
Abstract
Introduction
Tubular breast carcinoma is a special type of breast cancer composed of distinct, well-differentiated tubular structures. It has a low incidence, accounting for 1% to 5% of all breast cancers.1-3 Tubular carcinomas (TCs) can be divided into pure and mixed types. According to the 2012 World Health Organization classification, pure tubular carcinoma (PTC) is diagnosed when a tubular formation is more than 90%. When the tubular formation is 50% to 90% and admixed with another histological subtype, the tumor should be regarded as a mixed TC (MTC). 4 Pathologically, differentiating PTC from MTC is vital, since it affects the prognosis and treatment. Previous studies have shown that TC has a better prognosis than grade I breast invasive ductal carcinoma (IDC).5-7 The nontubular component of MTC may affect lymph node metastasis, molecular classification, treatment, and prognosis of the tumor.
Previous studies have described TC as architectural distortion or an irregular mass with spiculated margins on mammography. 8 The tumor size is usually small and clinical palpation is often negative. Therefore, it is difficult to identify on traditional mammography, especially in dense breasts. Digital breast tomosynthesis (DBT) is a new three-dimensional technique based on digital mammography (DM) that is known to improve the detection rate and reduce the recall rate of breast cancer. 9 This technology reduces breast tissue overlap and may increase the frequency of detection of structural distortions.10,11 However, there has been no research on TCs.
The purpose of this study was to retrospectively analyze the mammographic features, clinicopathological features, and prognosis of TC, to deepen the understanding of PTC and MTC, and to provide a basis for the formulation of standardized and individualized clinical diagnosis and treatment.
Materials and Methods
Research Population
Clinical data of 25 patients with TC who were diagnosed and treated in our hospital from January 2011 to May 2019 were reviewed. All patients were followed up every 3 to 6 months up to 5 years after treatment and then annually or when clinically indicated. Preoperative mammography images of the patients were obtained using the picture archiving and communication system. Clinical information of patients including general information and pathological features was obtained from the medical record system. This study was approved by the Ethics Committee. Informed consent was waived due to the retrospective nature of the study.
Imaging Examination
Twenty-one patients underwent preoperative DM examination. Among these, 11 patients underwent additional DBT examinations. All DBT examinations were performed using the Selenia dimensions system (Hologic). Bilateral digital mammograms were obtained in 2 views (craniocaudal and mediolateral oblique). The images were reviewed by 3 radiologists with 5 to 10 years of experience in breast imaging. Mammographic findings were evaluated according to the 2013 edition of the Breast Imaging-Reporting and Data System lexicon. 12 The presence of a mass, the characteristics of the mass, architectural distortion, calcifications, location, and gland density were recorded.
Clinical Pathology
Clinical information, pathological features, and treatments were recorded, which included sex, age, clinical history, primary tumor size, TNM stage, histological tumor type, hormone receptor status, human epidermal growth factor receptor 2 (HER2) status, Ki-67 status, lymph node metastasis, type of surgery, use of chemotherapy, use of radiotherapy, and use of endocrine therapy.
TNM staging of all patients was reassessed according to the American Joint Committee on Cancer Staging System (seventh edition). HER2 positivity was defined based on positive results in immunohistochemical staining (+ + +) or fluorescent in situ hybridization. Ki-67 ≥15% was considered positive and Ki-67 <15% was considered negative.
TCs were divided into 2 types: PTC was defined as a tumor with greater than 90% tubular structures. When tubular structures occupied 50% to 90% of the tumor and when other histological types were also observed, the tumor was classified as MTC.
Survival Analysis
The survival status and survival duration of patients were evaluated. The follow-up time was defined as the time from the date of treatment to death or the follow-up deadline. Overall survival (OS) was expressed as the number of months from the operation to the death or the last follow-up. Disease-free survival (DFS) was defined as the time from the date of treatment to the date of documented recurrence including locoregional recurrence (LRR) and/or distant metastasis. LRR was defined as a tumor arising in the treated breast or chest wall, ipsilateral axillary lymph nodes, ipsilateral internal mammary lymph nodes, or ipsilateral supraclavicular or subclavian area.
Statistical Analysis
IBM SPSS Statistics, version 23.0 (IBM Corp.) was used for all statistical analyses. Independent samples t-test or Mann–Whitney U-test was used for the analysis of continuous variables among baseline clinical characteristics. Categorical variables were analyzed using the chi-squared test and Fisher's exact test. The Kaplan–Meier method and log-rank test were used for the survival analysis. The primary endpoint of this study was OS and the secondary endpoints included DFS and LRR. A 2-sided P-value <.05 was considered statistically significant.
