
Abstract
Purpose:
Modern linear accelerators are equipped with cone beam computed tomography and robotic couches that can correct for errors in the translational (X, Y, Z) and rotational (α, β, γ) axes prior to treatment delivery. Here, we compared the positional accuracy of 2 cone beam registration approaches: (1) employing translational shifts only in 3 degrees of freedom (X, Y, Z), versus; (2) using translational-rotational shifts in 6 degrees of freedom (X, Y, Z, α, β, γ).
Methods:
This retrospective study examined 140 interfraction cone beam images from 20 patients with head and neck cancer treated with standard intensity-modulated radiation therapy. The cone beam images were matched to planning simulation scans in 3, then in 6 degrees of freedom, using the mandible, clivus, and C2 and C7 vertebrae as surrogate volumes. Statistical analyses included a generalized mixed model and was used to assess whether there were significant differences in acceptable registrations between the 2 correction methods.
Results:
The rates of improvement with corrections in 6 degrees of freedom for the mandible with a 5-mm expansion margin were 54.55% (P = .793), for the clivus 85.71% (P = .222), and for C7 87.50% (P = .015). There was a 100% increase in acceptability for the C2 vertebra within the 5-mm margin (P < .001). For the 3-mm expansion margin, the rates of improvement for the mandible, clivus, C2, and C7 were 63.16% (P = .070), 91.30% (P = .011), 84.21% (P = .027), and 76.92% (P < .001), respectively.
Conclusions:
Significant registration improvements with the use of rotational corrections with a 5-mm expansion margin are only seen in the C7 vertebra. At the 3-mm margin, significant improvements are found for the C2, C7, and clivus registrations, suggesting that intensity-modulated radiotherapy treatments for head and neck cancers with 3-mm planning target volume margins may benefit from corrections in 6 degrees of freedom.
Keywords
Introduction
Head and neck (H&N) cancers have been conventionally treated with 3-dimensional conformal radiotherapy, guided by electronic portal imaging. 1 These images displayed only a fraction of the information from the computed tomography (CT) simulation data set and thereby limited the quality of image registration. 1 Since the advent and implementation of cone beam computed tomography (CBCT) in radiation treatment delivery, treatment techniques have achieved greater conformality and dose escalation, such that intensity-modulated radiation therapy (IMRT) has now become a mainstay for treating H&N cancers. 2 Complementing the IMRT technique, the development of robotic treatment couches capable of rotational corrections yields the possibility of additional reproducibility when used in conjunction with current immobilization devices. 3 Corrections in 6 degrees of freedom (6-DoF) are commonly utilized for the purposes of small, highly conformal treatment volumes which are sensitive to changes in tissue depth and patient contour, such as in the case of stereotactic body radiotherapy). 4 –6 While the use of 6-DoF corrections would prove beneficial for the precise correction of patient positioning, it may not necessarily demonstrate a great impact on the dose distribution in the case of a small, spheroid target surrounded by a roughly uniform depth of tissue. 7 In contrast, typical H&N treatment volumes are elongated in the superior–inferior direction with the inclusion of the cervical lymph nodal chains, which tend to be unilaterally superficial. The displacement experienced with rotation is most amplified at the superior and inferior extremes, 7 suggesting that these treatments may be improved by rotational corrections.
Image-guided radiation therapy (IGRT) protocols involve using bony surrogate volumes in the treatment region, rather than registering the soft tissue targets directly. 1,8 –10 This approach is based on the reasonable assumption that the soft tissue volumes of interest do not deform relative to the bony surrogates. 9 Using bony surrogate volumes for image registration is preferable because the image contrast between soft tissue and bone is often superior to the contrast between different soft tissues. 10 Typical surrogates for the H&N region include the C2, C5, C7, and T1 vertebrae; the clivus, mandible, occipital bone, maxilla, suprasternal notch, and clavicular head. 8,9,11
The planning target volume (PTV) margin accounts for daily variations in setup positioning and intrafractional motion. The typical H&N PTV margin of 5 mm assumes a high degree of reproducibility and stability, achievable only by a well-struck balance between patient immobilization and comfort. 12 Thermoplastic masks are conventionally used to immobilize the head, neck, and shoulders for H&N IMRT treatments. Such masks offer a reasonable amount of immobilization provided that any anatomical changes between simulation and treatment are minimal 13 ; however, these masks are not able to account for anatomical changes over time due to weight loss, nor are they always adequate for patient fixation in the cases of lordosis or scoliosis. 14 With such long treatment volumes extending across a semirigid deformable anatomical region, it is common for only one sub-volume of the PTV to be successfully localized. 12 Furthermore, even with the use of thermoplastic masks, patients are still able to move inside the mask due to discomfort, 12 which significantly impacts conformal treatments which can last 15 minutes or longer, 15 as is often the case with step-and-shoot IMRT.
