
Abstract
Introduction
In Europe, lung cancer is the second most common neoplasia in men (14%), just after prostate cancer, and the third in women (7%), second to breast cancer and colorectal cancer. In 2020, about 41.000 new lung cancer cases were estimated in Italy (27.550 in men and 13.300 in women). 1
The evidence of American Cancer Society in 2022 for lung cancer was of 236.740 new cases of lung cancer in males and 118.830 in females and 130.180 lung cancer deaths (68820 in males and 61.360 in females). 1
Over the years, thanks to the increasingly widespread use of imaging techniques, the detection rate of pulmonary nodules has been significantly improved.
The use of computed tomography (CT) and positron emission computed tomography (PET/CT) were considered the routine methods for evaluating pulmonary nodules. Compared to conventional imaging, PET/CT can evaluate not only the morphological characteristics of the lesion, but also the metabolic ones; the final step involves the histological evaluation.
Lung cancer as an entity includes several pathological categories, which must adopt different treatment strategies. Tumor sampling therefore represents a fundamental pillar in the diagnostic and therapeutic decision, especially in the era of personalized targeted therapy, where it is absolutely essential to obtain both the correct histological typing and the molecular profile of the neoplasia. The appropriate biopsy technique (open, transbronchial, or percutaneous) for tissue sampling depends on many different factors, the most important one is the location of the tumor.
In general, excisional surgical biopsies should be avoided whenever possible, due to the greater comorbidities and complications rate. Percutaneous approach is generally preferred for more peripheral lesions, while trans-bronchial techniques preferred for central and peri-hilar masses, which are more easily accessible via bronchoscopy. Imaging-guided percutaneous transthoracic biopsies are well-established procedures in lung cancer guidelines of all major international society.2, 3 In fact, percutaneous approach can provide optimal sampling, with excellent performance and low complication rates. 4
Percutaneous technique can be guided by several imaging modalities: ultrasound (US), fluoroscopy, CT, magnetic resonance (MRI), cone beam CT (CBCT) and PET/CT.
For years, CT fluoroscopy-guided biopsy has been widely accepted as an effective and safe biopsy method (with an accuracy greater than 90%). Currently, the most widespread guidance method is CBCT. 5
PET/CT guidance allows to optimize the bioptic efficiency of samples, because both morphological and metabolic information are considered, especially for large pulmonary lesions, usually characterized by inhomogeneous 18F-Fluorodeoxyglucose (FDG) uptake. However, this technique is both procedurally and economically highly demanding.6, 7
The purpose of this study is to evaluate the diagnostic value of fusion imaging (positron emission computed tomography - cone beam computed tomography [PET/CT-CBCT]) guided percutaneous biopsy, targeted to the maximum standardized uptake value SUVmax) and minimum standardized uptake value (SUVmin) of large lung lesions.
Materials and Methods
This retrospective STROBE compliant 8 observational and monocentric study has taken place at the Radiology Department of Circolo Hospital and Insubria University of Varese. Informed consent, including for scientific publication of anonymous data, was obtained by every patient who took part in the study. The procedures were performed in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its subsequent amendments and ethical standards.
Between May 2020 and April 2021, 10 consecutive patients were selected from a larger population of patients who underwent percutaneous transthoracic lung nodule biopsy. The clinical indication for biopsy was provided for all patients by our institute's thoracic oncology multidisciplinary board. Inclusion criteria were: age> 18 years; lung nodules diameter greater than 3 cm; availability of a 18F-Fluorodeoxyglucose (18F-FDG) PET/CT scan within 1 month before the procedure; signed informed consent for scientific publication of anonymous data.
Patients were then selected for follow-up or definitive treatment (surgery/chemotherapy/radiotherapy) based on MDT decisions and patient preferences.
The PET/CT examination involved a protocol of intravenous administration of 2.5 MBq/kg of 18F-FDG. Patients fasted for at least 4 to 6 h (glycaemia <180 mg/dL) before 18F-FDG administration.
After 60 min from the radiopharmaceutical administration, total-body acquisitions (from the orbito-meatal region to the middle third of the femurs) were performed, using 40 slides PET/CT equipment (Biograph mCT, Siemens Healthineers, Erlangen, Deutschland). For attenuation correction, a low-dose CT scan (120 kV and electric current intensity <100 mAs) was performed without IV contrast injection.
