
Abstract
Purpose:
In this prospective phase II study, we investigated whether cone beam computed tomography scan was a superior method of image-guided radiotherapy relative to 2D orthogonal kilovoltage images in the post-radical prostatectomy setting.
Methods:
A total of 419 treatment fractions were included in this analysis. The shifts required to align the patient for each treatment were performed using 3D matching between cone beam computed tomography scans and the corresponding computed tomography images used for planning. This was compared with the shifts obtained from 2D orthogonal kilovoltage images, matching with the corresponding digitally reconstructed radiographs. Patients did not have fiducials inserted to assist with localization. Interfractional changes in the bladder and rectal volumes were subsequently measured on the cone beam computed tomography images for each fraction and compared to the shift differences between orthogonal kilovoltage and cone beam computed tomography scans. The proportion of treatment fractions with a shift difference exceeding the planning target volume of 7 mm, between orthogonal kilovoltage and cone beam computed tomography scans, was calculated.
Results:
The mean vertical, lateral, and longitudinal shifts resulted from 2D match between orthogonal kilovoltage images and corresponding digitally reconstructed radiographs were 0.353 cm (interquartile range: 0.1-0.5), 0.346 cm (interquartile range: 0.1-0.5), and 0.289 cm (interquartile range: 0.1-0.4), compared to 0.388 cm (interquartile range: 0.1-0.5), 0.342 cm (interquartile range: 0.1-0.5), and 0.291 cm (interquartile range: 0.1-0.4) obtained from 3D match between cone beam computed tomography and planning computed tomography scan, respectively. Our results show a significant difference between the kilovoltage and cone beam computed tomography shifts in the anterior–posterior direction (P = .01). The proportion of treatment fractions in which the differences in kilovoltage and cone beam computed tomography shifts between exceeded the 7 mm planning target volume margin was 6%, 2%, and 3% in the anterior–posterior, lateral, and superior–inferior directions, respectively.
Conclusion:
We prospectively demonstrated that the daily use of volumetric cone beam computed tomography for treatment localization in post-radical prostatectomy patients demonstrated an increased need for a shift in patient position. This suggests that in post-radical prostatectomy patients the daily cone beam computed tomography imaging improved localization of the prostate bed and may have prevented a limited number of geographic misses, compared to daily kilovoltage imaging that was not assisted with fiducials.
Introduction
Radical prostatectomy (RP) and radiotherapy (RT) are comparably efficacious and safe standard treatment options for localized prostate cancer. 1,2 Radical RT is commonly considered following RP in 2 different scenarios—the adjuvant and salvage settings. The adjuvant setting administers RT for undetectable disease due to high-risk pathologic features increasing the risk of relapse. 3,4 In contrast, salvage RT is provided when there is disease persistence or recurrence—typically represented by a prostate-specific antigen (PSA) level greater than 0.2 μg/L. 5 –7
A particular challenge in post-RP RT is accurately providing dose to the target, as organs at risk (OARs) may now occupy the RP’s surgical bed—the clinical target volume (CTV) of the radiation oncologist. 8,9 The interfractional changes in the size of bladder and rectum volume can significantly shift the CTV’s location, 10 –13 particularly at its superior aspect, 14 risking a geographic miss without careful planning. The stakes grow larger as post-RP RT studies explore hypofractionated RT and advocate for dose escalation. 15 –17 A geographic miss in either of these settings risks an intolerable therapy secondary to the larger dose. 18
Implementation of intensity-modulated radiotherapy (IMRT) has mitigated this challenge by increasing dose conformality. The steep dose gradients of IMRT minimize dose to OARs and reduce RT toxicity. 19,20 A disadvantage of tighter dose conformality is the increased possibility of a geographic miss. Issues with inadequate target localization have been demonstrated to result in undertreatment of the target and risk of the increased dose to the adjacent OARs. 21
Image-guided radiotherapy (IGRT) employs imaging to confirm the correct localization of the treatment target—the accuracy and precision required for safe IMRT. Combining IMRT with IGRT has allowed for dose escalation to the target volume with improved dosimetry and lower toxicity. 19,22 –24 Image-guided IMRT is now the recommended standard when treating prostate cancer. 25
Cone beam computed tomography (CBCT) is a commonly implemented and validated approach for IGRT post-RP. 26 Cone beam computed tomography allows direct visualization of anatomical landmarks surrounding the planning target volume (PTV). Technologists align the patient’s present position to closely match the position at the time of radiation treatment planning (ie, simulation). A common alternative is orthogonal kilovoltage (kV) imaging. For this approach, the patient’s position is verified by aligning the RP/surgical clips on the acquired kV images with clips on the digital reconstructed radiograph (DRR) from the planning CT data set. 27,28 In both cases, the surgical clips are fiducials to localize the PTV, but CBCT visualization allows for other anatomical landmarks to assist with localization. A larger PTV margin can account for any localization uncertainties instead, safely employing orthogonal kV imaging as the IGRT modality for post-RP RT at the cost of more dose to OARs.
