
Abstract
Introduction
Cancers of the breast are the most commonly diagnosed malignancies in women.1,2 Female breast cancer surpassed lung cancer in 2020 with an estimated 2.3 million new cases, accounting for 11.7% of all cancer cases. It is the fifth leading cause of cancer deaths worldwide, with 685,000 deaths. 2 The treatment of breast cancer varies according to stage. 3 The basic treatment methods are surgery, radiotherapy (RT), and chemotherapy/hormone therapy. 4 Advances in surgery and systemic therapy are gradually improving survival in breast cancer. 5 Lumpectomy (surgery to remove cancerous tissue from the breast) is usually performed on early stage breast cancer patients. Postoperative RT in the treatment of breast cancer has been shown to significantly reduce the risk of local recurrence and also improve long-term survival. 6
Postoperative whole-breast RT (WBRT) is the standard treatment for early stage breast cancer.7,8 For many years, conventional (2D) two open field tangential (2OFT) photon beams have been used as WBRT techniques in the world.9–11 This method caused late toxicities and poor cosmetic results due to unequal dose distribution.9,12 Especially in the left breast irradiation performed with this method, there was an increase in the doses of the heart and bilateral lung. In addition, it has been proven that the 2OFT techniques increase the risk of cardiac toxicity and morbidity moderately in left breast cancer. 13 Therefore, to reduce the side effects of WBRT, various RT techniques have been developed to improve the target dose and reduce the dose of organs at risk (OARs). 14
The three-dimensional conformal technique (3D-CRT) is a widely used RT technique for WBRT today. The development of 3D-CRT and the use of multileaf collimators (MLCs) have been successful in improving local control by increasing the possibility of shaping the treatment area to match the dose to the target volume. However, normal tissue toxicities remain a concern.15,16 The field-in-field (FIF) technique can be used as an alternative to 3D-CRT. In the FIF technique, beam orientations are similar to 3D-CRT, but instead of wedges, additional fields with manually created apertures are used for blocking. FIF technique has an important role in improving dose homogeneity and in obtaining fewer acute skin and soft tissue toxicities in the long term as well as a better cosmetic appearance of the treated breast. 9 Another frequently used technique is the intensity-modulated RT (IMRT) technique, which allows the user to modulate the intensity of each radiation beam. Each field used can have one or more high-intensity radiation fields and any number of lower-intensity radiation fields within the same field. Forward-planned IMRT (FP-IMRT) and inverse-planned IMRT (IP-IMRT) improved the target coverage while reducing the dose delivered to the lung, heart, and contralateral breast tissue.12,17,18
