
Abstract
Objectives:
To assess the usefulness of dermoscopy in monitoring the treatment response and recurrence of actinic keratosis treated with 5-aminolaevulinic acid photodynamic therapy.
Methods:
In total, 35 patients with 75 actinic keratosis lesions were treated with 5-aminolaevulinic acid photodynamic therapy. The patients were divided randomly into 2 groups, dermoscopic group and the control group. Sixteen patients with 35 actinic keratosis lesions were treated with dermoscopic monitoring to determine the end point of the treatment. The remaining 19 patients with 40 skin lesions served as control and treated without dermoscopic monitoring and observed with naked eyes. At 1-year follow-up, patients were examined to look for the recurrence rate of the disease.
Results:
In the dermoscopic group, 1 (2.85%) of 35 actinic keratosis lesions showed recurrence of disease after 6 months of treatment. The recurrence was noted with red pseudo-network and scales at the treated site, whereas in the control group, 5 (12.5%) of 40 lesions showed recurrence.
Conclusions:
Dermoscopy can be a useful tool for monitoring the skin lesions in patients with actinic keratosis during photodynamic therapy and follow-up.
Introduction
Actinic keratoses (AKs) are considered precancerous lesions that may eventually progress to squamous cell carcinoma (SCC). 1 It occurs mostly in the elderly patients at exposed body parts, such as face, scalp, and dorsum of the hands. Actinic keratoses are characterized by red patches with scale which cannot be easily peeled off. 2 Topical 5-aminolaevulinic acid photodynamic therapy (ALA-PDT) is a widely approved therapy for AKs. 3 Actinic keratoses have high recurrence rates, especially in those with multiple lesions. It is reported up to 24% recurrence at 12-month follow-up in an open-label study with PDT. 4
Dermoscopy is a valuable and noninvasive technique that has been used for both diagnosing and evaluating the treatment response of many skin diseases, such as premalignant and malignant lesions, inflammatory, and infectious diseases. 5 It can visualize the morphological structures in the epidermis and papillary dermis which are not visible with naked eyes. Actinic keratoses have characteristic dermoscopic features which include scales, red pseudo-network, targetoid-like appearance, and rosette sign. 6,7 However, there was no report for monitoring the skin lesions in patients with AK during PDT and follow-up. In the present study, our aim is to evaluate the efficacy of ALA-PDT for AKs and to determine the end point of the treatment response and look for the recurrence rate.
Materials and Methods
Patients With Actinic Keratoses
Thirty-five patients were diagnosed with AK by histopathology in Shanghai Skin Disease Hospital from January 2015 to October 2016. The patients who had metastatic tumors, autoimmune diseases, or photosensitive diseases were excluded. The study was done with the patients’ informed consent and approved by the ethics committee of Shanghai Skin Disease Hospital.
Photodynamic Therapy
The skin lesions were prepared by gently removing the scale and being treated with plum-blossom needle (HWATO; Suzhou Medical Supplies Factory Co, Ltd, Suzhou, China) to enhance the absorption of photosensitizing agent. 8 Then, ALA (Shanghai Fudan Zhangjiang Biopharmaceutical Co, Ltd, Shanghai, China) was applied topically, and after 3 hours of incubation period, the lesions were irradiated with 100 J/cm2 of red light generated from a diode laser (635 nm; Omnilux, England) at 100 mW/cm2. The treatment was repeated for 2 to 4 sessions at 2-week interval. 9
Dermoscopy Monitoring
Polarized dermoscopic images were obtained with a dermoscope (Molemax; Derma Instruments, Vienna, Austria) attached to a digital camera (Canon, Japan). Analysis of each AK lesion was performed independently by 2 dermatologists, who are both having experience in dermoscopy.
Thirty-five skin lesions of 16 patients were treated with dermoscopy monitoring to determine the end point of the treatment. The remaining 19 patients with 40 skin lesions were selected for control. The control group was treated without dermoscopic monitoring by observing with naked eyes. All the lesions were evaluated with dermoscopy during follow-up at 1, 2, 3, 6, 9, and 12 months after the completion of treatment. Frequencies and changes in dermoscopic features and histopathological results before and after treatments were assessed.
