
Abstract
Introduction
Cervical cancer ranks as the fourth most common cancer and remains a significant public health challenge for women globally. Notably, China and India collectively represent over one-third of the global burden of cervical cancer, accounting for 106 000 cases and 48 000 deaths in China in 2018. 1
In 2018, the International Federation of Gynecology and Obstetrics (FIGO) revised the staging system for cervical cancer, designating patients with regional lymph node metastasis (LNM) as stage III C. Specifically, patients with pelvic LNM alone are categorized as stage III C1, while those with para-aortic LNM are classified as stage III C2. 2 Accordingly, patients with stage III C are more likely to undergo concurrent chemoradiotherapy (CCRT)-based treatment. 3 Some researchers have confirmed the positive impact of the 2018 FIGO staging system on the prognosis of these advanced cervical cancer patients.4,5 However, the current number of reports is limited, and furthermore, certain studies have drawn conflicting conclusions, necessitating further validation.6–8 Therefore, it is crucial to accurately assess the primary tumor and lymph node (LN) status of these patients to differentiate tumor heterogeneity and plan individualized optimal treatment. 9 In this study, we evaluated the clinical outcomes and prognostic factors for 117 stage III C (FIGO 2018) cervical cancer patients treated with radical radiotherapy (RT) or radiochemotherapy at our department.
Extended-field radiotherapy (EFRT) involves RT with the upper boundary of the irradiation field above the bifurcation of the abdominal aorta, aiming to control or reduce regional recurrence and distant metastasis. All stage III C2 patients with cervical cancer require EFRT, but for stage III C1 patients, EFRT is optional. 10 At present, there are no guidelines or consistent criteria because the number, size, and distribution of LNMs all have potential impacts on the target delineation of RT. 11 Our study evaluated the anatomical distribution characteristics of pelvic LNM in stage III C cervical cancer patients, aiming to provide evidence to effectively delineate the irradiation field and offer guidance for EFRT in stage III C1 patients.
Material and Method
Patient Population
This study was approved by the Institutional Review Board with the approval number 202310-12-01 (approval date: October 30, 2023) and was conducted following the ethical standards outlined in the 1964 Declaration of Helsinki. As the study utilized previously collected clinical data, the requirement for informed consent was waived. We have de-identified all patient details to ensure that the identity of any individual cannot be determined. The reporting of this study adheres to Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines. 12
We conducted a retrospective analysis of the electronic medical records and follow-up data of a total of 117 patients enrolled in the Department of Radiotherapy at Jilin Province Cancer Hospital from January 2017 to January 2021. All cases were identified through imaging examinations and categorized into stages III C1 (98/117, 83.8%) and III C2 (19/117, 16.2%) based on the 2018 FIGO staging criteria. 3 The inclusion criteria were as follows: (1) Pathological diagnosis of cervical cancer through biopsy; (2) availability of general patient data, disease-related examination results, adjuvant treatment data, follow-up information, and survival outcomes; (3) underwent radical RT with or without concurrent chemotherapy; (4) absence of prior surgery or RT at other sites. Patients who did not meet these criteria or had special types of cervical cancer were excluded from the study.
Evaluation of the Anatomical Distribution of LN
LN involvement was diagnosed using computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography-CT (PET-CT). LN positivity was determined when the short-axis diameter was >1 cm or when there were high intensities on CT or MRI, or positive results on PET/CT. For LNs with a short-axis diameter <1 cm, positivity criteria included high intensities, irregular morphology, and central necrosis as revealed by enhanced scans.
To accurately evaluate the anatomical distribution of LNMs, we initially defined pelvic LNM into 4 sublocation groups: Common iliac, external iliac, internal iliac/obturator, and presacral LNM. Additionally, we categorized para-aortic LNMs into 3 subgroups based on vascular anatomy: Left-lateral para-aortic LNM, aortocaval LNM, and the right paracaval LNM group. Furthermore, para-aortic LNMs can also be divided into 3 subgroups according to the anatomy of vertebral bodies: Above the L2 vertebra body, between L2-L3, and below the L3 vertebra body. 13
Treatments
All patients underwent radical RT with or without concurrent chemotherapy. The RT consisted of external beam RT (EBRT), specifically three-dimensional conformal radiation therapy (3DCRT)/intensity-modulated radiation therapy (IMRT), and three-dimensional-image-guided after loading intracavitary brachytherapy (ICBT). The EBRT dose ranged from 45 to 50 Gy, delivered in 1.8 to 2.0 Gy/fraction. In cases of LNMs, the local dosage was increased to 60 to 64 Gy. ICBT typically commenced 4 weeks before the conclusion of EBRT and was administered 4 to 6 times at 6 Gy/fraction using an iridium-192 source. Overall, the total dose received by all patients for cervical tumors (EBRT + ICBT) exceeded 85 Gy. Chemotherapy included 3 regimens: Cisplatin (30-40 mg/m²/week) alone, concurrent cisplatin (30-40 mg/m²/week) and paclitaxel (60-80 mg/m²/week), and other platinum-based agents.