Both a qualitative and a semi-quantitative evaluation of the lesion consumption of 18F- FDG was carried out from the PET/CT images by a Nuclear Medicine Radiologist with 25 years of experience in PET imaging.
Semi-quantitative parameters were extrapolated, such as the standardized maximum and minimum absorption value, as well as SUVmax and SUVmin of the lesion.
Lung biopsies were performed at our Interventional Radiology Unit equipped with C-arm CBTC associated with Virtual Navigation Software (Allura Xper FD20, Philips Healthcare, Best, The Netherlands).
Specific techniques for the CBCT scan had already been presented. 9
The patient was placed on the angiosuite table taking account of the location of the lesion, accessibility, and distance from the cutaneous plane.
A first CBCT scan was performed for all patients in order to confirm and define the exact location of the lesion (centering CBCT).
PET/CT images were imported into the CBCT workstation and the low-dose CT image series of the PET/CT was superimposed over the centering CBCT using an automatic software and manual correction, throughout anatomical reference points (XperCT, Philips Healthcare, Best, The Netherlands).
Subsequently, PET images were loaded, to obtain a single fused PET/CT-CBCT image (Figures 1 and 2).

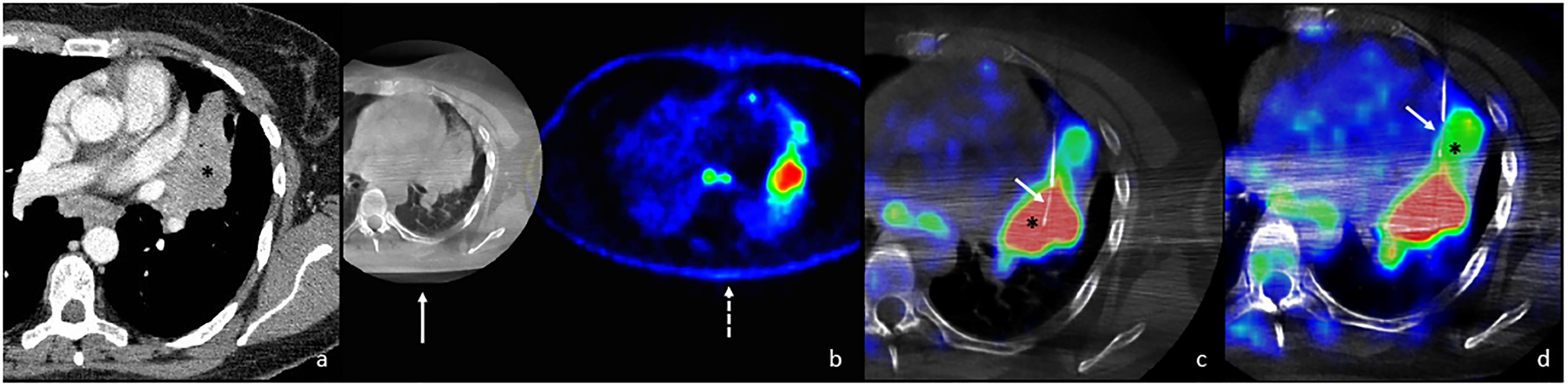
Male, 74 year-old. (a) AVGM sagittal arterial phase CT scan shows a voluminous left lower lung lobe neoplasm with shaded inhomogeneous contrast enhancement, the central portion enhances less (asterisk) than the periphery (white arrow). (b) XperGuide with PET-CT image fusion in “progression mode” demonstrates, the biopsy needle (arrow) with the tip embedded in the most distal area of the lesion (area with SUVmax 28.30—asterisk) where the first biopsy was done. The result of pathological anatomy was: small cell lung carcinoma, with about 80% neoplastic cells in the specimen and with possibility of biomolecular testing. (c) XperGuide with PET-CT image fusion in progression mode demonstrates, the needle retracted, along the Xperguide track (black arrow), with the tip in the area with SUV minimum 12.24 (head arrow) where the second biopsy was done. The result of pathological anatomy was: small cell lung carcinoma, with about 15% neoplastic cells in the specimen and no possibility of biomolecular testing.