This prospective phase II study compared 2 IGRT modalities in post-RP patients without implanted fiducials. The required shifts in patient position after image verification with orthogonal kV radiography and CBCT in the same patients were compared throughout their treatments. To increase the value in centers contemplating the transition from orthogonal kV imaging to CBCT, our methodology explored the relationship between an alternative rapidly assessable marker for changes in bladder and rectum size—the maximum diameter—in relation to the required shifts with either IGRT modality.
Methods
From December 2012 to October 2014, 26 post-RP prostate cancer patients treated with adjuvant or salvage RT were recruited for this prospective phase II study. This study was conducted as a quality assurance and therefore, was approved by the division of radiation oncology administration.
Patients who received adjuvant RT had a positive resection margin, extraprostatic extension (pT3a), or invasion of the seminal vesicle (pT3b). The patients who received salvage RT had a rising PSA level post-RP. Patients who did not have radiopaque surgical clips were excluded. For the radiation treatment, patients were simulated in a supine position, immobilized with Vac-Lok, and 2.5-mm thick CT images were obtained. Preparation for simulation and treatments included a full bladder and empty rectum.
The CTV was the prostate bed, contoured in accordance with RTOG guidelines. 29 Elective nodes were included in the CTV when indicated. The PTV was generated by expanding the CTV by 7 mm. Contoured OARs included the rectum, bladder, femoral heads, penile bulb, and small bowel.
The median prescribed dose was 66 Gy, delivered in 2 Gy per fraction (60-74 Gy in 2 Gy per fraction). Prior to each treatment fraction, patients were positioned with laser alignment into the treatment position via their localization tattoos. Then, 2 orthogonal kV images and a CBCT scan were obtained to determine the necessary shifts in patient position to align the planning PTV with the visualized patient anatomy at the time of the treatment. For the orthogonal kV radiographs, the specific surgical clips were contoured on CT data and used as a surrogate of the prostate bed. The shifts required to align and match the clips from the kV images to their corresponding DRRs were recorded but not used for treatment. The process was repeated by acquiring a CBCT scan and matching with the CT data set. The obtained shifts from the CBCT match were used to obtain the correct patient position prior to treatment. If the clips moved in separate directions or there was significant change in PTV position since simulation, alignment with soft tissue anatomy was utilized. For patients who required pelvic RT, the shifts for both orthogonal kV and CBCT methods were recorded only during the boost phase of the treatment. The shift values were recorded in the vertical (anterior–posterior), lateral, and longitudinal (superior–inferior) directions.
Data Analysis and Statistical Methods
The shift values obtained from orthogonal kV radiography images and from CBCT scans did not have a normal distribution. As such, they were compared with the Wilcoxon signed rank test. The null hypothesis was defined as the absence of a difference between the distribution in patient positional shifts between the 2 data sets—the required CBCT versus kV position shifts.