In recent years, advanced techniques, such as arc-based approaches, namely volumetric-modulated arc therapy (VMAT) and helical tomotherapy (HT) are spreading rapidly. VMAT is a dynamic form of IMRT that uses single or multi-arc rotating irradiation.19–21 VMAT is based on simultaneous optimization of MLC, gantry rotation, and dose rate. 22 Standard volumetric-modulated arc therapy (STD-VMAT), multiple arc VMAT (MA-VMAT), and non-coplanar VMAT (NC-VMAT) techniques improvedosimetry. 23 HT is actually a multi-field IMRT technique. HT has a rotating gantry accompanied by a couch-moving and high-speed dual collimator. 24 TomoDirect (TD) tomotherapy uses a fixed gantry angle instead of arc-based approaches. TD combines static gantry positions, concomitant couch translation and MLC modulation.25,26 Although photon therapy is the standard radiation therapy for breast cancer, proton RT (PRT) has become widespread nowadays due to its superiority in physical dose distribution. PRT represents a technique that allows dose reduction to structures beyond the target volume, depending on the properties of the proton particle. 14
Image-guided RT (IGRT) and deep inspiration breath holding (DIBH) techniques used with advanced technology are among the most indispensable for whole-breast irradiation. Daily MV- or kV-based IGRT is a method that takes target/organ motion into account and improves setup accuracy. With the IGRT feature, the margin of safety around the target volume is reduced, thus reducing the irradiated breast volume.27,28 DIBH technique allows for maximizing the distance between the target volume and the heart, reducing heart doses without sacrificing target coverage, or increasing the contralateral breast dose. 29
Some special techniques are also used to optimize plans in WBRT. Mayo et al. developed a new technique called hybrid-IMRT (H-IMRT) by combining conventional and IMRT fields for whole-breast irradiation. 30 The goal in hybrid RT is better homogeneous dose distribution, better target coverage, and better critical organ protection. 31 The hybrid-VMAT (H-VMAT) technique is a novel technique in which the majority of the dose is delivered to the target by conventional, static 3D-CRT fields, and the remainder by VMAT fields. 32 Another H-VMAT technique is a H-IMRT/VMAT technique that uses a simultaneously optimized algorithm combining IMRT with desired intensity modulation and VMAT with desired angular beam sampling. 33 Although different hybrid beam combinations are used in studies, in general, approximately two-thirds of the simultaneous dose is given from the static field and approximately one-third from IMRT or VMAT. 34 However, the optimal beam weight for hybrid RT plans remains uncertain. 