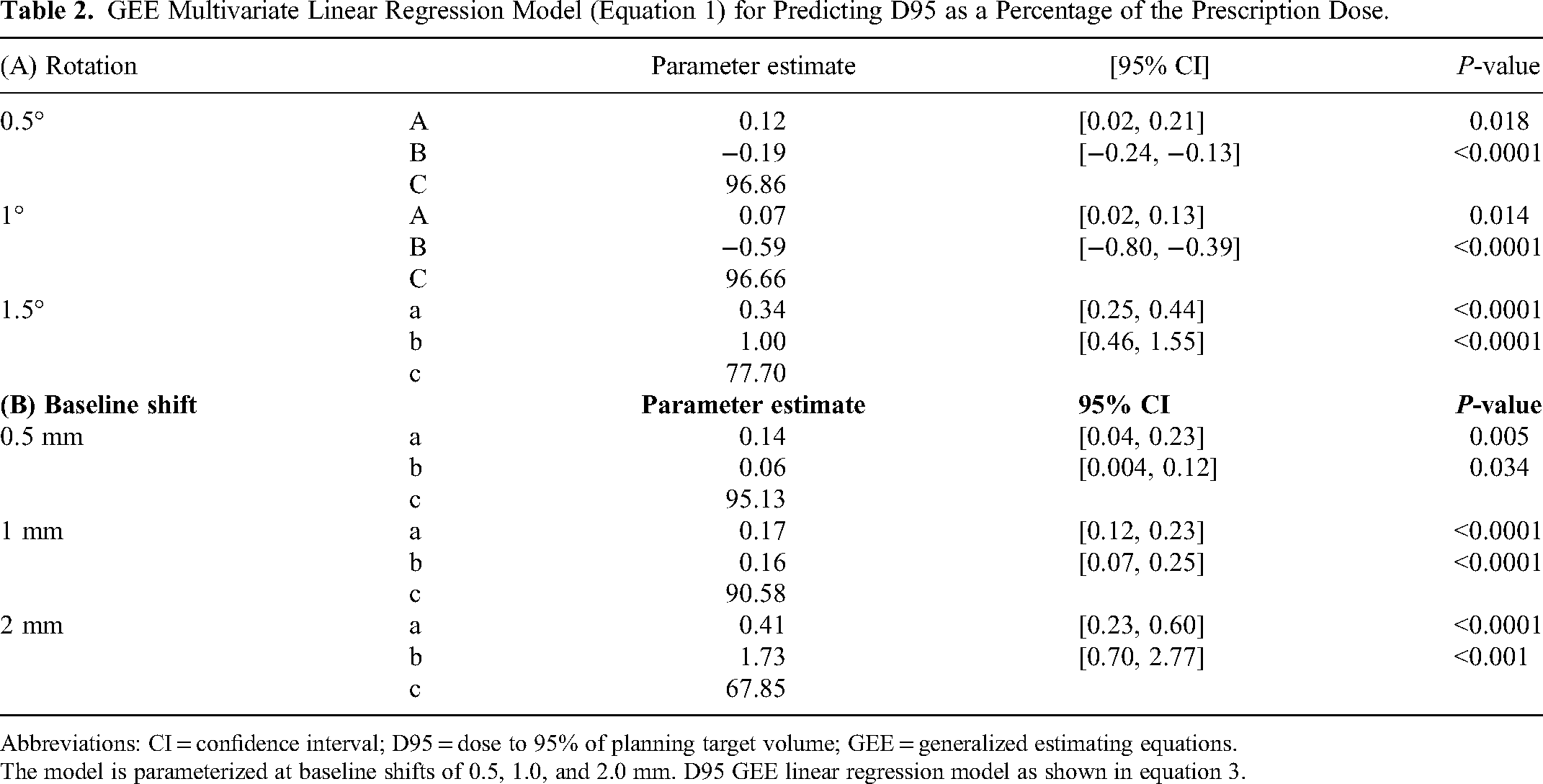
Abbreviations: CI = confidence interval; D95 = dose to 95% of planning target volume; GEE = generalized estimating equations.
The model is parameterized at baseline shifts of 0.5, 1.0, and 2.0 mm. D95 GEE linear regression model as shown in equation 3.
GEE Multivariate Logistic Regression Model (Equation 4) for Predicting the Probability (p) That V95 Exceeds 95% (Rotation Errors).

The model parameterizes rotation errors or baseline shifts. The volume of the planned target PTV and the distance from the PTV centroid to the isocenter are variables. Parameter estimates related to volume (A) and distance (B) are reported using their respective odds ratio (OR) and OR 95% confidence intervals and P-values.
Abbreviation: PTV, planning target volume.
Discussion and Conclusion
The results of this study demonstrate that the distance to the isocenter and the PTV volume are strong, statistically significant predictors of target coverage. Multivariate regression models were quantified for the effects of distance and PTV volume on target coverage. Larger targets in close proximity are more robust to baseline shift and rotational errors than smaller targets with an offset isocenter. The results of this study may help determine whether a patient is suitable for 4DCT-guided gated single-isocenter VMAT SBRT, as volumes and distances of target characteristics are easy to obtain from TPS.