With such challenges in immobilization, reproducibility, and maintaining accuracy despite anatomical changes over time, still some institutions have demonstrated the safe treatment of H&N cancers with a reduced PTV margin of 3 mm. 2,16 This study aims to ascertain the benefit of including 6-DoF corrections in H&N IMRT treatments through the evaluation of registrations to bony surrogate volumes, using registration margins of 5 mm and 3 mm.
Methods and Materials
Following institutional review board approval, this retrospective study involved retrieving CBCT images and clinical data from 20 randomly selected radiotherapy patients; all patients had a pathologically confirmed diagnosis of squamous cell H&N cancer and were treated between June 2017 and August 2017. There were 10 cases of oropharyngeal cancer, 3 cases of cancers of the larynx, 3 of the oral cavity, 2 patients with cancers of the salivary gland, and 2 with nasopharyngeal cancer. Eleven patients had definitive chemoradiotherapy and 5 patients were treated with radiation alone, whereas 4 patients received postoperative radiation. A summary of patient and treatment characteristics is presented in Table 1.
Patient and Treatment Characteristics.
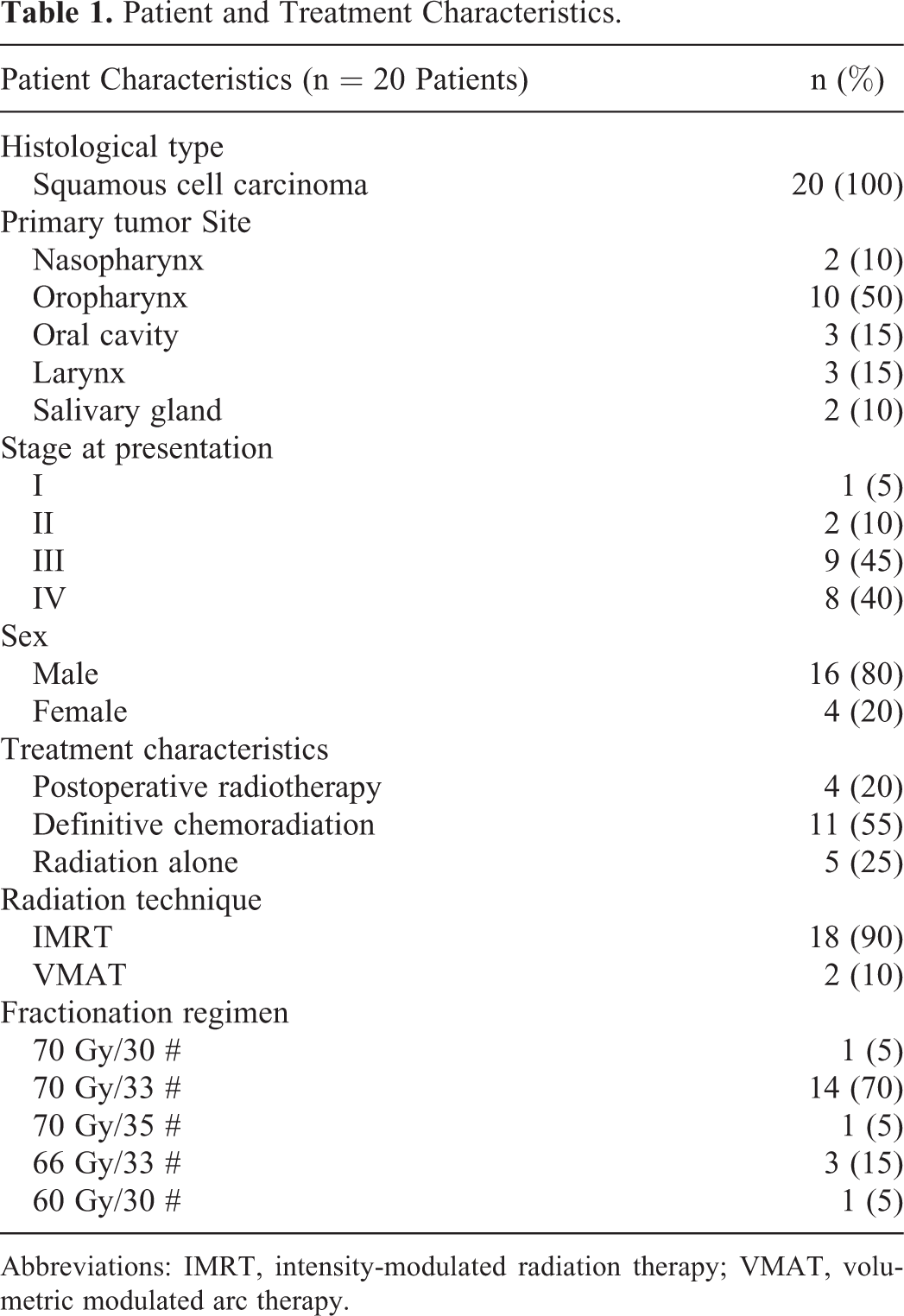
Abbreviations: IMRT, intensity-modulated radiation therapy; VMAT, volumetric modulated arc therapy.
All patients underwent CT-simulation using a Philips Brilliance 80 cm bore (Philips Healthcare Systems, Amsterdam, Netherlands). A 5-point thermoplastic mask (Orfit Industries, Wijnegem, Belgium) and, where appropriate, a custom-built mouthpiece, was used for patient positioning and immobilization. Helical scans were acquired at 1.5 mm increments with reconstructed slice thicknesses of 1.5 mm. Following simulation, treatment plans were generated using a Pinnacle treatment planning system, version 9.8 (Phillips, Amsterdam, the Netherlands). The gross target volume (GTV) was determined by the radiation oncologist