35 This systematic review aims to present the dosimetric results of studies using hybrid techniques with other techniques in WBRT.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 36 The keywords “Dosimetric comparison of breast radiotherapy” or “Hybrid breast radiotherapy” or “Hybrid whole breast radiotherapy” or “Hybrid VMAT” and “Hybrid IMRT” were searched in different databases (PubMed, Scopus, and Web of Science). No language restrictions were applied in the selection of articles but there was a time restriction (between 2010 and 2021 years). Additionally, references were searched from the original articles obtained to identify eligible studies. Initially, 599 articles fulfilled the search criteria. By looking at the title and abstract of the article, duplicate articles and articles that did not match the research purpose were eliminated. Case reports, narrative reviews, editorial reports, abstracts, or conference proceedings were excluded from the study data and only original and published articles were included. The number of articles with available hybrid breast RT planning dosimetric data (planned target volume [PTV] and OARs parameters) was reduced to 54. Finally, 22 hybrid WBRT articles were selected and included in the systematic review. The search strategy has been shown in the PRISMA flow diagram (Figure 1).
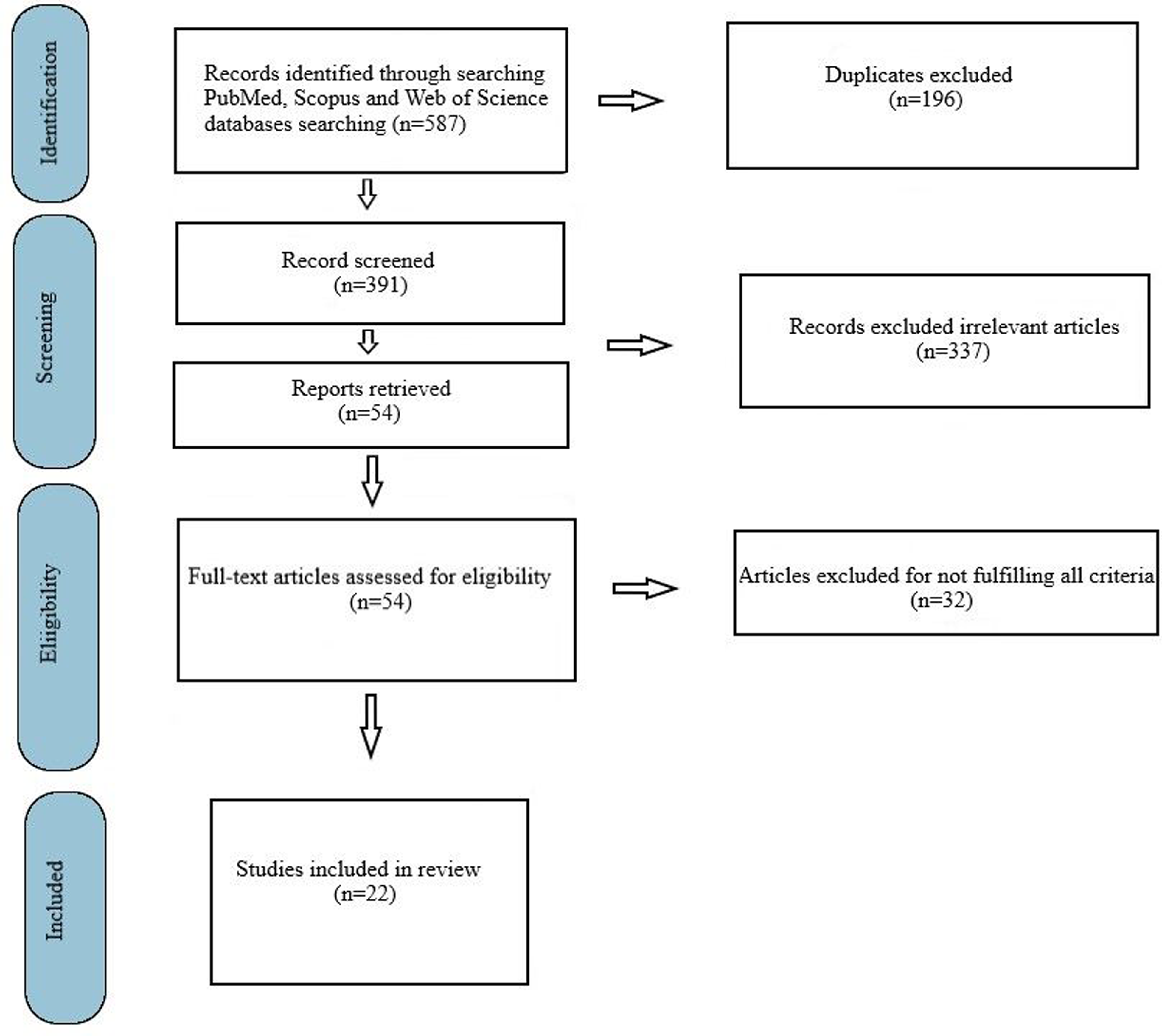
Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram for search criteria.
Results
After the screening, 22 potentially eligible articles were subjected to a detailed assessment. Dosimetric data of hybrid techniques along with different techniques are presented in Table 1. HI, CI, Dmean, or V95 values were included in the PTV values. V5, V20, V25, V30, or V40 values were presented for the ipsilateral or bilateral lung and the heart. Table 2 shows the country in which the articles in the research were made, the breast side, the defined dose (whether the simultaneous integrated boost [SIB] method was applied), hybrid beams contributed, monitor units (MU), time values, and key finding31,37–57
Dosimetric Results of Studies Using Hybrid and Other Radiotherapy (RT) Techniques in Whole-Breast Radiotherapy (WBRT).

Abbreviations: BL, bilateral; CI, conformity index; Dxx(%), dose incident on xx% structure volume; FIF, field in field; HI, homogeneity index; H-VMAT, hybrid VMAT; HT, helical tomotherapy; H-IMRT, hybrid IMRT; IL, ipsilateral; IMRT, intensity-modulated radiotherapy; PRT, proton radiotherapy; PTV, planning target volume; 2OFT, two open field tangential; 3D-CRT, three-dimensional conformal technique; VMAT, volumetric-modulated arc therapy; Vxx(%) Gy, % volume of structure receiving a dose of xx Gy.
Summary of Selected Clinical Studies That Have Reported on Whole-Breast Radiotherapy (WBRT) With Hybrid Techniques.