Female, 46 year-old. (a) Axial venous phase CT scan shows a large left upper lung lobe neoplasm with inhomogeneous contrast enhancement (asterisk). (b) Image extrapolated from Xperguide workstation shows the fusion between the axial CBCT (white arrow) image obtained during biopsy preparation and the colorimetric PET-CT (dashed white arrow) scan to make the fusion of the 2 datasets. (c) XperGuide with PET-CT image fusion in “planning mode” demonstrates the biopsy needle (white arrow) with the tip embedded in the most distal area of the lesion (area with SUVmax 15,20—asterisk) where the first biopsy was done. The result of pathological anatomy was: adenocarcinoma, with about 20% neoplastic cells in the specimen and with possibility of biomolecular testing. (d) XperGuide with PET-CT image fusion in “planning mode” shows, the needle retracted (white arrow), with the tip in the area with SUV minimum 6.36 (asterisk) where the second biopsy was done. The result of pathological anatomy was: insufficient specimen and no possibility of biomolecular testing.
Angiography navigation software (XperGuide, Philips Healthcare, Best, The Netherlands) was used to correct the needle path. Fused PET/CT-CBCT images allowed to identify areas of the lesion richer in glucose-hungry cells and areas with low return consumption.
The needle path was overlapped with real-time fluoroscopy; therefore, fluoroscopy/CBCT/PET-CT needle navigation was possible.
A semi-automatic biopsy system with a 19 Gauge coaxial trocar (Speedybell, Biopsybell, Modena, Italy) was used for all procedures after skin disinfection and local anesthesia (10 cc of 2% mepivacaine, Angelini, Rome, Italy).
Intraprocedural CBCT was performed to check correct needle placement within the target lesion for all patients.
Patients were subjected to a double biopsy sample, respectively in the areas with high radio-glucose uptake (SUVmax) and low uptake (SUVmin). To obtain the 2 samples it was not necessary to reposition the needle by performing a new puncture at the skin level, but we proceeded by performing multiple cores by retracting the needle along its trajectory, possibly using a minimum “tilting” of the needle within the lesion itself. The needle and the trocar were then removed at the same time. A CBCT scan at the end of the procedure was acquired, to assess for any complications (areas of perilesional hemorrhagic effusion or pneumothorax).
The material collected was then sent to the Diagnostic Pathology Service for the histological analysis. The percentage of neoplastic cells, inflammatory cells, fibrosis, necrosis, or non-neoplastic lung parenchyma was evaluated. Furthermore, the possibility of carrying out immunochemical and molecular investigations to define the biomolecular profile of the tumor was analyzed on the 2 different tissue samples.
Data Analysis and Statistics
Technical success was defined as the completion of the biopsy procedure with histopathologic confirmation of the lesion (diagnostic rather than non-diagnostic samples, such as the presence of necrosis and fibrosis not allowing for histological diagnosis).
The possibility of performing immunohistochemical and molecular biology investigations was also compared on both SUVmax and SUVmin biopsy samples.
In those cases of histologic diagnosis of benignity at the biopsy procedure, a confirmation was obtained with patient's clinical and radiological follow-up.
Technical success and the possibility of performing immunohistochemical and molecular biology investigations were assessed by 2 × 2 contingency table and Fisher's test.
The concordance between biopsy and histological analysis of the surgical specimen was studied by Spearman’ Rho. SPSS version 25.0 (IBM, Armonk, New York, USA) was used for all statistical analyses. In all cases 2-tailed test were used. P-values were considered significant when <.05. Data collection was performed by informatic spreadsheet of anonymous data (Excel Microsoft Corporation).
Results
The lung lesions of the 10 patients included in the study showed the following morphological and metabolic characteristics (Table 1): mean axial diameter of 6.3 cm (range 3.3-13.3), mean SUVmax of 16.38 (range 6.6-28.3), and mean SUVmin of 7.9 (range 4.6-13.7). Of these 10 lung lesions, 9 were found to be malignant (5 adenocarcinomas, 2 squamous cell carcinomas, 1 small cell neuroendocrine carcinoma, 1 large cell neuroendocrine carcinoma), while one lesion was benign (inflammation).
Morphological and Metabolic Characteristics of the Lung Lesions Included in the Study.