Follow-up Evaluations
After completing treatment, patients were regularly followed up with visits scheduled every 3 months for the first 2 years and every 6 months for the third to fifth years. All patients were followed up until March 2023 or until their death. We collected information on patients’ survival, recurrence status, and other related data. The endpoints of our research were the 3-year overall survival (OS) and disease-free survival (DFS). The former was defined as the duration from the initial date of treatment to the date of last follow-up or death from any cause, and the latter referred to the duration from the initial date of treatment to the date of recurrence/metastasis or death. 10
Statistical Analysis
The Kaplan–Meier method was utilized to create survival curves for assessing OS and DFS. The log-rank test and Cox proportional hazard regression model were employed for conducting univariate and multivariate analyses, respectively. The risk of para-aortic LNM in stage III C patients was evaluated using the Chi-squared test and logistic regression analysis. Variables with a P-value of <.05 in the univariate analysis were included in the multivariate analysis. A significance level of P < .05 was deemed statistically significant.
Results
Patient Characteristics
The demographic and clinicopathological characteristics of 117 stage III C cervical cancer patients are presented in Table 1. The median age was 54 years (range 30-73 years). Among the 117 patients, 108 (92.3%) had squamous cell carcinoma (SCC), while 9 (7.7%) had adenocarcinoma. All patients had pelvic LNM pretreatment, with 41 (35.0%) showing unilateral distribution and 76 (65.0%) bilateral distribution. Fifty-seven (48.7%) patients had <3 positive LNs involved, while 60 (51.3%) had ≥3 positive LNs. Ninety-seven patients (82.9%) underwent CCRT treatment, and the remaining 20 patients (17.1%) received radical RT alone based on their informed consent to resist or refuse chemotherapy despite recommendation.
Demographic and Clinicopathological Characteristics of 117 III C Cervical Cancer Patients

Abbreviations: SCC-Ag, squamous cell carcinoma antigen; FIGO, International Federation of Gynecology and Obstetrics; LNM, lymph node metastasis; III C, cervical cancer patients with regional LNM; III C1, cervical cancer patients with pelvic LNM; III C2, cervical cancer patients with para-aortic LNM.
The 3-Year OS and DFS Rates of Stage III C Cervical Cancer Patients
The 3-year OS and DFS rates for all patients were 75.2% and 65.8%, respectively, with a mean follow-up of 48 months (range: 4-74 months), and there were 29 deaths (24.8%). Specifically for stage III C1 and III C2 patients, the 3-year OS rates were 77.6% and 63.2% (P = .042), while the 3-year DFS rates were 70.4% and 47.4% (P = .003), as shown in Figure 1A and B. In patients with <3 and ≥3 pelvic LNMs, the 3-year OS rates were 81.0% and 68.5% (P = .058), and the 3-year DFS rates were 76.2% and 55.6% (P = .015), depicted in Figure 1C and 1D.

Kaplan–Meier curves for stage III C patients stratified by FIGO 2018 (A and B) and No. of pelvic LNM (C and D). A and C, 3-year OS, P = .042, P = .058. B and D, 3-year DFS, P = .003, P = .015. Abbreviations: III C, cervical cancer patients with regional LNM; III C1, cervical cancer patients with pelvic LNM; III C2, cervical cancer patients with para-aortic LNM; OS, overall survival; DFS, disease-free survival; LNM, lymph node metastasis; FIGO, International Federation of Gynecology and Obstetrics.
Among the 117 stage III C cervical cancer patients, distant metastases occurred in 16 individuals (13.7%) after treatment (refer to Table 2). Twelve patients were classified as stage III C1, and 4 patients as stage III C2. The most frequent distant metastases post-treatment were lung and bone metastases, with the majority occurring within 1 year. The 3-year OS and DFS of these patients were 56.7% (P = .047, compared to all patients) and 56.7% (P = .004, compared to all patients), respectively.
