
Abstract
Introduction
Collecting duct carcinoma (CDC), originating from the principal cells in the collecting duct of the renal medulla, 1 is an extremely rare form of renal cell carcinoma (RCC) with a poor prognosis and an incidence of less than 3% among all RCCs.2–4 In 1979, Cromie et al. first found that the epithelial cells of the distal Bellini duct are the source of CDC. 5 However, CDC was identified as a distinctive type of RCC by Fleming and Lewi in 1986. 6 CDC primarily affects males, and the median age ranges from 53 to 66 years.7–9 Hematuria is the most common presenting symptom, 9 but it is not specific; therefore, the diagnosis is performed based on pathology.
CDC has a more aggressive behavior and poorer prognosis than clear cell RCC (ccRCC) as most patients have metastases at the initial presentation. CDC differs from other types of renal cancers in its histological features, but is similar to upper tract urothelial carcinoma (UTUC). Because CDC is rare, it has been difficult to conduct large-scale clinical trials, and there is no standard treatment protocol. Due to the poor response to targeted therapies, the European Association of Urology guidelines 10 recommend surgery for CDC, but the strength rating is weak.
Owing to the rarity of this disease, the understanding of CDC remains insufficient. To the best of our knowledge, only approximately 3 studies have been conducted on CDC with more than 20 cases in a single center.8,11,12 Case reports and reviews are the main sources for improving our cognition of CDC. In this study, the clinical, imaging, pathologic characteristics, treatment, and prognostic outcomes of CDCs were retrospectively analyzed to provide insights into the disease.
Materials and Methods
Study Population
This study conforms to the strengthening the reporting of observational studies in epidemiology (STROBE) guidelines. 13 This study was approved by the Ethics Committee of Jinling Hospital (2022NZKY-004-01) on January 21, 2022, and written informed consent was waived for this study given its retrospective design. A total of 25 patients with CDC were collected, and 2 patients were excluded due to the loss of follow-up. The clinical, imaging, and pathological data of 23 patients confirmed to have CDC by surgical pathology between 2003 and 2020 at Jinling Hospital were analyzed by reviewing the charts and conducting follow-up via telephone. All patient details have been de-identified.
Patient Information
We collected information about the patient's gender, age, initial presentation, tumor size, tumor site, the tumor-node-metastasis (TNM) stage, and treatment methods. Imaging information, including ultrasound (US), computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET)/CT were also collected. Immunohistochemistry (IHC) was used to distinguish CDC from other tumors. All patients were followed up until December 2021 or death.
Statistical Analysis
Descriptive statistics were used to analyze the clinical variables. Kaplan–Meier method was used to assess overall survival (OS), which was defined as the time from the date of surgery to December 2021 or death. The log-rank test was used to assess differences among these variables. Cox regression analysis was employed to identify variables independently related to OS. SPSS version 21 and R software version 4.1.2 were used for statistical analyses.
Results
Clinical Characteristics of CDC
From 2003 to 2020, approximately 4900 patients were diagnosed with malignant renal tumors at our institution. Among them, 25 were diagnosed with CDC. The proportion of CDCs among all malignant renal tumor cases was 0.51%.
The mean age of the study population was 50.8 ± 12.4 years and ranged from 26 years to 71 years. The majority of patients were male (56.5%). The mean tumor size was 6.58 ± 2.56 cm in diameter, ranging from 2.5 cm to 13.5 cm. Tumor involvement was observed in 34.8% of the right kidney and 65.2% of the left kidney. Three patients (13.0%) had stage I disease, 1 (4.3%) had stage II disease, 10 (43.5%) had stage III disease, and 9 (39.1%) had stage IV disease. More than 73.9% of the patients had metastatic disease at diagnosis. The proportions of lymph node and distant metastases at the time of diagnosis were 52.2% and 30.4%, respectively. Of the 7 patients with distant metastases, the most common metastatic sites were the bone (n = 4), liver (n = 2), ureter (n = 2), lung (n = 1), and pleura (n = 1). Of the 16 patients who did not develop distant metastases at diagnosis, 11 developed distant metastases in the lung (n = 5), bone (n = 5), pancreas (n = 1), and liver (n = 1) after surgery, with a median distant metastasis time of 4 months. At the time of diagnosis, most cases (87.0%) had clinical symptoms, and the remaining 3 patients had asymptomatic incidentally discovered tumors. The main clinical symptoms included flank pain (n = 13), macrohematuria (n = 9), fever (n = 3), and chest pain (n = 1). The characteristics of patients with CDC in the study are listed in Table 1.