based on physical examination or magnetic resonance imaging that was acquired at the time of staging and workup. A dosimetric plan was created to deliver 60 to 70 Gy to the GTV and 56 Gy to the nodal volumes using an IMRT or volumetric modulated arc therapy technique. A standard fractionation scheme was used; thus, patients were scheduled for 6 or 7 weeks of radiation treatment.
In this study, reference volumes in the H&N were contoured using the planning system, which included the following bony surrogate structures: the mandible, clivus, C2 vertebra, and C7 vertebra (Figure 1). These structures are commonly referenced for CBCT-image matching in H&N cases. An expansion margin of 3 mm and 5 mm was created for each volume. These volumes and margins were exported to the CBCT system and used for image analysis, with the assumption that registration analysis of an expansion margin around a valid surrogate volume will be analogous to the registration analysis of an equivalent PTV margin around an clinical target volume (CTV).

Bony surrogate structures were contoured in the treatment planning system for image analysis: (A) mandible, (B) clivus, (C) C2 vertebra, and (D) C7 vertebra. An expansion contour of 3 mm and 5 mm was generated for each structure to allow analysis (both margins shown).
Kilovoltage CBCT images were acquired on an Elekta Synergy XVI platform version 4.5.1 (Elekta Medical Systems, Stockholm, Sweden) as part of the patients’ usual standard of care. Each CBCT scan was acquired by a 200° counterclockwise-rotation protocol. Cone beam computed tomography characteristics included a volumetric reconstruction, slice thickness of 1 mm, and in-plane pixel resolution of 2 mm. For analysis, weekly CBCTs (ie, fractions 1, 6, 11, 16, 21, 26, and 31) were retrieved from each of the 20 patients in the study; the 30th fraction was taken instead of the 31st if the patient was prescribed only 30 fractions. Thus, 140 CBCTs were available for analysis.