The Development of Distant Metastases After Treatment in 16 Stage III C Cervical Cancer Patients
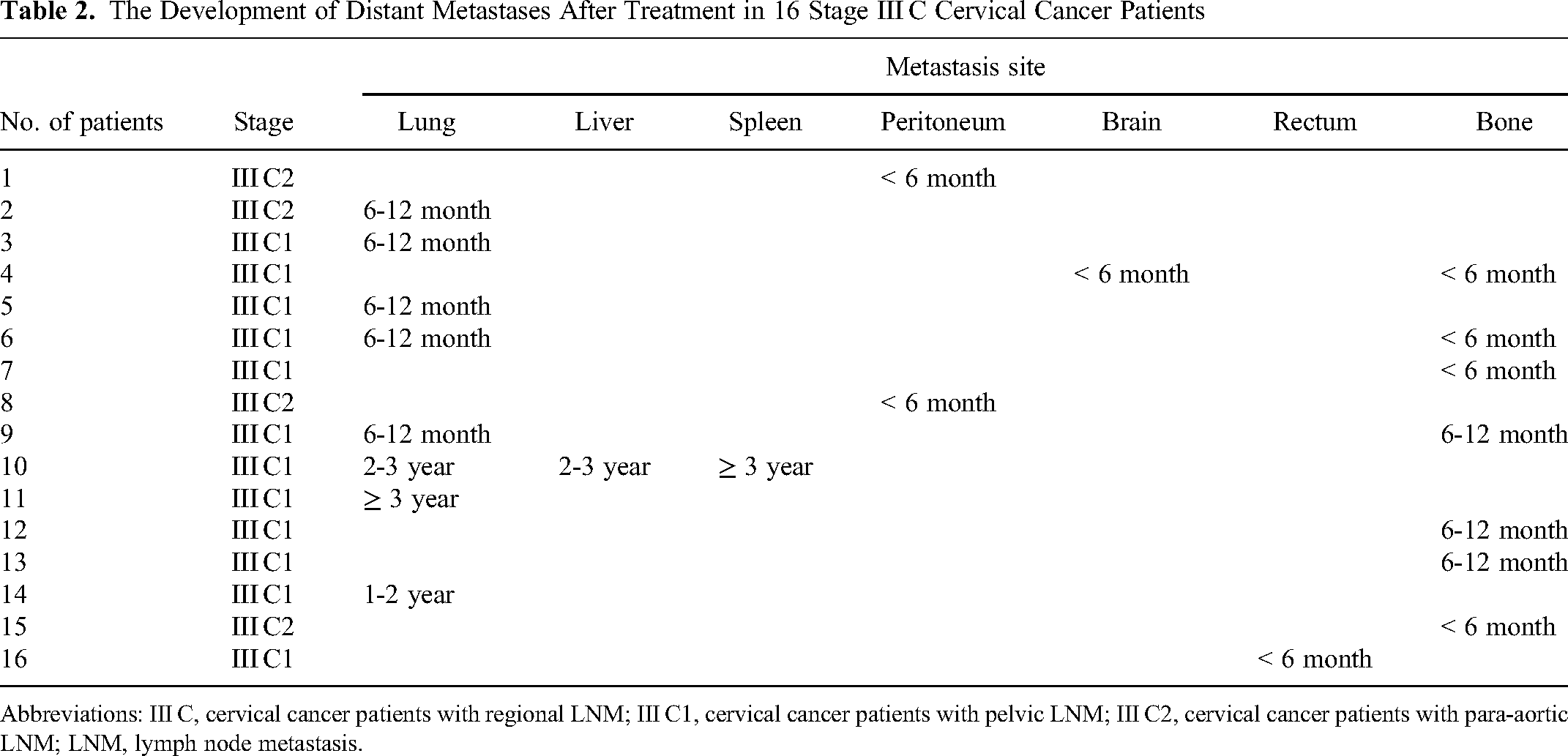
Abbreviations: III C, cervical cancer patients with regional LNM; III C1, cervical cancer patients with pelvic LNM; III C2, cervical cancer patients with para-aortic LNM; LNM, lymph node metastasis.
Prognostic Factors for OS and DFS
Table 3 indicates that the pretreatment location of pelvic LNM, histological type, and FIGO stage were prognostic indicators for 3-year OS (all P < .05), while the number of pelvic LNM as well as FIGO stage were prognostic indicators for 3-year DFS (all P < .05). Upon incorporating these variables into the multivariate analysis, the results revealed that histological type stood as an independent prognostic factor for OS (hazard ratio [HR] = 0.280, 95% CI: 0.104-0.753, P = .012), and the number of pelvic LNM (HR = 0.498, 95% CI: 0.256-0.970, P = .040) and FIGO stage (HR = 0.472, 95% CI: 0.225-0.988, P = .046) were independent prognostic factors for DFS in stage III C cervical cancer patients (refer to Table 4). The number of pelvic LNM ≥ 3 exhibited a trend toward statistical significance for OS. When we included this trend in the multivariate analysis (see Supplemental Table 1), 14 the result indicated that it also served as an independent prognostic factor for OS (HR = 0.432, 95% CI: 0.198-0.943, P = .035).