Results
Altogether, 25 patients with TC were enrolled in the study. Median age of the patients was 47 years (range: 33-81 years). The tumor was located on the left side in 13 cases and on the right side in 12 cases. The lesions were located in the outer upper quadrant (n = 17), inner upper quadrant (n = 3), inner lower quadrant (n = 2), upper 12 o’ clock region (n = 2), and central area (n = 1). Among the 25 TC cases, 15 were PTCs and 10 were MTCs. Among MTCs, 3 cases were complicated with ductal carcinoma in situ (DCIS), 6 with IDC, and 1 with invasive micropapillary carcinoma.
Imaging Findings
DM was performed in 21 patients, additional DBT was performed in 11 patients, and preoperative mammography was not performed in 4 patients. A total of 19 out of 21 TCs (90.5%) were visible on DM. One PTC and one MTC were not detected on mammography, but showed architectural distortion and the presence of a mass on DBT (Figure 1). Furthermore, both these patients had dense glands. Eleven out of 12 PTCs and all MTCs exhibited the presence of a mass and structural distortions on mammography and the differences between the groups were not significant (P = .373). In both the groups, a mass with a spiculated margin was more common (12 of 13) and only one PTC showed an oval mass with an obscured margin. Seven out of 21 TCs were accompanied by microcalcification and the difference was not statistically significant between the groups. The results of mammography findings are presented in Table 1.
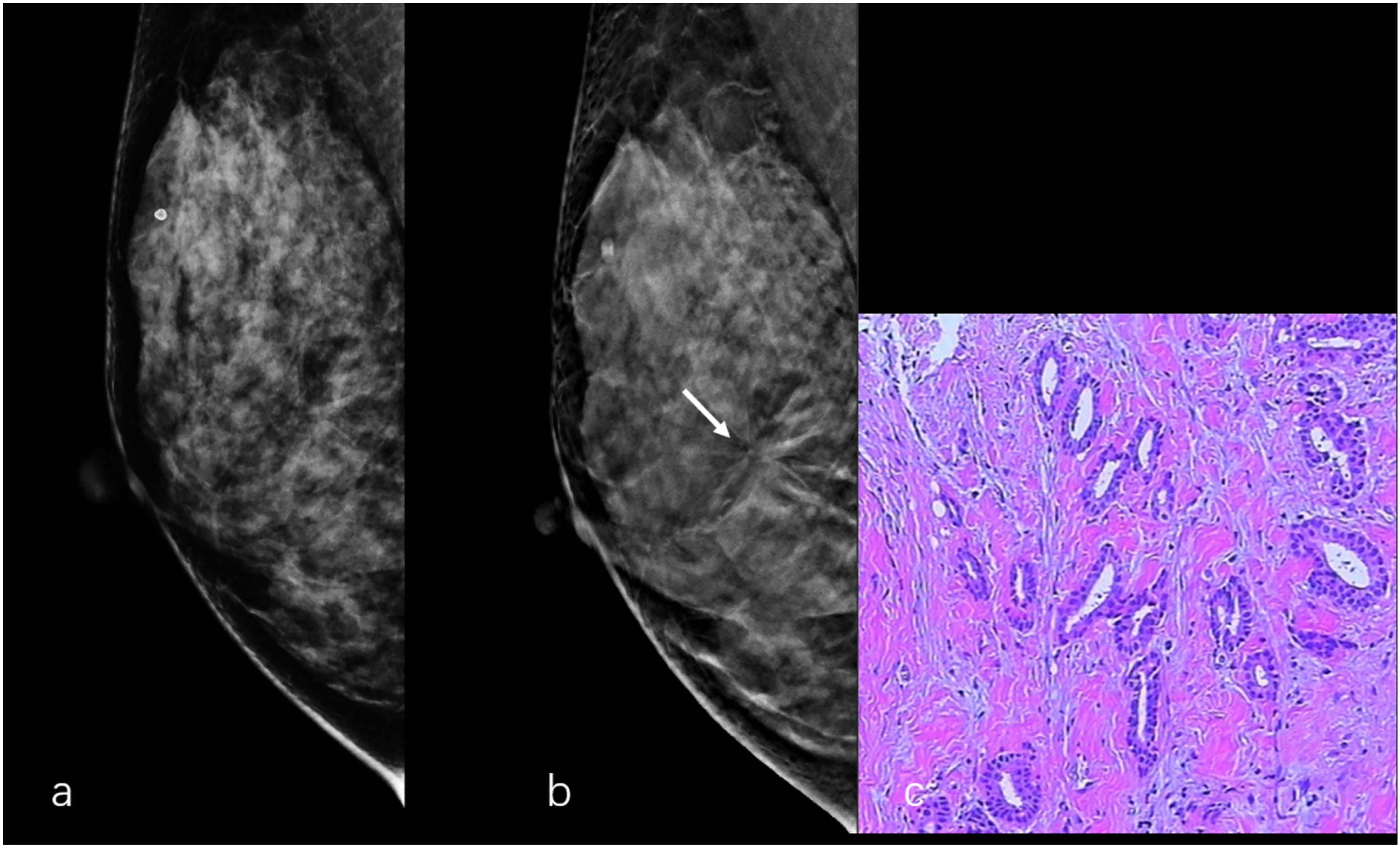
A 50-year-old female with tubular carcinoma of the right breast (a) Digital mammography in RMLO view shows negative findings. (b) Digital breast tomosynthesis in the RMLO view demonstrates architectural distortion (arrow). (c) The pathological result is PTC, the picture shows tubular structures (HE, 20 ×).