All 140 CBCTs were registered offline and matched to the planning CT scans. The CBCT matching was achieved by manual adjustments made to exported registrations with incorporated shifts used for treatment; at the time of treatment, registrations in 3 degrees of freedom (3-DoF) were conducted using an automatic Chamfer algorithm with adjustments made by treating therapists. The positional accuracy in 3-DoF and 6-DoF was measured for each surrogate structure using a binary response distribution (ie, acceptable registration = 1; unacceptable registration = 0; Figure 2). An acceptable registration was defined as a volume match within a discreet displacement margin; firstly, constrained to a displacement <5 mm, then reevaluated with an alternative displacement constraint of <3 mm. The 3-DoF image registrations were initially evaluated by 1 to 2 radiation therapists at the time of treatment, and then further reviewed retrospectively by the study observer. Patients were not treated using 6-DoF corrections; the 6-DoF registrations were retrospectively performed by the same study observer. Data collection included the shift values (relative to the patient’s treatment position) obtained for all 140 CBCT registrations in 3-DoF and 6-DoF (mm, degrees), and the binary response value (0,1) for each registration. The analysis workflow is presented in Figure 3.

Transverse CBCT image of C7 vertebra. A, Transverse CBCT image of 3-DoF corrections showing unacceptable registration for the 3-mm expansion margin and acceptable registration for the 5-mm expansion margin of the C7 vertebra. B, Cone beam computed tomography image of 6-DoF corrections showing acceptable registrations for the 3-mm and 5-mm expansion margins of the C7 vertebra. CBCT indicates cone beam computed tomography; DoF, degrees of freedom.
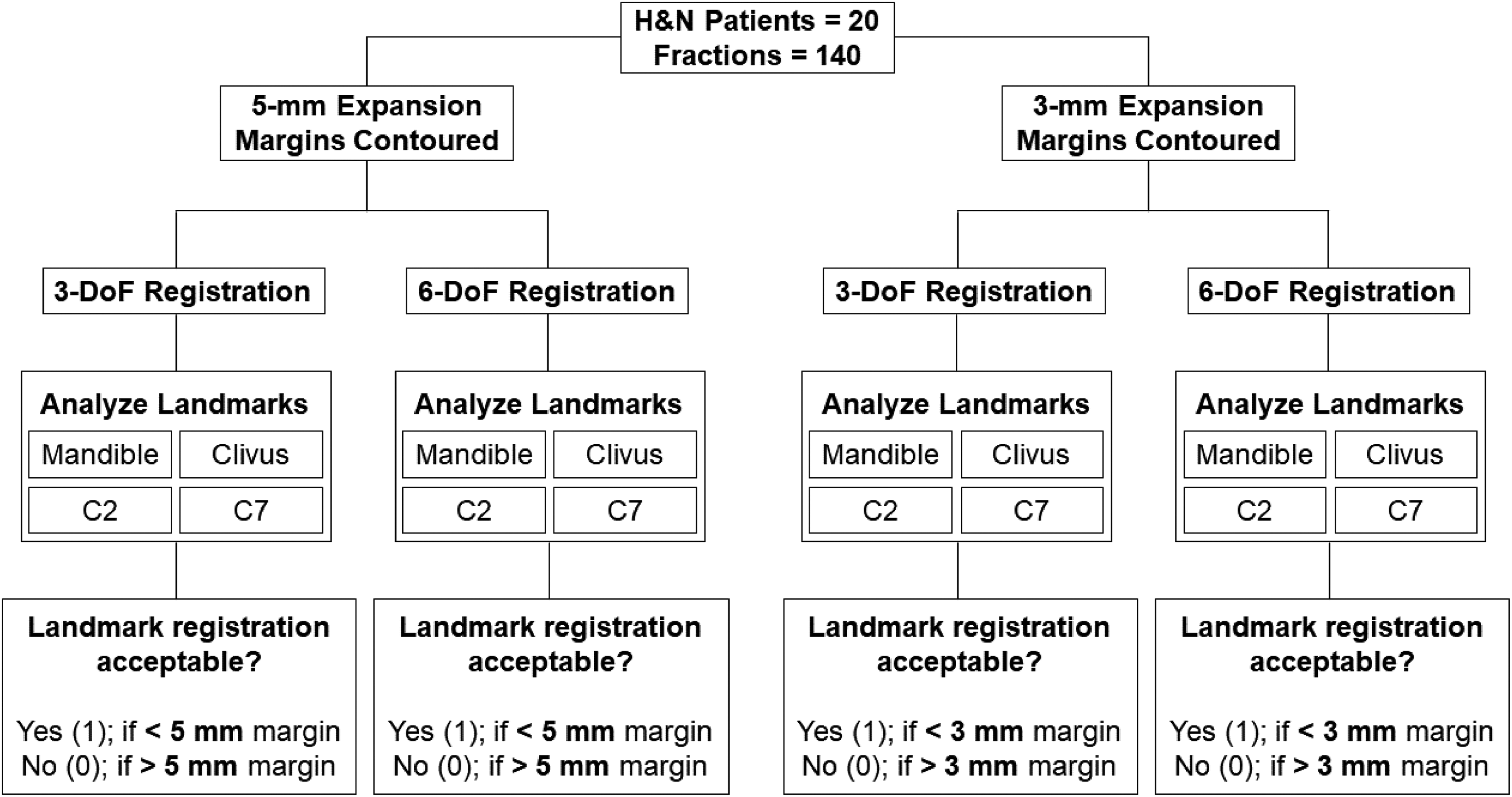
Cone beam computed tomography images from 7 weekly fractions were selected for each of 20 patients. The mandible, clivus, C2, and C7 landmarks were contoured on each patient’s CT simulation scan, and 5-mm expansion margins were generated for each landmark contour. Image registrations in 3-DoF were performed for all fractions, and the acceptability of each landmark was analyzed. Registrations in 6-DoF were performed for the same CBCT images; landmark acceptability was analyzed and compared to that of 3-DoF. The registrations and analyses were then all repeated with 3-mm expansion margins using the same selected CBCT images. CBCT indicates cone beam computed tomography; CT, computed tomography; DoF, degrees of freedom.