Follow-Up and Recurrence Rate
Patients were followed up at 1, 2, 3, 6, 9, and 12 months after the treatment. Lesion size was measured. Photographs were taken and biopsies were performed if the lesion was likely reappeared with dermoscopy observation. A recurrence was defined as disease occurring after a complete response. Recurrence of AK was assessed by reappearance of dermoscopic features, such as local erythema, surface scale, or keratotic plugs, and skin biopsy confirmed the atypical keratinocytes.
Statistical Analysis
Statistical analysis was performed using the t test where P ≤ .05 was considered statistically significant. All data were computed using the SPSS version 15.0 statistical package (SPSS, Chicago, Illinois).
Results
Clinical Features of Patients
Thirty-five patients were included in this study (16 men and 19 women; age range, 58-97 years, mean 75.4 ± 10.8). A total of 75 lesions were examined in the study. The lesions were located on the face in 59 lesions, on the extremities in 16 lesions. Twelve patients had only 1 lesion but the others had multiple lesions. The lesion ranged from 0.5 cm × 0.5 cm to 2.5 cm × 3.0 cm. The clinical differential diagnoses were as follows: seborrheic dermatitis, psoriasis, Bowen disease, SCC, basal cell carcinoma, and malignant melanoma.
Dermoscopic Features
With the different dermoscopic features, AK lesions were divided into nonpigmented and pigmented AK. The most common dermoscopic findings were scales/keratin (86.6%), red pseudo-network (81.3%), targetoid-like appearance (69.3%), and rosette sign (41.3%; Figure 1). We observed that the dermoscopic features of pigmented AK were brownish to gray pseudo-network, annular granular structures, and multiple slate-gray-to-dark brown dots and globules. Linear wavy vessels were observed.

Clinical images of AK showing red patches. Dermoscopic images of AK showing scale, red pseuo-network, targetoid-like appearance (A) and rosette sign (B). AK denotes actinic keratosis.
Dermoscopic Monitoring AK Treatment With PDT
All the AK skin lesions were successfully treated by PDT. In the dermoscopic monitoring group, the treating end point was dependent on when there were no features of red pseudo-network, scales, targetoid-like appearance, and rosette sign by dermoscopy. Most of the clinical features disappeared with 2 to 3 times of PDT, but some dermoscopic features still remained, such as red pseudo-network and targetoid-like appearance. Eight patients with 11 lesions were presented with dermoscopic pseudo-network and targetoid-like appearance after 3 times of PDT. We treated the lesions once or twice more to achieve dermoscopic curation (Figures 2 and 3).

Clinical and dermoscopic monitoring of AK treated with PDT session. A, Dermoscopic features at baseline, progressive reduction in scale (B), pseuo-network (C), targetoid-like appearance, and rosette sign disappeared after 2 months of PDT (D). AK denotes actinic keratosis; PDT, photodynamic therapy.

Different treatment times according to dermoscopic monitoring AK lesions treated with PDT by dermoscopic monitoring, the treatment times ranged from 1 to 5 times (A), with naked eyes, the treatment times were mainly 3 times (B). AK denotes actinic keratosis; PDT, photodynamic therapy.
Follow-Up and Lower AK Recurrence Rate With Dermoscopic Monitoring
The follow-up period was 12 months. In 6 cases of 75 lesions, dermoscopic features, such as pseudo-network and surface scale reappeared (Figure 4). The features were entirely confirmed by histopathology following lesion biopsy. The total recurrence rate was 8% (6/75). In PDT with dermoscopic monitoring group, one lesion recurred after 6 months and the recurrence rate was 2.85% (1/35). In the control group, the recurrence rate was 12.5% (5/40). The recurrence rate was significantly lower in dermoscopic group (Figure 5).