Characteristics of Patients with Collecting Duct Carcinoma (CDC).

Treatment
All patients in this study underwent surgery. Regarding the treatment modalities used, 20 patients (87.0%) underwent nephrectomy. Among them, 17 patients underwent retroperitoneal laparoscopic radical nephrectomy, 2 underwent open radical nephrectomy, and 1 underwent open radical nephrectomy combined with inferior vena cava thrombectomy. The remaining 3 patients underwent retroperitoneal laparoscopic (1 case) or open nephroureterectomy (2 cases). Nine (39.1%) patients received subsequent therapeutic interventions including radiotherapy (n = 4, 17.4%), chemotherapy (n = 6, 26.1%), and targeted therapy (n = 4, 17.4%). Of the patients who underwent radiotherapy, 2 had lung metastases, 1 had retroperitoneal metastases, and 1 had bone metastases. Of the patients who received chemotherapy, 2 had multiple metastases, 2 had bone metastases, 1 had liver metastases, and 1 had lung metastases. The most frequently administered chemotherapy regimen was gemcitabine combined with cisplatin (n = 3, 13.0%), followed by gemcitabine monotherapy (n = 2, 8.7%), carboplatin plus paclitaxel (n = 1, 4.3%). Four patients received targeted therapy owing to disease progression, including sunitinib (n = 2, 8.7%), sorafenib (n = 1, 4.3%), and apatinib (n = 1, 4.3%).
Imaging Features
CT was the main imaging modality for CDC (22 of 23), MRI was used in 3 cases, and PET/CT was used in 5 patients before surgery. Twenty-one patients underwent US examination, including conventional US, color Doppler ultrasound (CDUS), and 8 patients underwent contrast-enhanced ultrasound (CEUS). The radiographically occurring locations of CDC for the 23 patients differ: 13 in the cortex-medullary region, 7 in the cortex-medullary-pelvis region, and 3 in the medullary-pelvis. Most lesions presented mass type according to the morphology in imaging, and 1 presented diffuse nephritis-like change type.
In US, the tumor showed low or mixed signals and clear or unclear borders, and CDUS images demonstrated blood flow within the masses. CEUS showed that all tumors were more enhanced than the adjacent renal parenchyma. The enhancement was heterogeneous and earlier (3), later (3), or simultaneous (2) than that of the adjacent renal cortex, and the washout of the tumor was earlier (6) or simultaneous (2) than that of the adjacent renal parenchyma.
Of the 22 patients who presented mass type, the lesions appeared as solid (19) or cystic solid (3) tumors with clear or unclear borders and often presented irregular shapes in CT. Tumors were hypointense or with an inhomogeneous density in plain CT scan images, and uneven enhancement was observed after contrast injection. Three patients were misdiagnosed as UTUC (Figure 1A and B).

An irregular tumor in plain CT scan images (A) and uneven enhancement were observed after contrast injection (B). An irregular tumor displayed isointense signal shadows on T1-weighted images (C), slightly hypointense in T2WI (D), and uneven enhancement within the tumor (E). CT (F and G) and corresponding fusion (H and I) images showed intense FDG uptake of the left renal tumor and bone.