All statistical analyses were completed using SAS version 9.4 (2002-2012 SAS Institute, Inc, Cary, North Carolina). Descriptive statistics (mean, median, proportion) were used to describe the translational and rotational shifts in the image registration for each bone volume. Frequency tables (ie, data counts) and percentages were stratified by 3-mm and 5-mm margins for each bony structure. A generalized linear mixed model for the binary outcome improvements in registration accuracy accounted for the collinearity among the CBCT images within patients. This model was suitable as the data collected cannot be assumed to be statistically independent, nor can it be assumed to be normally distributed. 17 This model was used to assess whether there were significant differences in acceptable registrations using 3-DoF versus 6-DoF registrations and for each displacement constraint (3 mm versus 5 mm). Improvements in registration accuracies were reported as rates of improvement per surrogate volume. A 2-sided P value was used for statistical analyses, and a P value <.05 was considered to indicate a significantly different result.
Results
Registration Acceptability Across All Surrogate Volumes
The percentage of unacceptable registrations across all surrogate volumes with an expansion margin of 5 mm was 8% using 3-DoF corrections and 2% using 6-DoF corrections. This increased to 32% and 9%, respectively, for the registrations using the 3-mm uniform expansion margin.
A direct improvement in registration acceptability can be assessed by considering only the fractions containing surrogate volumes, which were unacceptably registered with 3-DoF corrections and were subsequently acceptably registered with the use of 6-DoF corrections. A reduction of 24% is seen in the average unacceptability across all surrogate volumes for the 3-mm margin, whereas the unacceptable registrations for the 5-mm margin are improved by only 7%. In both cases, the C7 vertebra shows the greatest improvement (43% of improved registrations for 3-mm and 15% of improved registrations for the 5-mm margin, on average across all fractions). The C2 vertebra demonstrated the least impact of the 6-DoF corrections, with reductions of only 11% and 3% in unacceptable registrations for the 3-mm and 5-mm margins, respectively.