The bladder and rectum sizes were measured on the CBCT images in offline review (Eclipse; Varian) for each fraction. These dimensions were then compared with the baseline bladder and rectum sizes measured on the CT simulation scan. The maximum vertical, lateral, and longitudinal bladder dimensions were determined by measuring the distance between the most anterior to posterior, lateral to lateral, and superior to inferior extents, respectively. The surrogate volume was obtained by multiplying these cardinal dimensions. To determine the rectum size, the greatest rectal diameter on an axial cut, in proximity to the prostate bed, was identified. The surrogate rectal volume was obtained by multiplying the distance between the most anterior to posterior extents (vertical dimension) and the most lateral extents. We then computed the interfractional changes in volume size by subtracting the volume computed for each treatment fraction from the baseline and dividing the result over the baseline volume. The correlation between the bladder and rectum sizes with the shifts was analyzed with Spearman correlation test.
Results
We analyzed 419 treatment fractions in total, from 26 patients with post-RP prostate cancer, treated with either adjuvant or salvage RT. The mean absolute value of vertical, lateral, and longitudinal shifts obtained with orthogonal kV radiographs was 0.353 cm (interquartile range [IQR]: 0.1-0.5), 0.346 cm (IQR: 0.1-0.5), and 0.289 cm (IQR: 0.1-0.4), respectively, compared to 0.388 cm (IQR: 0.1-0.5), 0.342 cm (IQR: 0.1-0.5), and 0.291 cm (IQR: 0.1-0.4) obtained from volumetric CBCT scans. Our results show a significant difference between the vertical shifts obtained with orthogonal kV radiographs and those obtained from CBCT scans (P = .01). No significant difference was found in the lateral and longitudinal shifts (P = .949 and .833, respectively; Figure 1). The absolute value of the difference between the shifts measured with orthogonal kV radiographs and CBCT scans is shown in Figure 2. Once positioned via orthogonal kV on surgical clips and then adjusted based on CBCT, a vertical shift greater than 0.7 cm (the