Univariate Analysis of Prognostic Factors for 3-Year OS and DFS in Stage III C Cervical Cancer Patients
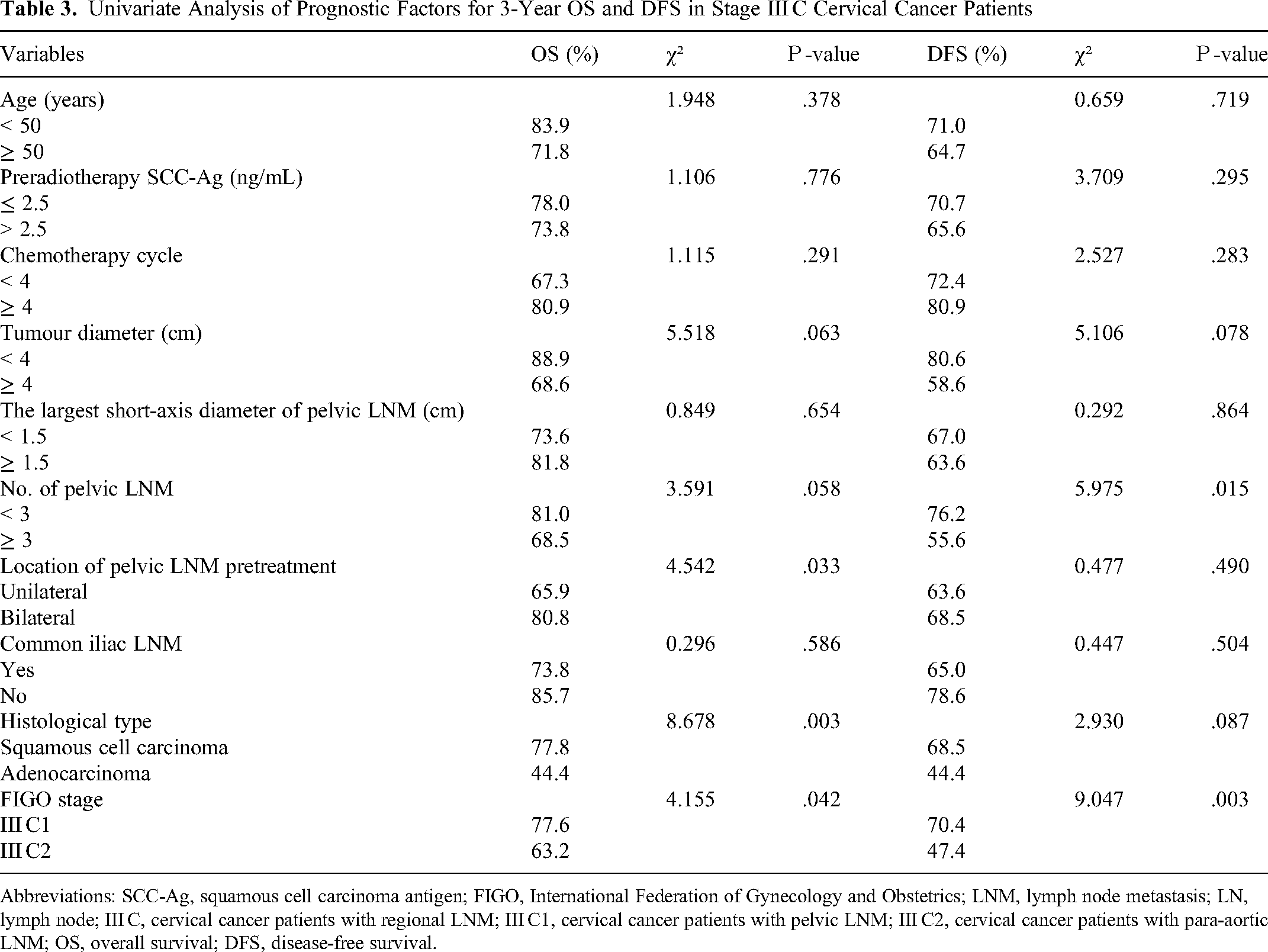
Abbreviations: SCC-Ag, squamous cell carcinoma antigen; FIGO, International Federation of Gynecology and Obstetrics; LNM, lymph node metastasis; LN, lymph node; III C, cervical cancer patients with regional LNM; III C1, cervical cancer patients with pelvic LNM; III C2, cervical cancer patients with para-aortic LNM; OS, overall survival; DFS, disease-free survival.