Abbreviations: BT, Bowtie; BTFFF, Bowtie flattening filter free; CP, conventional tangents; DT, delivery time; ETC, electronic tissue compensator; ECOMP, electronic tissue compensation; FP-IMRT, forward-planned IMRT; IMPT, intensity-modulated proton therapy; MU, monitor units; MA-VMAT: multiple arc VMAT; MSF, multistatic fields; NA, not available; NC-VMAT, non-coplanar VMAT; NCPA, non-continuous partial arc; OARs, organs at risk; PT, planning time; RT, radiotherapy; SIB, simultaneous integrated boost; SOC, standard of care; SP-IMRT, surface compensated IMRT; 2OFT, two open field tangential; 3D-CRT, three-dimensional conformal technique; TT, treatment time; TomoT, tomotherapy; T-2F, two coplanar fields; T-NC, two noncoplanar fields.
Discussion
To improve WBRT dosimetric results, it is necessary to increase within-target dose homogeneity, reduce off-target hotspots, and reduce doses delivered to the lungs, heart, and contralateral breast. By minimizing short-term and long-term complications, the local recurrence rate can be reduced and the survival rate can be increased in patients with breast cancer.30,58,59 In the majority of RT planning studies, the goal is to achieve even better dose distribution for treatment.
This systematic review provides an overview of the dosimetric results of commonly used techniques (2D/3D-RT, FIF, IMRT, VMAT, HT, TD, and PRT) and hybrid techniques (H-IMRT and H-VMAT) in WBRT. Most of the studies reviewed compare 2D/3D-CRT dosimetric results with other advanced RT technical results.31,39,40,42,43,46,48,50,52,55–57 Dosimetric results of treatment plans made with 2D/3D-CRT techniques are less competent than other techniques.31,39,42–44,46,57 While some of the studies stated that IMRT or FIF techniques provide better PTV homogeneity and OAR protection,38,40,48 some studies have demonstrated the superiority of VMAT techniques49,50 or tomotherapy techniques.41,59,60 In addition, it has been determined that PRT provides better dose homogeneity and OAR protection in breast RT.53,54
Especially in the past 10 years, clinicians have started to develop hybrid RT techniques to improve the quality of their treatment plans. The use of hybrid techniques was started for the first time in RT of breast cancer patients. 30 The reason for this was to minimize the irregularities in the dose distribution caused by the irregularity of the area in the breast. Using the hybrid technique, the advantages of the 2 RT techniques can be combined and promising results can be obtained.61,62 The hybrid RT results obtained indicate that the quality of treatment plans can be increased with the hybrid techniques used.10,61–65 Hybrid techniques are mostly created with the combination of 2D/3D-CRT + IMRT31,37–42,45–57 or 2D/3DCRT + VMAT 47,51,55,56 or IMRT + VMAT.42–44
Many studies show that the H-IMRT technique used in breast RT is dosimetrically superior.30,31,38–40,45,57,66–68 The dosimetric advantages of the H-VMAT technique have also been reported in many studies.42–44,47,49,55,68–70 Balaji et al. investigated the dosimetric advantages of H-IMRT (3D-CRT + IMRT) and H-VMAT (3D-CRT + VMAT) techniques and found that both techniques gave similar dosimetric results. 51 Chen et al. and Cilla et al. compared H-IMRT(3D-CRT + IMRT) and H-VMAT(3D-CRT + VMAT) plans, and they stated that H-VMAT plans provided superior dose distribution and homogeneity.47,55 Contrary to this Bi et al. compared H-IMRT (2OFT + IMRT) and H-VMAT (2OFT + VMAT) techniques and as a result, revealed that H-IMRT is the best treatment option. 71
The hybrid beam's contributing value for each patient may differ as the patient needs to be evaluated individually. PTV size and OAR placement play a vital role in selecting the optimal beam contributing weight. 69 Smith et al. showed the dosimetric results of H-IMRT plans made with different beam contribution ratios (80:20, 70:30, and 60:40). They discovered that the hybrid technique (70% 2OFT + 30% IMRT) provides dosimetrically superior dose compliance and homogeneity. 46 Similarly, in their H-VMAT RT study, Balaji et al. provided dosimetric results for various beam contribution ratios (90:10, 80:20, 70:30, 60:40, and 50:50). They found that the hybrid technique, consisting of 70% to 80% 2OFT + 20% to 30% VMAT sum, provided optimal dosimetric results. 68 According to Mayo et al., the hybrid plan requires less planning time and is independent of the planner's ability. 30 Xie et al. created an analysis of the cost of different RT methods for WBRT patients. The FIF technique was seen as the most cost-effective option, followed by the H-IMRT technique. 72
