
Abstract
Background:
Telehealth utilization patterns have been variably studied across diabetes, hyperlipidemia, and asthma settings. This study aims to evaluate telehealth patterns in these disease settings through the COVID-19 pandemic across age, gender, geography, and insurance dimensions.
Methods:
We identified patients with asthma, diabetes, or hyperlipidemia aged 18–64 with commercial or Medicaid insurance between 2017 and 2022 using Arkansas All-Payer Claims Database (APCD) data. The primary outcome variable was an indicator for any telehealth use. We plotted telehealth visits by quarter for each disease state by age, gender, rurality, and insurance strata. We also conducted linear regression analyses to associate telehealth use with each year relative to 2019 while controlling for patient characteristics.
Results:
Telehealth was seldom used pre-pandemic but sharply increased during the pandemic, reaching 11.8% in asthma, 9.1% in diabetes, and 9.0% in hyperlipidemia. Following the pandemic (2020–2022), females, urban residents, and younger patients were generally more likely to utilize telehealth. In adjusted analyses, relative to 2019, telehealth use sharply increased in 2020 between 12.7 and 15.1 percentage points (all p < 0.05) across the conditions. Utilization dipped in later years but remained much higher than prepandemic levels with the largest increases being among patients with asthma.
Conclusion:
These findings suggest that differences in telehealth adoption are not solely and uniformly attributable to observable patient characteristics but may also reflect structural and clinical factors particular to patient demographics and the specific disease setting. Ongoing efforts should support clinically-appropriate, even, and sustained access across groups.
Background
Telehealth is a potentially useful tool for managing chronic diseases. As a modality, it reduces the burden on patients by providing convenient care options, expands access, supports self-management, and facilitates care coordination, 1 including chronic condition management.2,3 During the COVID-19 pandemic, telehealth filled critical gaps in care continuity, 4 but its use has been uneven across race, ethnicity, and geography.5,6 For instance, in neurology settings, telehealth utilization patterns have varied by gender, 7 insurance,6,8,9 and age.6,10 Understanding demographic patterns of telehealth within chronic disease-specific clinical contexts can help to improve its future use.1,11
Telehealth use has been studied at varying levels and with varying effects across different chronic condition settings. Telehealth utilization in the diabetes setting has been associated with older patients and female patients 12 and has been linked to a higher likelihood of having hemoglobin A1c (HbA1c) in control.13–17 In contrast, in hyperlipidemia, one systematic review finds no differences between telehealth and lipid levels. 12 Patients with asthma who had severe exacerbations or outpatient visits were more likely to use telehealth during the pandemic. 18 One study finds that the majority of asthma patients with active electronic health records portals have messaged their providers electronically and have had a virtual visit, 19 while another systematic review article found that telehealth can improve adherence, symptom control, and quality of life. 20
The potential evenness of telehealth benefits depend on its utilization patterns across demographic groups. This study seeks to add to the literature on the three aforementioned chronic conditions—diabetes, hyperlipidemia, and asthma—by evaluating patterns of telehealth use before and during the pandemic along four demographic stratifications: age, gender, rurality, and insurance. We studied this question among patients in Arkansas, a predominantly rural state with significant barriers to health care access. Around 40% of the population lives in rural areas, 21 and the state ranks 48th in state health system performance nationally. 22 This study informs how telehealth may help fill gaps in care and address longstanding access barriers that contribute to health care disparities across the state.
METHODS
DATA
We analyzed 2017–2022 data from the Arkansas All-Payer Claims Database (APCD), focusing on patients with asthma, diabetes, and hyperlipidemia who are aged 18–64 with commercial or Medicaid insurance. We examined outpatient provider visits among claims associated with these chronic conditions, which were identified using International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes (Supplementary Appendix A). Evaluation and Management (E&M) visits were identified using Current Procedural Terminology codes 99201–99205 and 99211–99215, and telehealth visits were identified by Place of Service (POS) code 02 or modifiers GT or 95.
Data were aggregated at the patient-quarter level. All models excluded observations with missing ZIP codes, which accounted for <1% of any given sample. Our final analytic sample included 73,164 patient-quarters in asthma, 40,403 patient-quarters in diabetes, and 63,069 patient-quarters in hyperlipidemia. The primary outcome was a dichotomous variable indicating any telehealth use in the quarter. Sample stratifications include age category (age 18–44 vs. 45–64), gender (male vs. female), rurality (rural vs. urban), and insurance status (commercial vs. Medicaid). Patients were classified as rural residents if they lived in a county with a Rural-Urban Commuting Area code >3.