Multivariate Analysis of Prognostic Factors for 3-Year OS and DFS in Stage III C Cervical Cancer Patients

Abbreviations: III C, cervical cancer patients with regional LNM; LNM, lymph node metastasis; FIGO, International Federation of Gynecology and Obstetrics; OS, overall survival; DFS, disease-free survival.
Given the small number of 19 patients in stage III C2, which is inadequate for defining survival analysis, we specifically evaluated the data of stage III C1 patients alone. The outcomes revealed that the number of pelvic LNM was a prognostic indicator for 3-year DFS (P = .026), and histological type was a prognostic indicator for 3-year OS (P = .002). There was also a trend toward statistical significance for DFS (P = .053); hence, we incorporated it into the multivariate analysis as well. The result demonstrated that the number of pelvic LNM stood as an independent prognostic factor for DFS in stage III C1 cervical cancer patients (refer to Supplemental Tables 2 and 3).
Furthermore, we conducted an investigation into the correlation between the number of pelvic LNM and DFS. The results showed that there was a weak negative correlation between the 2 variables among all stage III C patients (r = −0.249, P = .007, Pearson correlation), but not among stage III C1 patients (r = −0.177, P = .082).
Anatomical Distribution of Pelvic and Para-aortic LNM in Stage III C Cervical Cancer Patients
To assess the potential impact of pelvic and para-aortic LNM on EFRT for cervical cancer patients, we analyzed the anatomical distribution of pelvic and para-aortic LNM in 117 stage III C cervical cancer patients (see Tables 5, 6, and Supplemental Table 4). The number of pelvic LNM was highest in the internal iliac/obturator region (284/365, 77.8%), followed by the external iliac (45/365, 12.3%) and common iliac LNM groups (26/365, 7.2%), and lowest in the presacral LNM group (10/365, 2.7%).
Distribution of Pelvic LNM (n = 365) in Stage III C Cervical Cancer Patients

Abbreviations: LNM, lymph node metastasis; III C, cervical cancer patients with regional LNM; III C1, cervical cancer patients with pelvic LNM; III C2, cervical cancer patients with para-aortic LNM.
Distribution of Para-aortic LNM (n = 60) in Stage III C2 Cervical Cancer Patients

Abbreviations: LNM, lymph node metastasis; III C2, cervical cancer patients with para-aortic LNM; L2: lumbar 2 vertebra body; L3: lumbar 3 vertebra body.
Subgroups divided by the vascular anatomy
Subgroups divided by the anatomy of vertebral bodies
In terms of the distribution of para-aortic LNMs, they were primarily located between the L2-L3 and L3 vertebra body below group (44/60, 73.3%). When considering subgroups divided by blood vessels, para-aortic LNMs were most frequently observed in the left-lateral para-aortic region (41/60, 68.3%), followed by the aortocaval (15/60, 25.0%) and right paracaval sites (4/60, 6.7%).
We then tried to analyze the correlation between the distribution of pelvic LNM and the prognosis of stage III C1 cervical cancer patients. As the numbers of common iliac LNM and presacral LNM were too small to calculate, we only integrated into the internal iliac/obturator LNM and external iliac LNM. The results suggested that the number of left and right internal iliac/obturator LNM respectively had a weak negative correlation with the 3-year DFS of stage III C1 cervical cancer patients (r = −0.233, −0.249; P = .044, .031, respectively), but their summation showed no correlation with prognosis (refer to Supplemental Table 5).
High-Risk Influencing Factors for Para-Aortic LNM in Stage III C Cervical Cancer Patients
The emergence of para-aortic LNM represents a significant event in the progression of cervical cancer, directly impacting treatment decisions and patient prognosis. As depicted in Table 7, tumor diameter, the largest short-axis diameter of pelvic LNM, the number of pelvic LNM, location of pelvic LNM, and the presence of common iliac LNM were identified as high-risk influencing factors for para-aortic LNM. Upon incorporating the variables with P < .05 from the Chi-squared test into the logistic regression analysis, the results revealed that the largest short-axis diameter of pelvic LNM ≥ 1.5 cm and the presence of common iliac LNM stood out as the primary high-risk influencing factors for para-aortic LNM in stage III C cervical cancer patients.