same as the PTV margin) was necessary in 27 (6.4%) of the 419 treatments. Although the difference in lateral and longitudinal shifts did not reach statistical significance, the number of treatment fractions in which the shift difference exceeded 0.7 cm was 10 (2.4%) and 13 (3.1%), respectively (Figure 2). For 42 (10%) fractions, the difference in at least one of the cardinal directions was over 0.7 cm.
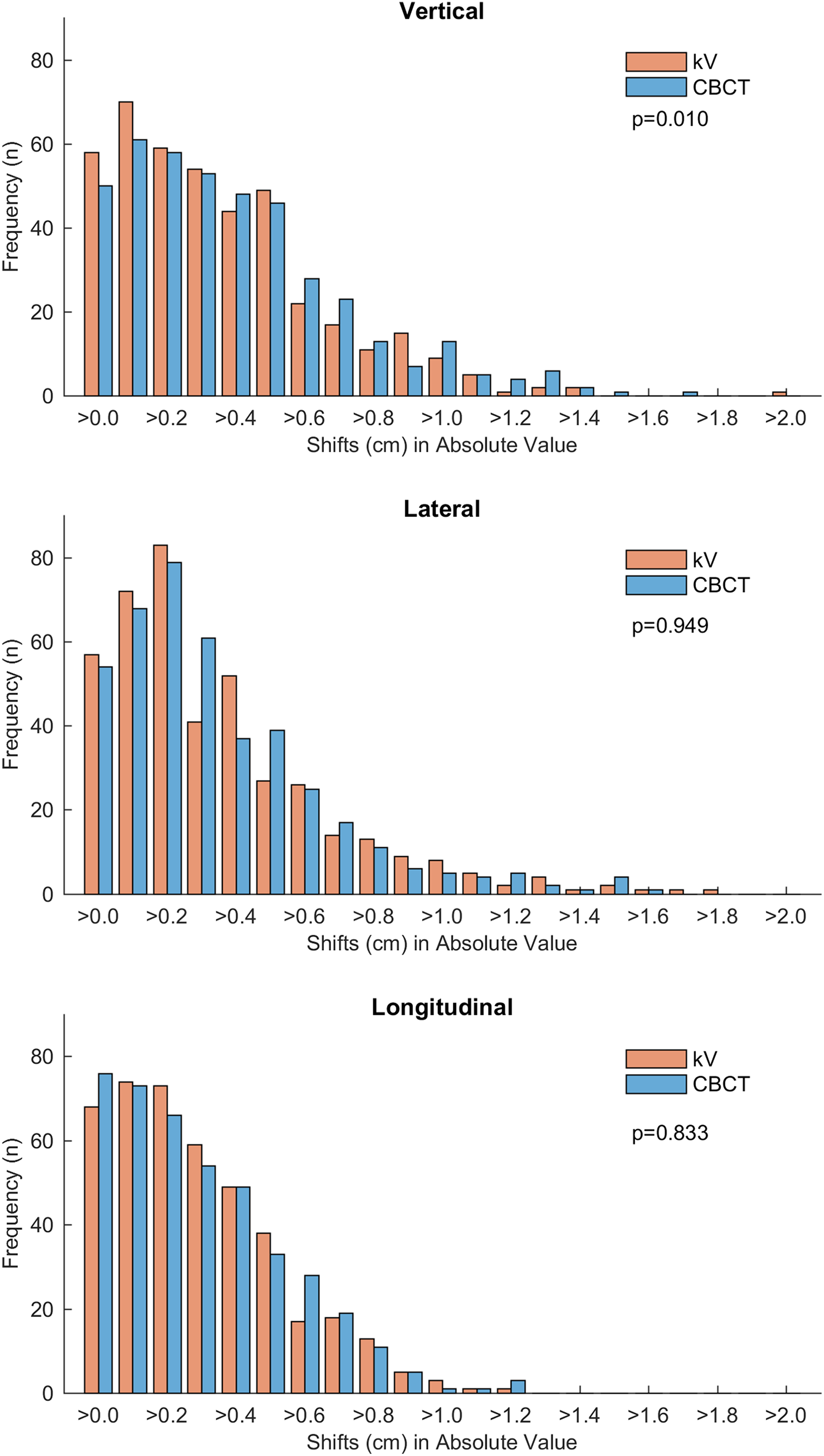
Histogram distribution of the KV and CBCT shifts in absolute value in the 3 cardinal directions (vertical, longitudinal, and lateral). The P values are shown. CBCT indicates cone beam computer tomography; PTV, planning target volume.

Histogram distribution of the absolute value of the difference between CBCT and kV shifts. The number of times the shifts (vertical, longitudinal, and lateral) differed by more than 0.7 cm (PTV margin) of the 419 treatment fractions is shown. The red dashed line indicates the 0.7 cm shift. CBCT indicates cone beam computer tomography; kV, kilovoltage; PTV, planning target volume.
Further analysis showed that the vertical and longitudinal shifts obtained from CBCT images were highly correlated with changes in the bladder (P < .001, ρ = −0.221 and P = .002, ρ = −0.148, respectively) and rectum size (P < .001, ρ = 0.209 and P < .001, ρ = −0.177, respectively). There was no correlation between CBCT lateral shifts and bladder (P = .054) or rectum sizes (P = .371). The kV vertical and longitudinal shifts were also correlated with the changes in bladder (P < .001, ρ = −0.204 and P = .01, ρ = −0.125 respectively), but not with the lateral shifts (P = .357). Interestingly, the direction in which the kV shifts correlated with the changes in rectal size were in the lateral (P = .017, ρ = −0.117) and longitudinal (P < .001, ρ = −0.177), but not in the vertical directions (P = .286; Figure 3).

Scatter plot showing the relationship between the kV and CBCT shifts and changes in the bladder volumes (top row) and rectum (bottom row) volumes in the 3 cardinal directions (vertical, longitudinal, and lateral). CBCT indicates cone beam computer tomography; kV, kilovoltage.