Early detection of AK recurrence after PDT clinical and dermoscopic image at baseline (A), regression after twice PDT (B). Detection of recurrence (C) and successful retreatment after twice of PDT (D). AK denotes actinic keratosis; PDT, photodynamic therapy.
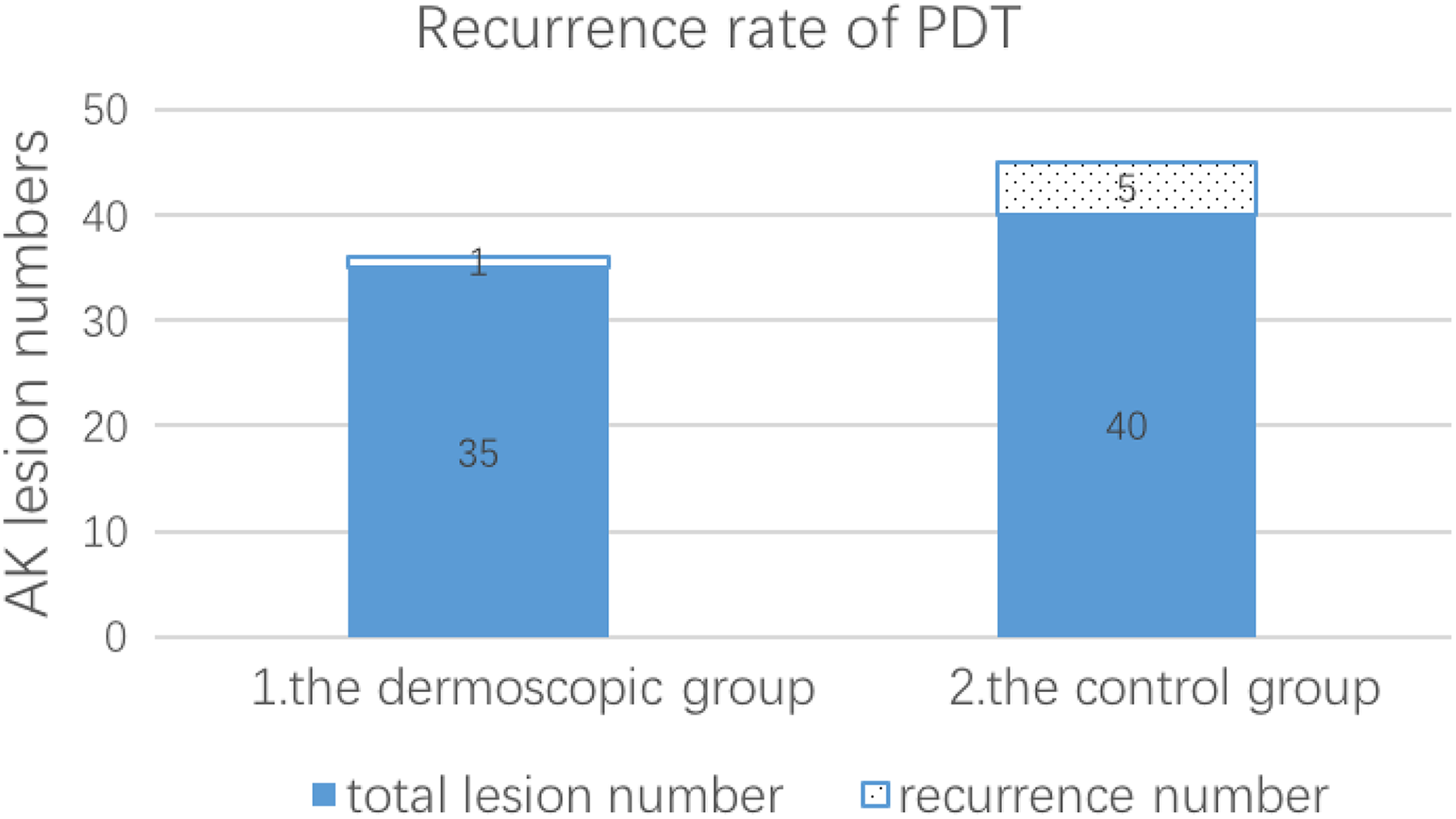
Recurrence rate of AK lesions treated with PDT after 12-month follow-up with dermoscopic monitoring, the recurrence rate 2.85% (1/35) was significantly lower than the controls 12.5% (5/40). AK denotes actinic keratosis; PDT, photodynamic therapy.