Technical success was 100.0% (10/10 cases) in the SUVmax group and 70.0% (7/10 cases) in the SUVmin group: core material was too poor for analysis in 2 cases and amorphous in 1 case. Fisher exact test showed no statistically significant difference among the 2 groups (P-value: .2105).
Considering only the cases which tested positive for neoplasia (9 cases in the first group and 6 cases in the second group), the possibility of performing immunohistochemical and molecular biology investigations was achieved in the 100.0% (9/9) of cases in the SUVmax group and in the 33.3% (2/6) of cases in the SUVmin group. Fisher exact test showed a statistically significant difference among the 2 groups (P-value: .011).
For the validity of the study, the 2 cases of neuroendocrine tumor (neuroendocrine small cell carcinoma and neuroendocrine large cell carcinoma) whose histotype did not require a deepening of receptor study were also included in the evaluation.
The one case with no oncologic diagnosis (“inflammation”) underwent clinical and radiological follow-up. A CT scan at 3 months demonstrated complete regression of the lesion.
Table 2 compares the histological characteristics of SUVmax and SUVmin biopsy samples, in particular the presence, expressed as a percentage, of neoplastic cells, inflammation, fibrosis, necrosis, and normal lung parenchyma. The mean percentage of neoplastic cell was 37.22 ± 27.28 (mean ± standard deviation) in the SUVmax group and 9.29 ± 5.35 in the SUVmin group. Spearman’s rho was 0.71749 (P-value: .06949), indicating for a statistical significant difference among the 2 groups.
This table shows the pathological anatomy results for the samples taken in the maximum SUV zone (left macro column) and the minimum SUV zone (right macro column). The table shows that the percentage of neoplasia is much higher in the maximum SUV ( first left column ) vs those in the minimum SUV (sixth column ); moreover, in cases 1, 2 and 10 in the samples taken in the minimum SUV areas, a diagnosis could not be made. While in case 7 (which was found to be inflammatory process) the percentage of neoplastic tissue is zero and that of inflammatory tissue is 100 unlike the same samples in the area at minimal SUV where this difference is very blurred.

Abbreviation: SD, standard deviation.
Note that a >.05 P-value stands for a statistically significant difference (absence of correlation) among the investigated groups.
Discussion
PET/CT is now routinely assessed in diagnosis, staging and follow-up of lung neoplasms. It is also included among the guidelines of some cancers as a biopsy guidance. 10
The great contribution the functional/metabolic images of PET could offer during a biopsy procedure is the possibility to identify areas with a higher concentration of neoplastic cells and nowadays this tool is minimally exploited.
The use of PET/CT-CBCT fusion imaging in this field would allow to obtain a biopsy sampling with a better yield and, moreover, it would allow to minimize the number of sampling procedures with inconclusive results. In literature, diagnostic accuracy of percutaneous needle aspiration biopsy for small nodules reaches 74% for nodules ≤1.5 cm meaning for 26% biopsies have to be repeated. 11
Functional imaging using FDG is able to identify, inside large lung lesions, high uptaking areas which correspond to the highest concentration of pathological cells. 12
Precisely for this reason, interventional applications based on PET imaging have increased in the last decade and several studies have been published on the possibility of performing biopsies with the aid of PET-CT images. 8
In a study by Fanchon et al, taken on lesions localized in different anatomical districts, by means of autoradiographic samples, the proof of FDG absorption tests was shown to be adequate for a correct histological diagnosis of certainty. 13
The first works performed exclusively by simply viewing the pre-procedural PET/CT images in comparison with those CT or to the co-registration of the intraprocedural images, 14 making a qualitative comparison without a real fusion imaging. 15 Subsequently, software was used to record the preprocedural PET/CT data with intraprocedural imaging, usually CT 16 and moreover it was the use of a US/PET/CT image fusion system combined with an electromagnetic navigation device has been described. 17 More recently, some authors have tried to perform biopsy procedures using intraprocedural PET/CT images real time.18, 19 Radhakrishnan et al performed biopsies with PET/CT guide only using an automated robotic arm, obtaining a diagnostic efficacy equal to 100%. 20 Our paper instead exploits the fusion of PET/CT-CBTC images, as well as another unique study already present in the literature of Abi-jaoudeh et al who used a PET/TC-CBCT fused image system with a navigation software with an edition prior to ours. The results were already promising at the time. 21
Lastly, in a study by Fontana et al 2 groups of homogeneous patients were considered, subjected to 2 different guiding methods for biopsy procedures (CBCT and fusion of PET/CT with CBCT). All the results showed that percutaneous biopsies with fused PET/CT-CBCT images allow to reduce the number of inadequate samples. 5
Instead, what we have focused on in this work is to really demonstrate the reason why biopsies with PET/CT-CBCT fused images reduce the number of re-biopsies, making 2 biopsy samples in adjacent, morphologically indistinguishable areas, but with totally different histopathological results. This is because through PET/CT images we are able to differentiate areas metabolically active, rich in neoplastic cells compared to areas that have undergone necrosis or fibrosis, from which we would be able to obtain poor histological and biomolecular information.