ANALYSES
First, we plotted the proportion of patients with any telehealth visits by quarter to characterize the patterns of uptake over time. Chi-squared tests assessed differences across stratifications for the pre-pandemic era (January 2017–February 2020) and pandemic era (March 2020–December 2022). Analyses were examined by chronic disease diagnosis and across age, gender, rurality, and insurance strata.
We then estimated adjusted associations between calendar year, patient characteristics, and telehealth use using linear probability models. Separate models were estimated for patients with asthma only, diabetes only, and hyperlipidemia only. The dependent variable was an indicator for any telehealth use in a given patient-quarter. Independent variables included calendar year indicators (with 2019 as the reference year), gender, age group (18–44 vs. 45–64), race (Black vs. White, controlling for other non-White groups), insurance type (Medicaid vs. commercial), and rural residence. Standard errors were clustered at the ZIP-code level to account for geographic correlation. Regression results are reported as percentage-point changes in the probability of telehealth use and are presented in Table 1 . This study was determined to be nonhuman subjects research by the University of Arkansas for Medical Sciences Institutional Review Board.
Adjusted Associations between Calendar Year, Patient Characteristics, Telehealth Use by Condition
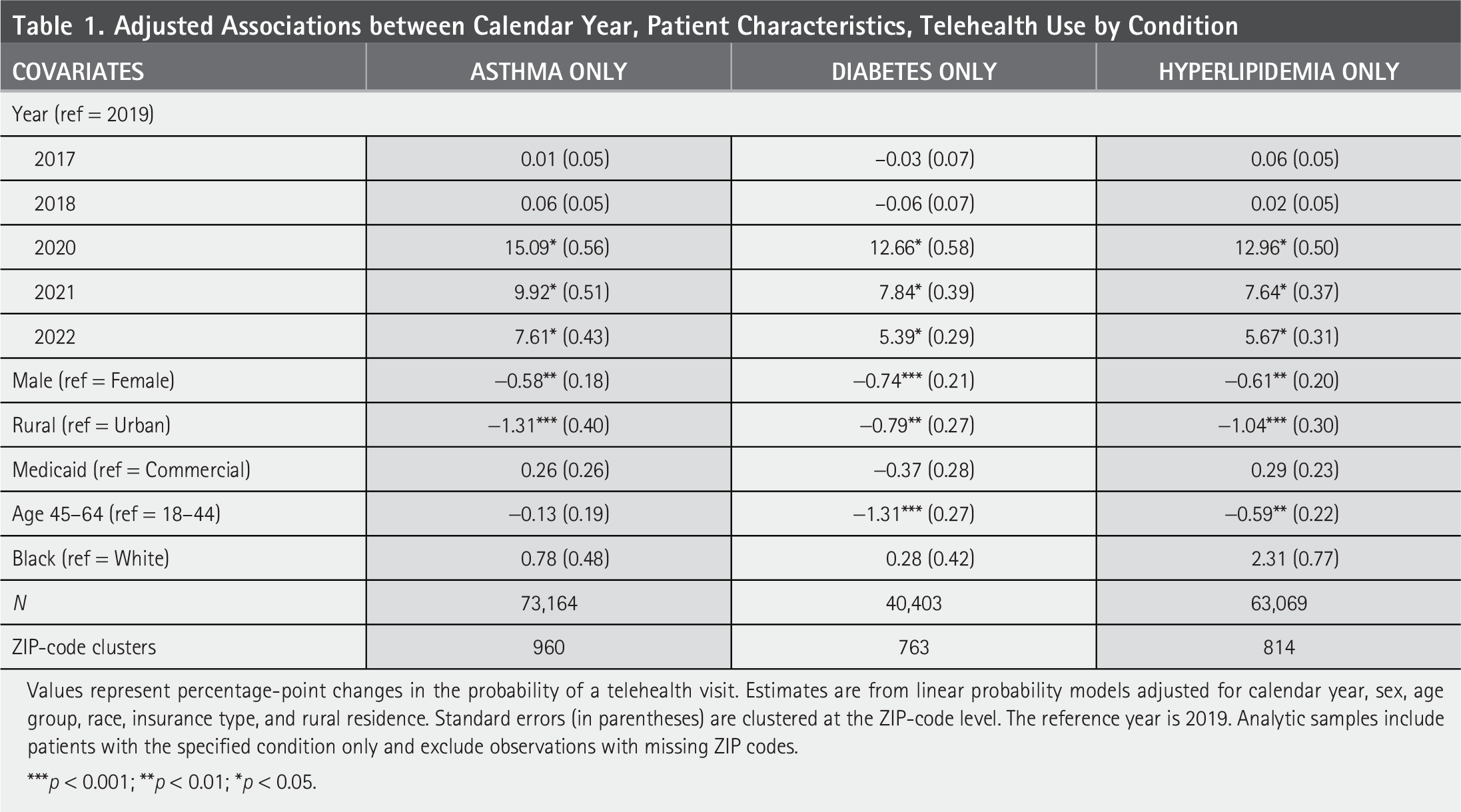
Values represent percentage-point changes in the probability of a telehealth visit. Estimates are from linear probability models adjusted for calendar year, sex, age group, race, insurance type, and rural residence. Standard errors (in parentheses) are clustered at the ZIP-code level. The reference year is 2019. Analytic samples include patients with the specified condition only and exclude observations with missing ZIP codes.