Analysis of the High-Risk Influencing Factors for Para-aortic LNM in Stage III C Cervical Cancer Patients

Abbreviations: SCC-Ag, squamous cell carcinoma antigen; LNM, lymph node metastasis.
Discussion
Currently, the uniformly recommended treatment for stage III C cervical cancer is radical chemoradiotherapy. However, due to its heterogeneous features in tumors and prognoses, the rationality of this stage III C classification remains controversial. To gain a better understanding of and effectively manage patients with this form of cervical cancer, we conducted a retrospective analysis of 117 patients with stage III C who were treated with radical RT or CCRT at our institution. The results revealed that patients in stage III C2 exhibited worse 3-year OS and DFS rates (63.2% and 47.4%) compared to those in stage III C1 (77.6% and 70.4%). Histological type emerged as an independent prognostic indicator for OS, while the number of pelvic LNM and FIGO stages served as independent prognostic indicators for DFS. Our results were consistent with several previous reports.15,16 For instance, Liu et al 17 reviewed the clinical records of 325 stage III C1 patients treated with CCRT, revealing a 3-year DFS rate of 66.3%. Tumor size of ≥ 4 cm and the number of pelvic LNM ≥ 2 were identified as adverse prognostic factors for DFS. Furthermore, these studies also underscored the inherent heterogeneity of stage III C cervical cancer.
Recently, Pinto et al 10 published retrospective data that included 62 patients with locally advanced cervical cancer treated with RT and chemotherapy. They reported a 3-year OS of 70.8% and a DFS of 64.6%. The total number of deaths during the study period was 20 (32.3%). Patients diagnosed with adenocarcinoma exhibited a worse prognosis in comparison to those with squamous cell carcinoma. They observed that pelvic LN size (> 2.5 cm) had a negative impact on OS. Our result was inconsistent with theirs, possibly due to the parameter we used, which was set at 1.5 cm. It's worth noting that Song et al 18 employed the same measurement criteria as we did. However, due to disparities in case selection (268 patients with cervical cancer in stage I B1-IV B), they discovered that patients with LNs >1.5 cm experienced a worse 5-year OS.
Duan et al 6 identified 2660 confirmed stage III C cervical cancer cases, dividing them into 4 substages: III C-T1, III C-T2a, III C-T2b, and III C-(T3a + T3b). They reported 5-year OS and DFS rates of 82.1% and 74.7% in III C-T1, 76.1% and 65.9% in III C-T2a, 75.8% and 73.7% in III C-T2b, and 68.0% and 64.8% in III C-(T3a + T3b), respectively. Their findings emphasized that LN status alone might be insufficient for determining the clinical characteristics of stage III C patients and could be inappropriate in the clinical setting. Importantly, their study specifically excluded cases with preoperative treatment or underdosage of RT. Our study addresses this issue, albeit with a relatively small number of cases.
Ryu et al 19 conducted a study involving 119 stage III C1 and 15 stage III C2 cervical cancer patients treated with chemoradiotherapy. They reported 5-year OS rates of 74.5% and 38.1%, respectively. Their findings suggested that age, para-aortic LNM, and pelvic side wall invasion were independent prognostic factors for survival. Similarly, our study also had a small number of stage III C2 patients (19 cases), which rendered statistical analysis invalid. Consequently, we focused on evaluating the data of stage III C1 patients alone to ensure a more accurate assessment. However, due to incomplete data, we were unable to calculate the 5-year survival rate.
To validate the 2018 FIGO staging system, Liu et al 20 evaluated 586 stage III C cervical cancer patients (31 III A, 142 III B, 325 III C1, and 88 III C2) who underwent definitive RT in China. They reported 3-year DFS rates of 79.9%, 70.4%, 66.3%, and 29.8%, respectively. Their findings indicated that the 2018 FIGO staging system demonstrated greater distinction within stages and better predictive accuracy for DFS compared to the previous staging system. Raut et al 14 also validated the FIGO Classification 2018 in patients with locally advanced cervical cancer treated with chemoradiation. The 3-year DFS rates based on restaging according to FIGO 2018 for stage I B, II A, II B, III A, III B, III C1, III C2, and IV A was 100%, 93%, 84%, 53%, 77%, 74%, 61%, and 61%, respectively.
Nevertheless, data from some studies have suggested that the ability of the new FIGO staging system, particularly stage III C, to guide prognosis may be limited. 14 Yang et al 7 proposed that higher FIGO 2018 staging was less consistently associated with worse 5-year OS, as the differences among stage III Cr, IA-IB, and IIA-IIB cohorts were not statistically significant. Interestingly, the number of LNs in the stage III C cohort in their study was notably lower than in our results (154 vs 365 + 59). This may be attributed to the fact that their included patients all underwent standard surgery and pelvic lymphadenectomy, although they did not provide detailed information. Furthermore, they also suggested that using the diameter of LNs in imaging tools to predict metastasis had minimal clinical significance.