Discussion
Image-guided RT is crucial to reliably and tightly conform RT doses to their targets. Different published studies have described the potential locations of the prostate bed’s PTV, tracking its position throughout treatment and offering the insights as to whether the PTV was adequate. 30 –36 This information is of value because the PTV can be readily visualized with modern image-guided IMRT. 8,37,38 Options for daily image guidance include orthogonal kV radiographs, volumetric CBCT scans, or occasionally ultrasound. 39 –41 Cone beam computed tomography has required evidence of its advantages prior to implementation since it is more labor intensive for technologists, requires more physician input, and provides additional ionizing radiation to the patient.
In this study, patient treatment position was verified using orthogonal kV and CBCT scans. There were significant differences in the magnitude of the required positional shifts between the 2 modalities. However, a discussion of the results must consider how the imaging modalities’ outputs can be used to infer the position of the PTV. Numerous studies have described the use of anatomical landmarks, 12,33,42,43 surgical clips, 27,44 or fiducials 13,32,36 to assist with localization, albeit not in a comparative fashion. In our study, surgical clips that had remained in the prostate bed were contoured and used as reproducible marker of the PTV location. Studies have raised concerns with this approach as intrafraction positional variation in anatomical landmarks and clips can compromise prostate bed localization. 14,27,30,44,45
In comparison to the extensive literature on localization in patients with intact prostates, there is only one peer-reviewed study comparing image-guided techniques in post-RP patients. 46 One other related study compared alternative matching strategies in the significantly different post-RP setting. 28 Methodologically, our study uniquely contributes to the literature as it performed (1) a prospective study, (2) a comparison of planar kV versus CBCT image guidance when matching to any fiducial (implanted or clips), and (3) a comparison of planar kV versus volumetric CBCT guidance in the same post-RP patients. Simpson et al posed a similar question to our own. They retrospectively assessed 50 post-RP patients who had IGRT with either CBCT or kV planar imaging matched to the patient’s surgical clips. 46 Their study reported the required patient shifts and their primary clinical end point—toxicity. Acute toxicity was low and ultimately not different, despite that they also reported greater error and shifts with kV planar imaging. The limitations are the retrospective design and their comparison between different patients, as opposed to comparing the shifts required in the same patient (ie, the same clinical scenario).
Fortin et al retrospectively compared whether implanted fiducials versus surgical clips had greater changes in position between treatments or interobserver variability, when matching with planar kV images. 28 They found that fiducials had less interobserver variability and less migration. Caveats include the retrospective methodology, utilizing different observers from the treating technologists, and no statistical assessments to support their conclusions. There are additional post-RP studies that contrast the use of fiducials or surgical clips in contrast to anatomical landmarks (eg, matching to bone). 24,27,44 However, no other comparative post-RP studies compare image-guidance modalities or utilize CBCT in an evaluation of localization with surgical clips versus implanted fiducials.
Specific to our findings, the vertical shifts obtained from volumetric imaging are significantly different than the shifts from planar radiography imaging. It is important to appreciate that the absolute value of the difference between the CBCT and orthogonal kV radiography shifts exceeded the PTV margin of 0.7 cm for 10% of treatments. This reflects that the positioning of patient based on orthogonal kV images risked a partial geographic miss in 10% of fractions.
Cone beam computed tomography scans in this study appeared to show that the prostate bed moved posteriorly and inferiorly as the bladder fills and anteriorly and inferiorly as the rectum size increases. In other intact prostate studies, the variation in OAR size has been shown to affect the anterior–posterior (vertical) shifts. 14,47 This is also true for numerous other post-RP studies. 27,33 –35,44 –46 With kV IGRT, the relationship between the shifts with bladder size change is also similar. However, with the change in rectum size, it was the lateral and longitudinal kV shifts that showed a significant correlation. One can foresee a mechanism where changes in rectal volume would mechanically alter the position of the clips. The significant lateral shift bears further scrutiny though. Unlike our results, a change in rectal size should not preferentially displace them toward the left or the right (Figure 3).