***p < 0.001; **p < 0.01; *p < 0.05.
Results
Telehealth was largely unused pre-pandemic, with no >0.4% of patient-quarters involving telehealth across any of the patient demographic and condition combinations. During the pandemic, utilization sharply increased, reaching 11.8% in asthma, 9.1% in diabetes, and 9.0% in hyperlipidemia ( Table 2 ).
Incidence of Telehealth Use among Chronic Conditions Patients: Differences by Groups and Time Period
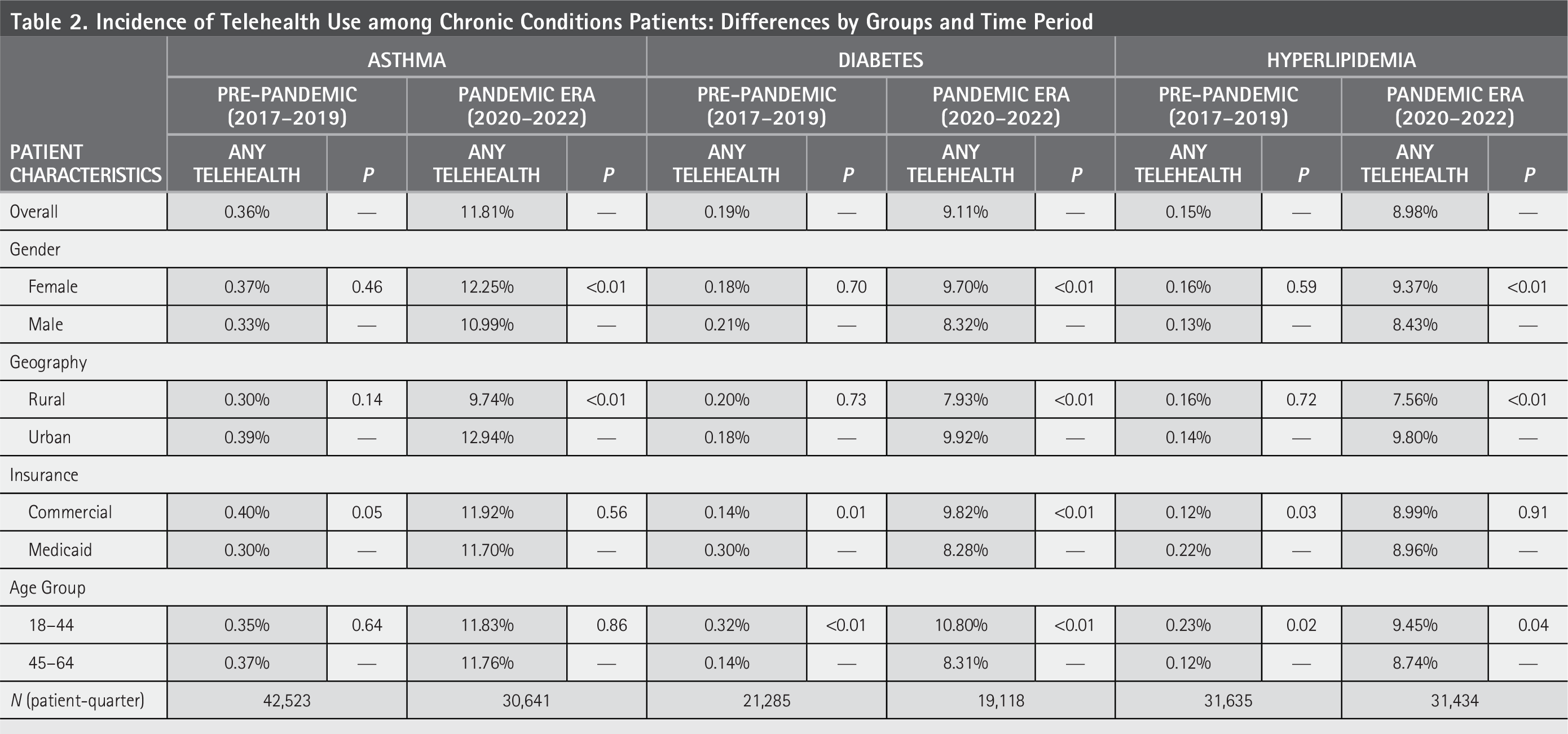
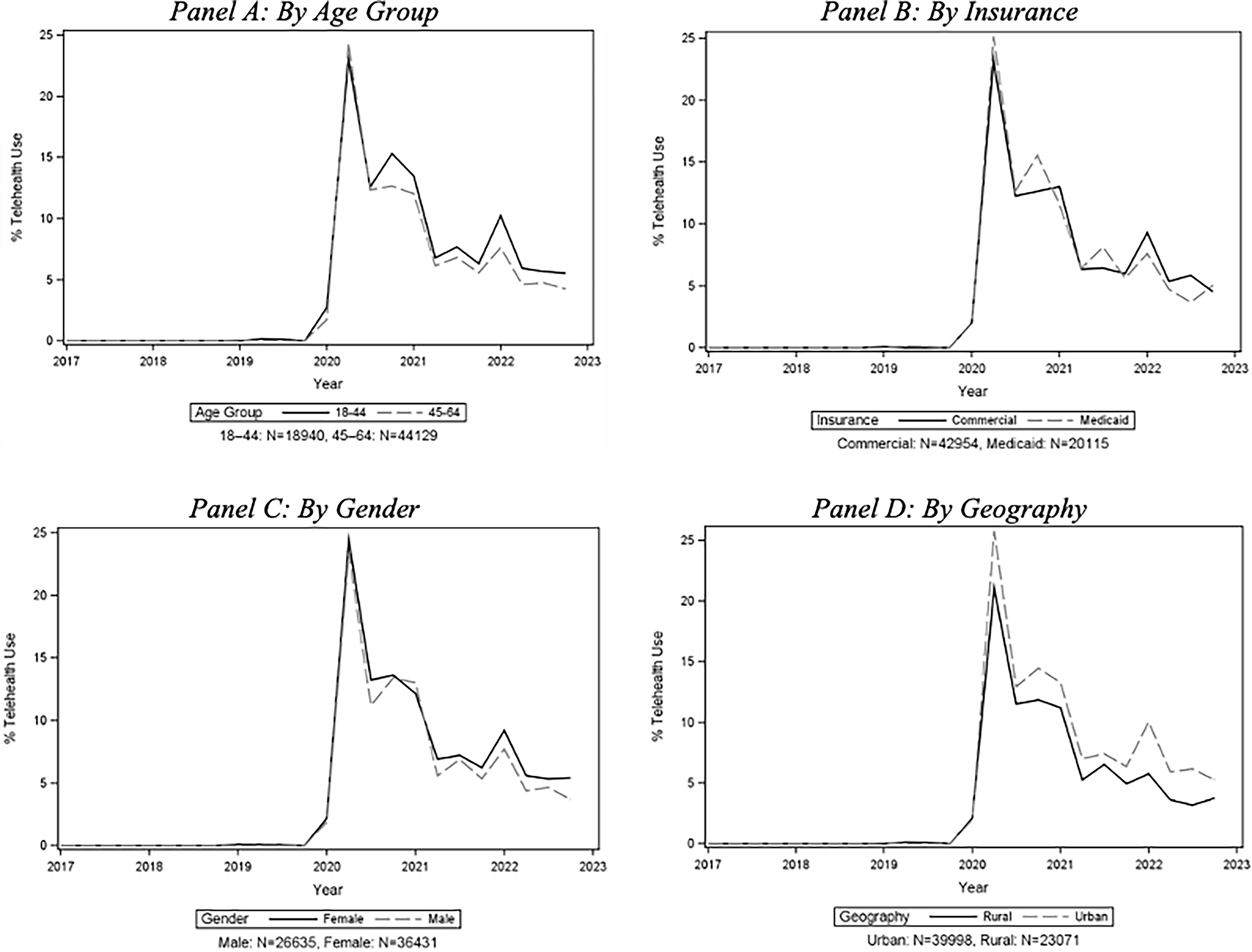
Patterns of telehealth use before and during the pandemic show a similar pattern across gender and geography with baseline levels being statistically indistinguishable before the pandemic but being quite different during the pandemic. For instance, prior to the pandemic, there were no differences by patient gender in telehealth utilization patterns. However, during the pandemic, female patients saw higher use than male patients across all conditions: asthma (12.3% vs. 11.0%, p < 0.01), diabetes (9.7% vs. 8.3%, p < 0.01), and hyperlipidemia (9.4% vs. 8.5%, p < 0.01) ( Table 2 ). These patterns are reflected in the mean plots (i.e., Panel C across Figs. 1 – 3 ) where the male telehealth utilization rates are largely below the female telehealth utilization rates.