Comparison of the Mammographic Features of Pure and Mixed Tubular Carcinomas.

Abbreviations: PTC, pure tubular carcinoma; MTC, mixed tubular carcinoma.
The cases with the presence of a mass on mammography (n = 13).
Clinicopathological Features
The clinicopathological features of the 25 TCs are presented in Table 2. The average age of patients in the PTC and MTC groups was 46 (36-56) years and 49 (33-81) years, respectively. The tumor size ranged from 0.5 to 5.2 cm and the average size was 1.21 ± 0.92 cm. The PTC group had a smaller tumor size compared to the MTC group (P = 0.033). The PTC group had no lymph node metastasis, while 50% of the patients with MTC had sentinel or axillary lymph node metastasis (P = .005). Among the 25 TCs, 24 were estrogen receptor-positive and 22 were progesterone receptor-positive. The expression rates of ER and PR in the PTC group were 100% and those in the MTC group were 90% and 70%, respectively. Only one MTC showed HER2 overexpression. Altogether, 16 patients from the 2 groups exhibited lower expression of Ki-67 and the difference between the groups was not statistically significant.
Clinicopathological Characteristics of the 2 Groups.

Abbreviations: PTC, pure tubular carcinoma; MTC, mixed tubular carcinoma; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2.
Treatments
Breast surgery included breast-conserving surgery (BCS) or mastectomy and axillary surgery included sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND). Two patients with PTC and one patient with MTC (with DCIS) underwent BCS and SLNB. The remaining 22 patients underwent mastectomy and ALND. Patients in the MTC group received more postoperative radiotherapy than those from the PTC group, but the difference was not significant (P = .052). Most of the patients including 11 patients with PTC and 8 patients with MTC received postoperative chemotherapy (P = 1.000). Seven patients with PTC and 5 patients with MTC were treated with endocrine therapy (P = 1.000) (Table 3).
Follow-Up and Prognosis
The median follow-up duration for all patients was 44.6 months (range: 10.1-104.4 months). No breast cancer-related deaths were reported and the OS rate was 100% in both the groups. Lung metastasis was observed in one case of MTC (with invasive micropapillary carcinoma) at month 54 of the follow-up. There was no local recurrence in both the groups. There was no significant difference in DFS between the groups (P = .264) (Figure 2). The 5-year DFS rates in the PTC and MTC groups were 100% and 75%, respectively.

Disease-free survival of the pure tubular carcinoma group (n = 15) and the mixed tubular carcinoma group (n = 10).
Treatment Characteristics of the 2 Groups.

Abbreviations: PTC, pure tubular carcinoma; MTC, mixed tubular carcinoma; BCS, breast-conserving surgery; SLNB, sentinel lymph node biopsy; ALND, axillary lymph node dissection.
Discussion
TC is a type of invasive breast cancer with an incidence of less than 2%. It is considered to have a good prognosis and can be used as an indication for BCS.5,13 However, not all TCs are pure. Mixed TCs are usually associated with other types of breast cancer, especially DCIS and IDC. 14 Due to the low incidence and high heterogeneity of MTC, very few studies have examined its clinical and biological characteristics and natural history. Our study retrospectively analyzed the clinicopathological characteristics of 25 patients with TC and found that MTC had a larger tumor size and was more prone to lymph node metastasis than PTC. There were no significant differences in other characteristics such as age and the expression of ER, PR, HER2, and Ki-67. Previous studies have demonstrated that most of the breast TCs are smaller than 2 cm.13-16 Our study also observed that PTCs were smaller than MTCs (P = .033). Most of the PTCs are less than 1.0 cm in size and T staging is T1a-T1b, while most of the MTCs are more extensive (larger than 1 cm). For TCs larger than 1 cm, the possibility of a mixed type should be considered.