In MRI, the lesions appeared as irregular solid tumors with unclear borders, and showed mixed signals that displayed isointense signal shadows on T1-weighted images (Figure 1C). The tumor signals were variable on T2-weighted images: One tumor was slightly hypointense, and the other 2 were slightly hyperintense (Figure 1D). Perfusion imaging revealed uneven enhancement within the tumor (Figure 1E).
In PET/CT, renal tumors and metastatic lesions showed intense fluorodeoxyglucose (FDG) uptake. The maximum standardized uptake value (SUVmax) of the tumor ranged from 7.1 to 22.4, and the SUVmax of metastatic lesions ranged from 6.7 to 36.6 (Figure 1F-I).
Pathology
All renal tumors were retrospectively reviewed by an expert urological pathologist. Macroscopically, the cut surface was gray-white/gray-yellow/gray-red in color, with a moderate or firm texture. Microscopically, CDCs display a tubular/tubule-papillary/cord/nest growth pattern and an infiltrative growth pattern associated with desmoplastic stromal reaction. Coagulative tumor necrosis was found in 3 patients (13%) and sarcomatoid differentiation was found in 4 patients (17.4%). Most patients (95.7%) underwent IHC to assist in the diagnosis. The results of IHC were expressed as “positive/total numbers” as follows: Pax-8(12/12), CKpan(5/5), CK19(9/11), Vimentin(17/19), E-cad(9/12), P504s(8/14), Ksp-cad(2/4), RCC(3/11), CD10(7/21), CD117(0/12), CA9(6/7), CK7(6/18), CK20(1/5), EMA(4/5), Melan-A(0/6), FH(3/3), CD31(0/2), CD34(0/2), GATA-3(1/7), CK5/6(0/5), Villin(1/5) P63(2/9), INI-1(2/2), Pax-2(3/5), Cathepsin-K(1/4), TFE3(2/8), HMB-45(0/4), Melan-A(0/6), SDHB(2/2), S-100(3/3), and 34βE12(1/2) (Figure 2A-F). The Ki-67 index of patients ranged from 5% to 70%.
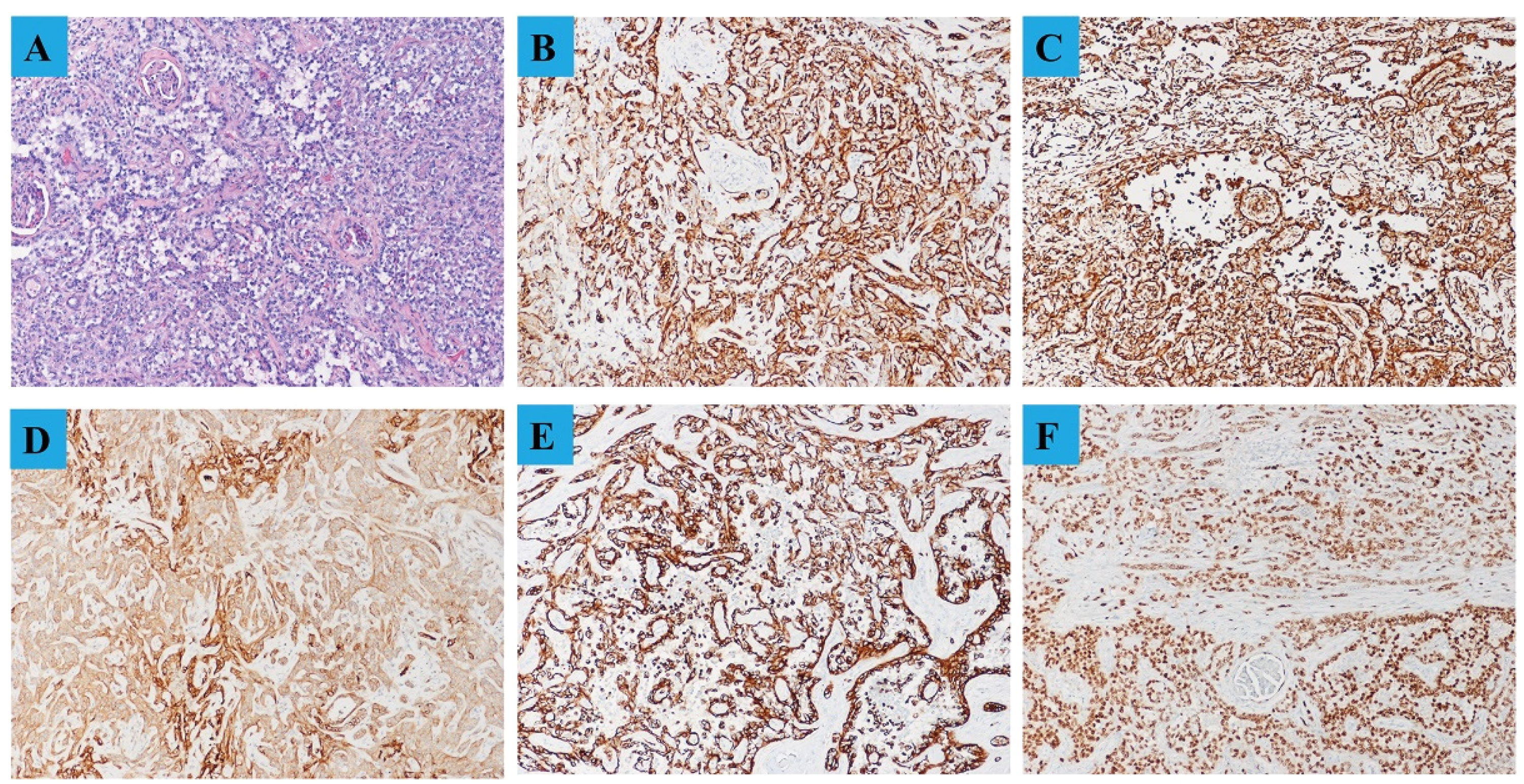