Long et al 8 validated the predictive power of the 2018 FIGO staging system for the prognosis of stage III C cervical cancer patients. A total of 418 patients were eligible for analysis, including 42 in stage III A, 120 in III B, 190 in III C1, and 66 in III C2. The 5-year OS rates were 43.3%, 40.6%, 54.1%, and 23.1%, respectively. Patients with stage III C1 cervical cancer exhibited heterogeneous clinical characteristics, reflecting variable prognoses, which depended on the T stage and the extent of pelvic LNMs. They recommended restaging stage III C1 cervical cancer based on the T stage, considering tumor size, local tumor invasion, and LNM. Large multicenter trials are warranted to validate these findings.
Matsuo et al 21 similarly validated the 2018 FIGO staging system using data from the SEER database. 21 The study included 11 733 patients with stage III cervical cancer. The most common substage was stage III C1 (n = 6888), followed by stage III B (n = 3812), and stage III A (n = 1033). Their results revealed that stage III C1 disease had better survival outcomes than stage III A and III B disease, with 5-year survival rates of 62.1%, 46.0%, and 42.6%, respectively. Furthermore, the survival outcomes of stage III C1 disease significantly differed based on the T stage, implying that local tumor factors, in addition to nodal status, are crucial determinants of survival. However, their validation included only a stage III C1 cohort, and the presence of para-aortic LNM was not classified or analyzed, thus potentially limiting its representation of the real-world scenario in cervical cancer. There are urgent needs for more reports, particularly prospective studies that can accurately predict the oncology outcomes of such patients in the future.
LNM was not incorporated into the staging system until the 2018 FIGO classification update. 22 Pelvic and para-aortic LNM are major prognostic factors in cervical cancer; therefore, it is important and promising to detect them preoperatively. 10 Currently, pretreatment LN assessment is primarily performed by imaging, with DWI-MRI exhibiting the highest sensitivity and [18F] FDG-PET-CT demonstrating the highest specificity.23,24 Our study aimed to evaluate the anatomical distribution of pelvic and para-aortic LNM. The diagnoses for LN involvement were conducted by CT (n = 7), MRI (n = 106), and PET-CT (n = 4). The results are partially inconsistent with previous reports,7,11 likely due to the relatively low diagnostic accuracy of CT or MRI, coupled with the difficulty in diagnosing LNM. 25 For example, many metastatic LNs are of normal size. Meanwhile, enlarged LNs could be benign lesions, such as inflammation or reactive hyperplasia lesions. 26
The incidence rates of LNM in advanced cervical cancer have been less reported so far due to its inherent heterogeneity, making the issue correspondingly complex. One important reason for this complexity is that the effect of LNM varies by T stage. 27 Duan et al 6 suggested that it might be unnecessary to subdivide cases with T3a/T3b by LN status. Aslan et al 28 evaluated the prognostic value of LN ratio (LNR) in 185 stage III C cervical cancer patients who underwent primary treatment by radical hysterectomy. All patients received adjuvant chemoradiation after surgery. The 5-year DFS was 62.5%, while the 5-year OS rate was 70.4%. Nonsquamous histology and LNR ≥ 0.05 were independent prognostic factors for decreased DFS. Clinicians should pay attention to LNR as a newly identified prognostic factor in stage III C cervical cancer.
McComas et al 27 reinforced the evidence that nodal status influenced survival and suggested a robust application for the new FIGO staging system. Their study included 11 853 N0 patients, 4451 III C1 patients, and 869 III C2 patients. The 5-year OS was 78.5%, 61.9%, and 39.4%, respectively. The prognoses were negatively affected by the presence of LNM and T stage with the risk of death at nearly 1.5 times greater for pelvic node involvement and 2 times greater for para-aortic node involvement. Patients with tumors ≤ 4 cm did not experience an increased risk of death. However, it's important to note that they only analyzed the 5-year OS. Although the sample size in our study was relatively small, we attempted to analyze the correlations between the distribution of pelvic LNM and the prognosis of stage III C1 cervical cancer patients. Our result showed that either the number of left or right internal iliac/obturator LNM had a weak negative correlation with 3-year DFS of stage III C1 patients, but the sum of both did not. This paradoxical result needs to be further confirmed in a larger and well-controlled study.