Discussion
Actinic keratosis is currently considered as a precancerous lesion. Patients with multiple AKs may have a 14% cumulative probability of developing SCC within 5 years. 10 Because of the high risk of potential cancer, early active treatment is necessary. Actinic keratosis treatment methods include cryotherapy, surgical resection, PDT, local drug therapy, chemical exfoliation, and other methods. 11,3 Photodynamic therapy is an emerging technique for the treatment of AK in recent years, especially for those who have multiple skin lesions in the face. 12
Dermoscopy is a noninvasive, simple, and inexpensive technique that improves diagnostic accuracy of dermatological diseases that are not visible to the naked eyes. Dermoscopy can make a link between macroscopic clinical dermatology and microscopic dermatopathology. 13 Yellow-white scales, red pseudo-network, targetoid hair follicle, and rosette sign were most frequently observed in AK. 14 In our study, scales and red pseudo-network were observed with similar frequency compared to the previous study. With the polarized dermoscopy, targetoid-like appearance and rosette sign were more frequent in our study compared to the previous.
Dermoscopy is not only a useful tool for diagnosing skin diseases but also helpful in monitoring the clinical response to treatment. 15 In this study, we used dermoscopy to monitor the AK treatment. Seventy-five AK lesions were treated with ALA-PDT (2-5 treatment times). Most patients seemed to be cured at 2 to 3 times of treatment, and the scaly and keratotic patches disappeared. We observed progressive reduction in surface scales and red pseudo-network after PDT by dermoscopy. However, with dermoscopy, we found 11 lesions of the 8 patients presented with pseudo-network and targetoid-like appearance when clinically remission. The characteristic dermoscopic features of AK remained after 3 times of PDT in this study. We then continued treating the lesions with PDT for another once (in 8 lesions) or twice (in 3 lesions) till the dermoscopic features vanished. For the AK lesions treated with PDT in dermoscopic group, the treatment times ranged from 1 to 5 times. While in the controls, the treatment times were mainly 3 times (Figure 3). It suggests that with dermoscopic monitoring, individualized treatment can be realized. The treating session can be adjusted to achieve the best therapeutic effect.
Besides the usefulness in disease diagnosis and therapeutic observation, dermoscopy is also very important in the monitor of early recurrence. After 1-year follow-up, 6 cases of the 75 lesions reappeared dermoscopic features, such as pseudo-network and scale, and the features were later confirmed by histopathology. Of the 6 recurrent lesions, only 1 lesion was in the dermoscopic group. It belongs to an old female patient who has multiple AKs on the face. The other 5 recurrent lesions were in the control group. All of them were treated with PDT for 3 times. The recurrence rate was significantly reduced with dermoscopic monitoring (Figure 5). The most probable cause is that subclinical lesions can be discovered with dermoscopy, so the disease can be prevented to progress and cured.
In conclusion, dermoscopy-assisted PDT for AK was more pronounced than the naked eye to determine the end point of treatment and the recurrence rate of AK was significantly decreased. With dermoscopic monitoring, we hope the treating session can be adjusted to achieve individualized treatment for the patients.
Footnotes
Authors’ Note
This study was approved by the Ethics Committee of Shanghai Skin Disease Hospital (approval no. 201503ke). All patients provided written informed consent prior to enrolment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant of the Joint Project of New Frontier Technology of Shanghai Shen-kang Hospital Development Center (SHDC12015123), and Scientific and Technological Innovation Projects of Shanghai in 2017 (17411952500).