The study performed on 10 lesions with inhomogeneous uptake on PET investigation subjected to double sampling with guided fused PET/TC-CBCT images, respectively at the level of the areas with maximum SUV and with minimum SUV, documented the presence of a greater number of tumor cells (9/10) or inflammatory (1/10) cells at the level of areas with maximum SUV, while in areas with minimum SUV necrosis and/or fibrosis prevailed. All the samples taken in the areas with maximum SUV led to a histological diagnosis instead, for the samples taken in the areas with low SUV in 3 cases it was not possible to obtain a diagnosis due to the presence of amorphous and/or scarce material. 22
The added value of the guide with fusion of PET/CT images in the execution of biopsies is therefore confirmed: by carrying out the sampling in the area of the lesion enhancing the radiopharmaceutical, there is a greater certainty of obtaining adequate material in order to formulate a histological diagnosis of certainty. Furthermore, our experience has shown—on a numerically small cohort—that despite being a frustule made up of an adequate quantity of tumor cells (at least 200 cells) it allows to carry out biology and molecular immunohistochemical studies (detailed histological diagnosis), searching for the mutations and the most frequently expressed antigens in non-small cell lung cancer (EGFR, ROS-1, ALK, and PD-L1), considered as predictive parameters of response to medical therapy.
Analyzing only the cases of neoplasia (9/10 and 6/10), it is possible to carry out molecular biology investigations in all the frustules from the areas with high SUV (9/9), while this is possible only on one part of the cases of withdrawals made in areas with minimum SUV (2/6); the difference between the results obtained in the 2 groups in this case turned out to be statistically significant (P = .011), thus confirming that in the areas with high SUV it is possible to find a greater number of neoplastic cells in the areas with low SUV, where fibrosis prevails/necrosis. However, it is necessary to consider some limitation of our study: first, it is a study on a few patients and although the results are statistically solid, they are applied to too small a number of patients; it is not a randomized trial; the follow-up in cases without surgery is rather short. Finally, the calculation and justification of the sample size wasn't performed.
Conclusion
In conclusion, the biopsy with fusion-imaging PET/CT-CBCT, in addition to being safe and feasible, has great potential, as it increases the detection rate and improves the effectiveness of the histological examination, reducing the number of inadequate or false negative samples.
Finally, it allows to carry out the biopsy sampling in the areas richest in neoplastic cells, thus obtaining more useful information for the planning of subsequent oncological treatments, more and more personalized for the individual patient.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
This work did not require ethics committee approval because for the application of an additional imaging system to an established procedure does not. In detail, at our Institution, in all large lesions, multiple biopsy samples are performed within the tumor mass to ensure a higher probability of a positive outcome. In the context of a larger study, we have begun to use fusion with PET-CT as a standard for thoracic lesions; over a period of about 2 years we performed all x-perguided biopsies with PET-CT fusion to evaluate whether it was necessary and beneficial to do so. This study has been previously published (Fontana F, Piacentino F, Ierardi AM, et al. Comparison Between CBCT and Fusion PET/CT-CBCT Guidance for Lung Biopsies. Cardiovasc Intervent Radiol. 2021;44(1):73-79. doi:10.1007/s00270-020-02613-3.). In this cohort of patients, in 10 cases, only functional imaging guidance was then applied to a standard practice for large thoracic masses, which specifically not changed in either the number of retrievals or the workup of large lung lesions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.