Cervical cancer patients with pelvic LNM are at high risk of developing para-aortic LN relapse and thus might benefit from elective EFRT. 10 Srinivasan et al 11 validated a para-aortic lymph nodal contouring atlas in cervical cancer. They showed that the most common location of para-aortic LNM was the left para-aortic area below the inferior mesenteric artery (105 LN-52%), followed by the aortocaval region (55 LN-27.2%), and the precaval region (14 LN-6.9%). Our results were in agreement with previous studies.13,29,30 We found an asymmetrical distribution of para-aortic LNM with an increased risk of LN involvement in the left lateral para-aortic and aortocaval regions, with most para-aortic LNM occurring in the region of the L2-L3 interspace and the L3 vertebra body below. The role of elective EFRT remains debatable in the absence of a large-scale randomized trial involving modern RT techniques. 31 In this regard, a multicenter EMBRACE-II study is currently ongoing, which prescribes the addition of para-aortic irradiation. 32
Possible risk factors for developing para-aortic LNM might include age, tumor size, FIGO stage, SCC-antigen (Ag) elevation, number of pelvic LNM, and tumor extension to the pelvic wall.33,34 We also analyzed the high-risk influencing factors for para-aortic LNM. The largest short-axis diameter of pelvic LNM ≥ 1.5 cm and the presence of common iliac LNM were the main risk factors influencing para-aortic LNM in stage III C patients (P = .046, .006, respectively). Specifically, the data we used for this analysis were collected before the initiation of treatment. At that time, we considered all the patients as a single group because their disease had not been interfered with prior to this point, reflecting the natural occurrence of their para-aortic LNM. Additionally, during the post-treatment follow-up, we found that only 3 stage III C1 patients developed para-aortic LNM, which is too small a sample for meaningful analysis. Although the sample size is relatively small, the results of our study may contribute to an extended understanding of the clinical characteristics for advanced cervical cancer.
The SCC-Ag is currently the most widely used marker for squamous cell carcinoma of the cervix. A high level of preradiotherapy SCC-Ag has been proven to be a significant risk factor for pelvic nodal failure. 35 However, the diagnostic power is still insufficient. 23 Our results also showed that preradiotherapy SCC-Ag had no effect on the prognosis of stage III C cervical cancer.
The present study had several limitations. Firstly, it was a single-institutional retrospective study with selective bias due to missing information. Secondly, the number of cases, especially those in stage III C2, was relatively small, leading to an imbalance between the groups. Thirdly, the presence of LNM was identified by imaging examination alone. Lastly, we performed survival analysis only for 3 years and did not evaluate other parameters. Therefore, we need to further explore and identify the results in the future through large-scale prospective trials.
Conclusion
In summary, this study retrospectively evaluated the prognostic factors of stage III C cervical cancer and assessed the anatomical distribution of LNM. The histological type, number of pelvic LNM, and 2018 FIGO stage were identified as prognostic factors that negatively affect survival outcomes. Additionally, the largest short-axis diameter of pelvic LNM ≥ 1.5 cm and the presence of common iliac LNM were the main risk factors influencing para-aortic LNM in stage III C patients. The results of this study validated the 2018 FIGO staging criteria in stage III C cervical cancer patients who underwent CCRT, providing a deeper understanding of the updated staging criteria and aiding in better patient management for those in stage III C. A large-scale prospective study is warranted to better manage this group of patients in the future.
Supplemental Material
sj-docx-1-tct-10.1177_15330338241254075 - Supplemental material for Clinical Outcomes and Prognostic Factors in Stage III C Cervical Cancer Patients Treated with Radical Radiotherapy or Radiochemotherapy
Supplemental material, sj-docx-1-tct-10.1177_15330338241254075 for Clinical Outcomes and Prognostic Factors in Stage III C Cervical Cancer Patients Treated with Radical Radiotherapy or Radiochemotherapy by Wenting Zhang, Hong Yu, Yuting Xiu, Fanxu Meng, Zhuo Wang, Kangkang Zhao, Yunlong Wang, Zhishen Chen, Juntian Liu, Jie Chen and Baosheng Sun in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Science and Technology Development Plan Project of Jilin Province, China (20210203096SF), and the Jilin Province Health Science and Technology Capability Improvement Project, China (2023LC064).
Ethical Approval
The study was reviewed and approved by the Jilin Province Cancer Hospital Institutional Review Board. Approval number: 202310-12-01. The date of approval was October 30, 2023.
Informed Consent
The need for informed consent was waived due to the retrospective nature of the study. This was reviewed and approved by the Jilin Province Cancer Hospital Institutional Review Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.