Different RT techniques used have different dose-shaping capabilities but almost every method has some advantages and disadvantages. The increased survival rate of breast cancer patients raises concerns about secondary cancers associated with low-dose radiation. 73 As the duration of treatment increases, patients’ discomfort during treatment may increase, and thus treatment uncertainty may arise.74,75 In addition, as the number of MU increases, the radiation dose affecting the whole body also increases. IMRT produces high MU in breast RT plans. The increase in the number of treatment fields used while making the treatment plan causes more normal tissue volume to receive radiation doses. Depending on the increase in low-dose exposure, the incidence of secondary cancers also increases.76,77 The study comparing IMRT with 3D-CRT revealed that the incidence of solid secondary cancers after IMRT could potentially increase compared to 3D-CRT. 76 Other studies have shown that the risk of secondary cancer in breast RT performed with the 3D-CRT technique is lower in the IMRT or VMAT techniques.19,77,78 Hacıislamoğlu et al. stated that the risk of developing secondary cancer in RT performed with the FIF technique in whole-breast irradiation is lower than that of IMRT and VMAT. 79 The disadvantage of tomotherapy is long treatment time with distress for the patient and risk of movement during RT. 41 VMAT provides a faster treatment time compared to other techniques.43,44,49 VMAT improves dose distribution by providing greater degrees of freedom in RT plans, but the low dose areas formed in OARs are of concern in terms of the risk of developing a second malignancy. 80 PRT offers dosimetric advantages in breast irradiation53,54 and a reduction in the rate of second cancer development, 81 but PRT is not common and is a very expensive technique.82,83
According to the volume of the heart exposed to radiation, there is an increase in cardiovascular diseases after left breast RT. 84 For this reason, it tried to reduce the heart dose as much as possible with the appropriate RT technique. Studies have shown that the heart dose of H-IMRT gives similar results to 2DRT, 3DCRT, and FIF. It was observed that the heart dose was higher in VMAT and IMRT plans compared to H-IMRT and 2DRT.32,39,57 In the study in which the dosimetric results of the H-IMRT and H-VMAT plans were presented, it was observed that the heart doses were similar. 52 In the comparison of H-IMRT and HT, it was observed that the heart dose of H-IMRT was lower. 41 When contralateral breast doses were examined, IMRT and VMAT doses were found to be higher than 3DCRT, H-IMRT, and H-VMAT.38,39,44,45,47,51
The main purpose of creating hybrid RT plans is to reduce the disadvantages of existing techniques. A well-doped hybrid beam scheme may be beneficial in reducing the risk of developing secondary cancer.49,68 Hybrid RT techniques, like other techniques, have some limitations. If the H-IMRT plan has a high MU, scattered radiation and hot dose areas outside the target may occur. 74 Because hybrid techniques are created by combining 2 RT plans, it is necessary to use 2 different quality assurance (QA) methods before starting the treatment. Loss of time may occur during QAs of hybrid treatment plans. This is an important issue that needs to be clarified for hybrid techniques. It will be useful to support the dosimetric results obtained from the hybrid methods used in WBRT with clinical results in the future.
Conclusions
The studies covered in this article provide a robust dataset for prospective hybrid WBRT. The dosimetric results of WBRT treatment plans using hybrid techniques are compared with other RT techniques and are exciting because they reveal superior aspects. Studies show that the rate of secondary cancer risk, which may be the result of applied RT techniques, is different. What factors contribute to the risk of secondary cancer formation can be further analyzed and discussed in the future. Hybrid RT is worthy of further investigation with new prospective protocols.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article