TC often shows architectural distortion or an irregular mass with spiculated margins on mammography.8,17,18 In our study, 2 TCs were not detected on DM, but were visible on DBT. This may be due to the small size of the lesions and the dense breast tissue. Reportedly, DBT has apparent advantages in the detection of spiculated masses and architectural distortions.9-11 Thus, we assumed that DBT was superior to DM for the diagnosis of TC.
ER and PR status in breast cancer is an important index for determining the need for endocrine therapy. Previous studies have shown that TC usually has a higher ER/PR expression and lower HER2 overexpression.5,6,14-16 We found that the PR positivity rate in the PTC group was higher than that in the MTC group, but the difference was not statistically significant. On the other hand, both groups had a lower rate of HER2 overexpression and only one patient with MTC showed HER2 overexpression. Therefore, we speculate that breast cancer with TC components may respond to endocrine therapy, but not to Herceptin.
TC rarely presents with lymph node metastasis.5,14,19-24 Kader et al 21 compared TC and stage I IDC in the British Columbia Cancer Agency database and found that axillary lymph node involvement, lymph node metastasis rate, and local and systemic recurrence rates of TC were lower than those of stage I IDC. The authors suggested that patients with TC do not require routine ALND or systemic adjuvant treatment. However, some studies have shown that lymph node metastasis may occur even if the lesion is small, suggesting that axillary lymph node staging should be considered in all TC cases. 25 Another study reported that only 6% of the patients with PTC had axillary lymph node metastasis, while patients with MTC had an axillary lymph node metastasis rate of 29%. 20 In our study, no lymph node metastasis was observed in the PTC group, but more than half of the patients in the MTC group had lymph node metastasis and most of the tumors were smaller than 2 cm. Therefore, we suggest that sentinel lymph node biopsy should be performed instead of ALND in PTC patients. In contrast, ALND should be performed in patients with MTC even if the tumor is smaller than 2 cm.
The overall prognosis of the 2 groups was good, there were no tumor-related deaths, and the OS rate was 100%. One case of MTC had distant metastasis within 5 years, but there was no significant difference in DFS between the groups. Fritz et al 26 and Chen et al 27 reported that radiotherapy can improve the prognosis of patients. In our study, patients in the MTC group received more postoperative radiotherapy, which might be related to a good prognosis. However, in the MTC group, a patient with mixed invasive micropapillary carcinoma who had received postoperative radiotherapy had distant metastasis during the follow-up. Therefore, we speculated whether distant metastasis was related to composite components, but not to postoperative radiotherapy, since invasive micropapillary carcinoma is highly malignant and prone to lymph node and distant metastasis. Considering the small number of cases in our study, further research should be conducted to arrive at a definitive conclusion.
Our study has several limitations including its retrospective design and relatively small sample size. It was a single-center study, leading to a possibility of bias. Furthermore, follow-up duration was inadequate for some patients.
Conclusion
TC usually appears as a small, irregular spiculated mass on mammography and DBT may improve its detection. TC is a type of breast tumor with a low degree of malignancy, good prognosis, high survival rate, high ER and PR positivity rate, and low HER2 positivity rate. Due to the low rate of lymph node metastasis in PTC, sentinel lymph node biopsy is recommended instead of ALND to reduce postoperative complications. For MTC, ALND should be performed even if the lesion is smaller than 2 cm.
Supplemental Material
sj-docx-1-tct-10.1177_15330338211045198 - Supplemental material for Pure and Mixed Tubular Carcinoma of the Breast: Mammographic Features, Clinicopathological Characteristics and Prognostic Analysis
Supplemental material, sj-docx-1-tct-10.1177_15330338211045198 for Pure and Mixed Tubular Carcinoma of the Breast: Mammographic Features, Clinicopathological Characteristics and Prognostic Analysis by Chanjuan Wen, Weimin Xu, Genggeng Qin, Hui Zeng, Zilong He, Sina Wang, Zeyuan Xu, Mengwei Ma, Zhendong Luo and Weiguo Chen in Technology in Cancer Research & Treatment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Clinical Research Program of Nanfang Hospital, Southern Medical University (No. 2020CR010), and Natural Science Foundation of Guangdong Province, China (No. 2019A1515011168).
Ethical Approval
This study was approved by the Ethics Committee of Southern Medical University Nanfang Hospital (Lot: NFEC-2017-136).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.