Four potential situations could explain this finding: (1) technologists systematically picked a specific clip to localize to, (2) surgeons preferentially clip one side of the pelvic wall, though this was not observed in our images, (3) anatomical influences, such as the sigmoid folding inferiorly toward the CTV, or (4) large numbers of surgical clips, >10 surgical clips in some patients, complicating identification of the contoured clips that act as fiducials (Figure 4A). All hypotheses relate to the clips use as a surrogate of the tumor bed, which can be instead directly visualized with CBCT (Figure 4B). This also highlights a key limitation of the study. If patients had fiducials implanted, they may have had improved registration with kV planar imaging. This benefit could have reduced or even negated the benefit seemingly observed with CBCT.

An illustration of image-guided radiotherapy (IGRT) application. A, Anterior kV image of the patient acquired at the time of treatment prior to any shift, following alignment of the patient with external fiducial markers (tattoo) and laser localization only. The magenta, red, and the green lines depict the tumor bed, the PTV, and the clips contoured on the planning CT data set, respectively. The structures are overlaid on the anterior kV image to aid the technologist in measuring the shift necessary to place patient’s PTV into the treatment field. B, (Top) An axial slice of the patient acquired with CT. Red and green lines depict the contoured PTV and clips. (Bottom) The same axial slice acquired with CBCT at the time of treatment and after the desired match has been achieved. CBCT indicates cone beam computer tomography; kV, kilovoltage; PTV, planning target volume.
A separate methodological reason for the difference in shifts is the nonblinded aspect of our study. Since technologists were aware that the kV planar shifts were not going to be used, they may have committed less time to troubleshoot a difficult match—knowing that a CBCT was to follow. A more direct hypothesis is that CBCT simply better visualized soft tissues, providing more data to assist with localizing the PTV. In contrast, kV planar imaging’s limited contrast restricts matching to bony structures, clips, or implanted fiducials.
This study utilized a more rapidly assessable and different metric for daily evaluations of the bladder and rectum—the maximum diameter. Past works have demonstrated that the volume of these organs influences the safe minimum PTV expansion. 11 Alternative assessments are more time-consuming volume-based approaches, such as contouring the organs. Cone beam computed tomography’s increased sensitivity seemed to demonstrate that this rapidly implementable tool predicted for when the PTV could be out of position. Further validation of the use of the maximum diameters of the bladder and organ as a surrogate for their volume could facilitate expedited quality assurance during CBCT IGRT implementation.
This study has important limitations. First, it is a single-center phase II study of 26 patients. The sample size and experience of a single center innately predispose these results to systematic errors and bias. An example would include the nonblinded shifts performed by the technologists. Also, the absence of clinical data questions the significance of any setup or dosimetric relationships identified. These 2 limitations may direct the community toward collaborative studies in post-RP patients. Finally, our use of surgical clips as fiducials resonates with the issues identified by Fortin et al—clips may migrate and be less reliable than implanted fiducials in the post-RP patient. 28 Although our use of fiducials makes our work readily applicable to numerous centers that have appreciated the lack of prospective data mandating a shift to CBCT, it prevented us from concluding that our results are applicable in post-RP patients with implanted fiducials. If clips are inferior to implanted fiducials, then this study’s localization to clips may have exaggerated any differences between CBCT and kV planar image guidance.
The study presented herein fills an important niche. It prospectively demonstrated that CBCT image guidance in post-RP patients identified the need for more significant shifts in patient position than kV planar imaging. Directly comparing these shifts in the same patients minimized the potential for bias. Limiting the applicability of these data is the knowledge that the control arm, registration with kV planar imaging, could have been further improved with implanted fiducials. The absence of other prospective studies in this setting and the acknowledged limitations of this study highlight the need for additional prospective studies evaluating post-RP RT setup.
Conclusion
This prospective phase II study demonstrated that daily volumetric CBCT image guidance led technologists to introducing significantly greater changes in post-RP patient setup, in comparison to the use of planar kV imaging. However, this study’s methodology does not directly assess if nor prove that planar kV imaging was an inferior IGRT modality. An expanded study population at multiple centers, the use of surgical clips versus an implanted fiducial, and the inclusion of clinical end points are important factors to be explored in future studies. With the paucity of data directly applicable to this distinct setting, our data provide the strongest support to date that daily CBCT imaging improves treatment localization for post-RP IGRT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.