Hematoxylin and eosin staining demonstrated that malignant epithelial tumor with a predominantly invasive tubular growth pattern and an associated desmoplastic response in the adjacent stroma (A) (100×). Immunohistochemistry (IHC) showed CKpan 3+ (B), Vimentin 3+ (C), CA9 3+ (D), CK19 3+ (E), and PAX-8 3+ (F) (100×).
CDC Prognosis
The median follow-up period was 12 months (range: 4-62 months). The median OS was 12 months (95% CI: 10.136-13.864; Figure 3A). In this cohort, 22 patients died because of disease progression, and 1 was still alive at the end of the follow-up period. The OS rates at 1 year and 2 years were 43.5% and 26.1%, respectively. Notably, 2 patients with CDC survived for more than 4 years. One survived 62 months and had stage T1aN0M0 disease; the other survived more than 52 months by the end of follow-up and had stage T2aN1M0. The OS rates were significantly higher in patients with symptoms than in patients without symptoms (12 months vs 7 months, P = .007; Figure 3B), and differences in median survival time between patients with and without distant metastases were statistically significant (10 months vs 22 months, P = .022; Figure 3C).

Kaplan–Meier curves of survival. (A) Overall survival (OS). (B) According to symptom. (C) According to distant metastasis.
Univariate Cox regression analysis suggested that distant metastasis and no symptoms at initial diagnosis were risk factors for prognosis. Variables with P < .05 in univariate analysis were enrolled in the multivariate Cox regression analysis. Finally, multivariate Cox analysis revealed that no clinical symptoms at initial diagnosis and distant metastasis were independent prognostic factors for CDC patients. The results of this analysis are shown in Table 2.
Univariate and Multivariate Analyses of the Overall Survival (OS).