In this study, the different degree of baseline displacement and rotational error was simulated for all axes. While errors may not be the same across all axes in clinical practice, the corresponding data describes how much the target coverage would be affected in a worst-case scenario. Baseline drift and rotation levels are selected based on the previous studies of baseline drift and rotation errors. 33 For tumor radiotherapy facilities equipped with breath-gated functionality and capable of a 6-day motion therapy bed, residual baseline drift is about 2.0 mm in most patients, and rotation error may be within 0.5°.34–38 Furthermore, baseline shifts of 0.5 mm within 0.5° rotation were found to still have good target coverage. When the rotational error was increased to 1.5° and baseline shift errors were increased to 1.0 mm, the D95 and V95 values were >95% in only 3 cases. When rotational and baseline shift errors were small, target coverage was similar to the ideal case of no rotation. At 0.5° and baseline shifts smaller than 1.0 mm, almost all targets had D95 and V95 values >95%. Only 2 cases had D95 and V95 values <95% and all were >93%, as they have the smallest target and the longest distance to the isocenter. For rotational errors of 1.0, 36.3% of targets had D95 and V95 values <95%. The 19.3% and 13.6% of PTVs had D95 or V95 values <90%, respectively. In general, target coverage worsened with increasing baseline shift, rotational errors, and target distance to the isocenter. However, in practice, not all clinics performing SBRT have real-time tracking capabilities and online correction of the 2 types of error. Therefore, it cannot be assumed that the baseline shift is within 0.5 mm and rotational error is within 0.5°. Furthermore, we observed the initial baseline shifts in the range of 1.0 to 3 mm, and rotational errors range from 0.5° to 2.5°. Prior studies have reported that the initial baseline shift can reach 5 mm and the initial rotation error can reach 3.0°. 39 Although our radiation therapy center has a 6D treatment table that can be corrected online, other units may rely on manual correction for initial baseline drift and rotation errors. The baseline shift and rotation of the patient observed during treatment can be large. Although extreme baseline shifts and rotational errors are uncommon, they have the potential to impair target coverage for multitarget, single-center SBRTs. Unlike PTV volume and distance to the isocenter, baseline drift, and rotational error are not known before treatment. Therefore, adopting a conservative approach to ensure safe and accurate treatment must consider at least a certain percentage of the extreme baseline drifts and rotational errors observed clinically.
For multiobjective planning, considering the motion accuracy of multileaf gratings, the current planning system usually defaults to placing the isocenter at the center of mass or geometry of the target area. 40 In this study, the Eclipse system planned the epicenter between the centroids of PTVs. Unfortunately, the results show that the center point and centroid point of planning optimization may not be consistent. In order to minimize the risk of impaired coverage of each PTV, centers should be located to favor smaller PTVs. The distance at which the isocenter should be offset depends on the PTV volume, distance, baseline drift, and uncertainty that may occur in rotational positioning. Interestingly, we also found in our experiments that larger targets have higher D95 values at nominal distances than smaller targets, and the difference is more pronounced at larger rotations. All targets had V95 values <95% when the baseline shift increased to 2.0 mm and rotational error increased to 1.5°. As observed in the D95 analysis, the effect of distance was more important for the coverage of V95. Therefore, in clinical practice, it may be optimal to set the isocentric geometric center for multiobjective planning. Another method described by Roper et al is to first set the level of target coverage, solve the distance to the isocenter according to the volume of the known target, and then set the plan isocenter within the maximum radius from the target centroid to achieve the set target coverage. 31
This study describes the dosimetric effects of baseline drift and rotational error on multitarget PTV coverage and analyses the interaction between target distance to rotational and translational center points and PTV volume. However, there are some potential limitations to this work, we recognize that there are other complex factors that can have a significant impact on dose effectiveness. In the clinical practice of liver radiation therapy in the free-breathing scenario, anatomical changes have a larger impact on the target dose distribution. 41 There are other ways to reduce target dose coverage due to rotation or baseline drift, such as scaling to PTV based on the number of and anatomical location of GTVs. The focus of this study is mainly on the dose coverage of PTV, and the dose restriction of organs at risk immediately adjacent to the target area is an important consideration in practice (eg, the stomach, small intestine, ribs, and kidneys). OAR doses due to setup errors are too high and can be as severe as those resulting in inadequate target dose coverage. Furthermore, the number of enrolled patients was relatively small, and the conclusions can be further supported by increasing the sample size in future studies. These considerations are areas for future investigation.
In conclusion, baseline shifts and rotational errors have been observed in patient studies based on 4DCT-guided gating, affecting target coverage, especially targets that are far from the isocenter and small in size. For the clinical practice of VMAT SBRT in liver multitarget single-isocenter plans, in addition to considering its initial baseline shift and rotation, the intrafraction rotation error of the angle and shift of baseline are important considerations. The results of this study may help determine whether a patient is suitable for 4DCT-guided gated single-isocenter VMAT SBRT, as volumes and distances of target characteristics are easy to obtain from the treatment plan system.
Footnotes
Abbreviations
Authors’ Notes
Yun Zhang and Shanzhou Niu contributed equally.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
The study has been approved by the Institution Review Board and Ethics Committee of Jiangxi Cancer Hospital, and the approval number is 2023ky194.
Funding
The authors acknowledge the support provided by the “Five-level Progressive” talent cultivation project of Jiangxi Cancer Hospital & Institute, Jiangxi Cancer Hospital scientific research open fund project (KFJJ2023YB21), Jiangxi Double Thousand Plan, Joint Fund of the National Natural Science Foundation of China, and the Karst Science Research Center of Guizhou Province, Science and Technology Program of Jiangxi Province (Grant Nos. WCDJ2024JQ01, jxsq2019201061, 62261002, 20192BCB23019, and 20202BBE53024).