Rates of Improvement With the Use of 6-DoF Corrections, Per Surrogate Volume
The rates of improvement (P value) with corrections in 6-DoF for the mandible with a 5-mm expansion margin were 54.55% (P = .793), for the clivus 85.71% (P = .222), and for the C7 vertebra 87.50% (P = .015). The Fisher exact test was used for the C2 vertebral registrations at the 5-mm expansion margin, as there were not enough data for the logistic regression function; this yielded a 100% increase in acceptable registrations with 6-DoF corrections (P < .001). In the case of the 3-mm expansion margin, the rates of improvement (P value) for the mandible, clivus, C2, and C7 were 63.16% (P = .070), 91.30% (P = .011), 84.21% (P = .027), and 76.92% (P < .001), respectively. Tables 2 and 3 summarize the results of the statistical analyses.
Summary of Statistical Analyses Yielding Rates of Improvement for Registrations Conducted With a 5-mm Expansion Margin.a

Abbreviations: DoF, degrees of freedom; NS, not significant.
an represents the total number of observed registrations which were unacceptable using 3-DoF corrections.
b P < .001.
c P < .050.
Summary of Statistical Analyses Yielding Rates of Improvement For Registrations Conducted With a 3-mm Expansion Margin.a

Abbreviations: DoF, degrees of freedom; NS, not significant.
an represents the total number of observed registrations which were unacceptable using 3-DoF corrections.
b P < .050.
c P < .001.
Discussion
In the treatment of H&N cancers, image guidance is an essential aspect of accurate and safe radiation delivery. The utilization of daily IGRT for H&N treatments is recommended, as target volumes in this site are often within millimeters of critical structures. 2,18 Furthermore, the optimization of daily image guidance protocols will be beneficial in reducing systematic setup errors. 19 This study sought to determine the efficacy of using 6-DoF corrections over 3-DoF corrections for H&N treatments, by comparing the registration accuracy of bony surrogate volumes at both 5-mm and 3-mm expansion margins. Rather than measuring the displacements of each surrogate volume, the registration acceptabilities were evaluated qualitatively using these clinically relevant margins to reflect treatment decision-making. This method demonstrates registrations as a result of a combination of rotations and translations, rather than translations alone, and is a method reflective of the IGRT protocols in place at our institution.
Improved registrations for the C7 vertebra were observed more frequently with 6-DoF corrections than the other surrogate volumes, as is to be expected for the structure at the greatest distance from the isocenter and is in an area where mask immobilization may be limited. It follows that the C2 and clivus were affected the least often by the 6-DoF corrections due to their proximity to the isocenter. The mandible showed the second greatest number of observed improved registrations for both margins, presumably due to the relatively deformable nature of the mandible relative to the skull and cervical spine. 14 This does not necessarily suggest that 6-DoF corrections are well suited for semirigid structures such as the mandible; rather, that there may have been a greater number of unacceptable mandible registrations with 3-DoF corrections since the mandible is not a prioritized matching structure in the treatment of laryngeal and most pharyngeal cancers. A similar study by Courneyea et al 12 showed that unacceptable registrations decreased from 15% to 4% using a 5-mm margin when rotational corrections were implemented; at a 3-mm margin, the unacceptability decreased from 49% to 21%. While the improvements per fraction were not tracked, these acceptability frequencies are still comparable to those found in this study.
The use of the 6-DoF corrections yielded statistically significant direct registration improvements for the C2, C7, and clivus volumes in the case of a 3-mm surrogate expansion margin; compared to only the C7 vertebral registration being significantly improved for the 5-mm margin. This was to be expected as narrower margins have higher demands for reproducibility. Though the rates of improvement for C7 at this wider margin are 7-fold, the volumes which are more representative of critical structures in close proximity to the chosen surrogates (namely the clivus and C2) are not significantly improved, suggesting that the implementation of 6-DoF corrections into the H&N IMRT workflow may not necessarily be worthwhile if treated with 5-mm PTVs.