Discussion
A study 7 based on the Surveillance, Epidemiology, and End Results database found that CDC is more common in the white, males, and married individuals; the median age was 59 years; advanced stages accounted for the majority of cases, and tumors were more frequently detected in the left kidney. Similar to other studies,8, 14, 15 we observed that CDC was common in middle-aged men; there was a preference for men, with a male-to-female ratio of 1.3:1. Moreover, tumors were more likely to occur in the left kidney.
The clinical presentation of CDC is highly variable according to the depth of invasion and tumor location. Most patients with CDC present with gross hematuria, followed by abdominal pain, weight loss, and palpable masses. 16 However, these symptoms are not specific, and some RCCs can present similar clinical symptoms. In our study, most patients presented various clinical presentations at diagnosis. Flank pain was the most common presentation, followed by gross hematuria. This study suggested that patients without clinical symptoms were a risk prognostic factor, but the reason is still unclear. We found that 2 of the 3 asymptomatic patients with stage III, and all 3 patients developed distant metastasis shortly after surgery.
Generally, CDC is difficult to distinguish from other types of RCC by nonspecific radiological features. The presence of a medullary-located solitary tumor and invasion in the renal sinus region in imaging may help remind us of the possibility of diagnosing CDC when the tumor is small. 17 However, it is difficult to differentiate when the tumor is large. 18 One study confirmed that 18F-FDG-PET/CT could be used to evaluate the extent of the disease because the region of metastases shows high 18F-FDG uptake. 19 In this study, 5 patients underwent 18F-FDG-PET/CT at diagnosis, and 4 patients had metastases on imaging owing to a higher SUVmax.
Considering the lack of specific imaging features, histopathological examination remains to be the only precise diagnostic tool available. A tumor diagnosed as CDC should meet the 6 criteria proposed by the International Society of Urological Pathology. 20 It is highly significant to different CDC from other tumors that occur in the renal medulla, such as UTUC, renal medullary carcinoma, and type 2 papillary RCC, which have remarkable overlapping morphological features with CDC. 21 Therefore, IHC is very important for excluding other diagnostic entities. A panel of PAX8/ PAX2, p63/p40, CK17/CK9, GATA-3, OCT3/4, INI-1, FH/2SC, 34be12, and ALK may help in the differential diagnosis between CDC and other diseases.9, 21 In the present study, a higher proportion of positive immunohistochemical staining was observed for Pax-8, CKpan, CK19, Vimentin, E-cad, and P504s; and a higher proportion of negative immunohistochemical staining was observed for RCC, CD10, CD117, CK7, CK20, Melan-A, GATA-3, CK5/6, P63, Cathepsin-K, TFE3, HMB-45, and Melan-A.
This study supports the aggressive nature of CDC, with a metastasis incidence of 73.9% at initial diagnosis. Twelve patients developed lymph node metastasis, and 7 patients had distant metastasis at diagnosis. Consistent with previous studies,22, 23 the lymph nodes, bones, adrenal glands, liver, and lungs were the most frequent distant metastasis sites. Studies found that advanced stage disease is an independent unfavorable prognostic factor for patients’ surviva.17, 24 Xie et al. found that 4 patients with lower-stage disease and smaller tumor size (T1aNxM0) survived longer than 10 years. 8 Other studies also reported similar findings.25, 26 In the present study, 2 patients survived for more than 4 years. Among them, 1 presented stage T1aN0M0, and the other had stage T2aN1M0. However, 1 patient with stage T1bN0M0 in this study survived for only 4 months. These results revealed that the prognosis outcomes vary even when CDC was identified at an early stage. As the previous study described, 7 our study confirmed that distant metastasis was an independent risk prognostic factor.
In the targeted therapy era, the role of cytoreductive nephrectomy (CN) in non-clear cell histology is a subject of ongoing debate.15, 21 A study of 286 patients with CDC showed that the median survival time of surgical patients was longer than that of nonsurgical patients, from 4 months to 24 months. 7 Radical nephrectomy is the standard treatment reported in most studies, whereas a few cases underwent partial nephrectomy.27, 28 CN may be the only potentially curable option for localized tumor. 7 In our study, all patients underwent surgery. Interestingly, 3 patients underwent nephroureterectomy for the preoperative diagnosis of UTUC.
Considering the histological similarity between UTUC and CDC, the latter may be sensitive to chemotherapy used for urothelial cancer. Rizzo et al 29 recently published the results of a retrospective analysis of 36 metastatic CDCs treated, as a matter of daily clinical practice, with cisplatin-gemcitabine or cisplatin-gemcitabine-paclitaxel at 3 large Italian institutions. Disease control rate was 47.2%, median progression-free survival (PFS) was 6 months, while median OS was 8 months. In a prospective study that recruited 23 patients with metastatic CDC, the patients were treated with 6 cycles of chemotherapy (gemcitabine and platinum salt), the median PFS, objective response rate and OS were 7.1 months, 26%, and 10.5 months, respectively. 30 These real-world experiences confirmed the modest activity of cisplatin-based chemotherapy for the treatment of CDC. In our study, gemcitabine combined with cisplatin was the most common regimen for CDC. Considering that the genetic characteristics of CDC and UTUC are different, the chemotherapy regimens used for UTUC may not be the best for CDC, 31 and new regimens should be investigated based on the features of CDC.
Consistent with previous studies, 24 our study showed that the 1-year OS rate was 43.5%, and the median OS was 12 months. In a cohort of 21 cases reported by the Mayo Clinic, the 1-year OS rate was 62%, and the median OS was 1.5 years. 8 The lower survival estimate compared to other reports may be attributed to the higher proportion of patients with higher tumor stages in our group.
Several studies have identified the benefits of targeted therapy for metastatic ccRCC; however, evidence regarding the use of these drugs in CDC is limited and mainly comes from retrospective data or case reports. In a study 32 of 13 patients with CDC treated with targeted therapies (temsirolimus [n = 2], sorafenib [n = 7], sunitinib [n = 3], and pazopanib [n = 1]), the overall disease control and median OS were 23% and 4 months, respectively. The disease control time of the patients ranged from 6 months to 33 months. Procopio et al. 33 reported the overall positive results of the prospective BONSAI phase II study in which 23 patients were treated with single-agent cabozantinib. The objective response rate was 35%, median PFS was 4 months and median OS was 7 months. In our study, 4 patients received targeted therapy, 2 patients were treated with sunitinib, 1 patient with sorafenib, and 1 patient with apatinib; the OS time was in the range of 8 to 52 months.
Although the present study provided considerable information on CDC, it has several limitations. First, it is a single-center retrospective study. Second, this study was retrospective in design, and power calculations were not conducted to estimate the required sample size. Finally, the sample size is small, patient selectivity and representativeness are poor, resulting in selective bias and reduced statistical efficiency. Further prospective studies are necessary to elucidate optimal treatment strategies to improve the survival of patients with CDC. Despite these limitations, this study could contribute to a better understanding of CDC.
Conclusions
This study presents a relatively large series of patients with CDC in a single center to investigate the characteristics of this rare subtype of RCC. In summary, CDC presents with a male predilection and occurs commonly in middle-aged people, most patients present an advanced tumor stage at diagnosis and die within 1 year after surgery. Its imaging and pathologic features overlap with other renal tumors and UTUC. Distant metastasis and no clinical symptoms at initial diagnosis were independent risk prognostic factors. Future larger studies are expected to better clarify the features of the rare renal tumor.
Footnotes
Abbreviations
Acknowledgements
The author(s) would like to thank Professor Yunlong Shi from the Nanjing University of Aeronautics and Astronautics for language editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 82072836).
Ethical Approval
This study was approved by the Ethics Committee of Jinling Hospital (2022NZKY-004-01) on January 21, 2022. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.