Corrections in 6-DoF are performed by means of the tilting motion of a robotic treatment couch and do not allow for any nonrigid rotational motions, so any unacceptable registrations because of deformations of the H&N would not be improved with the use of 6-DoF. Furthermore, such tilting could potentially introduce patient drift within the thermoplastic mask, 3 potentially introducing an additional source of registration error. Gevaert et al demonstrated that the coverage became increasingly inadequate with increasing pitch and roll angle. 19 It is noteworthy to mention that linear accelerators are equipped to simulate corrections for yaw and roll rotations about the isocenter without the need for a robotic treatment couch. Yaw can be corrected by adjusting the couch isocentric angle, and roll can be corrected by adjusting the gantry angle, and both of these manual corrections do not involve any patient drift or tilt. 20 Perhaps these may be worthwhile considerations for changes to treatment protocol in the cases of patients who are set up with minimal pitch rotation errors.
In addition to having a dosimetric impact, weight loss during the course of treatment may result in systematic differences in setup positioning relative to the patient’s position during CT simulation, as well as increased intrafraction motion. 12 The use of 6-DoF corrections does not address intrafractional motion due to weight loss; however, improvements over 3-DoF corrections were demonstrated in our registration results from CBCT scans taken from throughout the patients’ courses of treatment. Yet, there was a 4% to 5% increase seen in unacceptable registrations of the 31st fraction compared to the first fraction. This suggests that the systematic weight loss–induced errors can be corrected in 6-DoF more effectively than in 3-DoF, but also that the effects of weight loss may still necessitate adaptive replanning despite the use of 6-DoF corrections.
The analysis of the registrations using margins of both 5 mm and 3 mm suggests that there may be implications of 6-DoF corrections aiding in H&N treatments using 3-mm PTV margins. To the best of our knowledge, there are only limited studies comparing the effects of IMRT treatments of H&N cancers using PTV margins of 5 mm and 3 mm. Chen et al compared 2 large cohorts of patients treated with H&N IMRT and concluded that there were no significant differences in 2-year locoregional control, nor in patient-reported toxicities between those treated using 3-mm and 5-mm PTV margins, even without any mention of using 6-DoF corrections for the 3-mm PTV treatments. 2 A retrospective analysis conducted by Caudell et al showed that using narrower margins did not result in an increase in local failure. 21 Most recently, Navran et al demonstrated that locoregional control could be maintained with a PTV margin of 3 mm, while reducing radiation toxicity and decreasing doses to organs at risk. 16
Our study was limited by its retrospective nature, in that it did not allow for the acquisition of verification CBCT scans to indicate any potential patient drift nor did it include posttreatment scans to measure intrafractional stability. Another limitation to the study was the relatively small cohort of patients. As it was demonstrated in the present study that corrections in 6-DoF are more beneficial with a 3-mm surrogate expansion margin, future research may be directed toward analyzing the dosimetric impact of patients treated with a PTV of 3 mm using 6-DoF corrections and the dosimetric consequences of any measurable patient drift.
Conclusion
The only significant registration improvement with the use of 6-DoF corrections with a 5-mm expansion margin is seen in the C7 vertebra. Significant improvements are found for the C2, C7, and clivus registrations with a 3-mm margin. This suggests that centers currently treating H&N cancers with 3-mm PTV margins may benefit from incorporating 6-DoF corrections into their IGRT protocols.
Footnotes
Authors’ Note
The study was approved by the Research Ethics Board of Sunnybrook Health Sciences Centre (approval number 434-2014). Informed consent was not required as the study is retrospective.
Acknowledgments
The authors would like to acknowledge Mr Stephen Russell, manager of the Division of Radiation Therapy at the Odette Cancer Centre, for his support of our research. The authors would like to acknowledge Darby Erler, clinical specialist radiation therapist at the Odette Cancer Centre, for her contribution in obtaining ethics approval for this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Arjun Sahgal has given past educational seminars with Elekta AB, Accuray Inc., and Varian medical systems. Arjun Sahgal is a member of the Elekta MR-Linac Research Consortium.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.