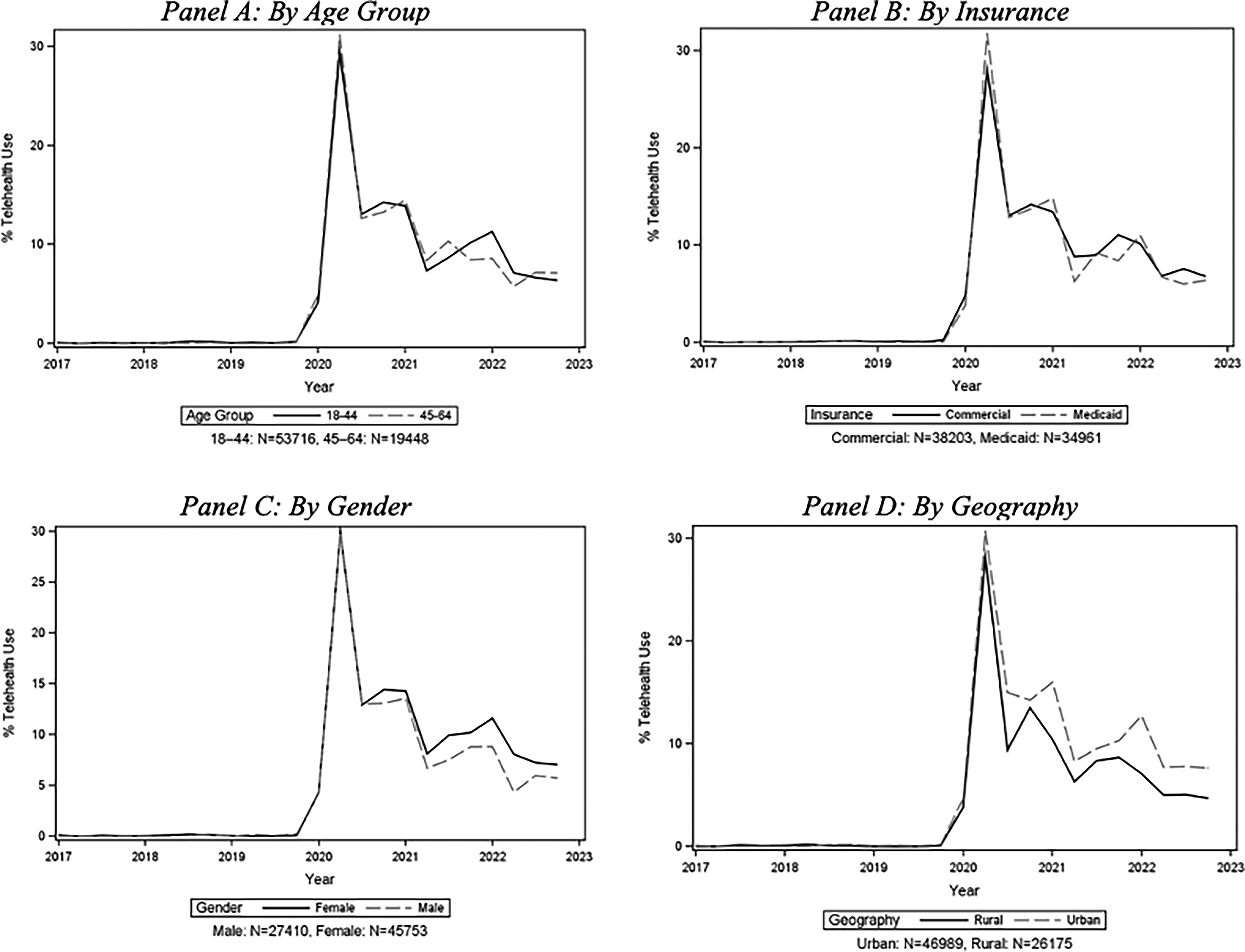
Telehealth use among patients with asthma diagnosis by quarter and group.
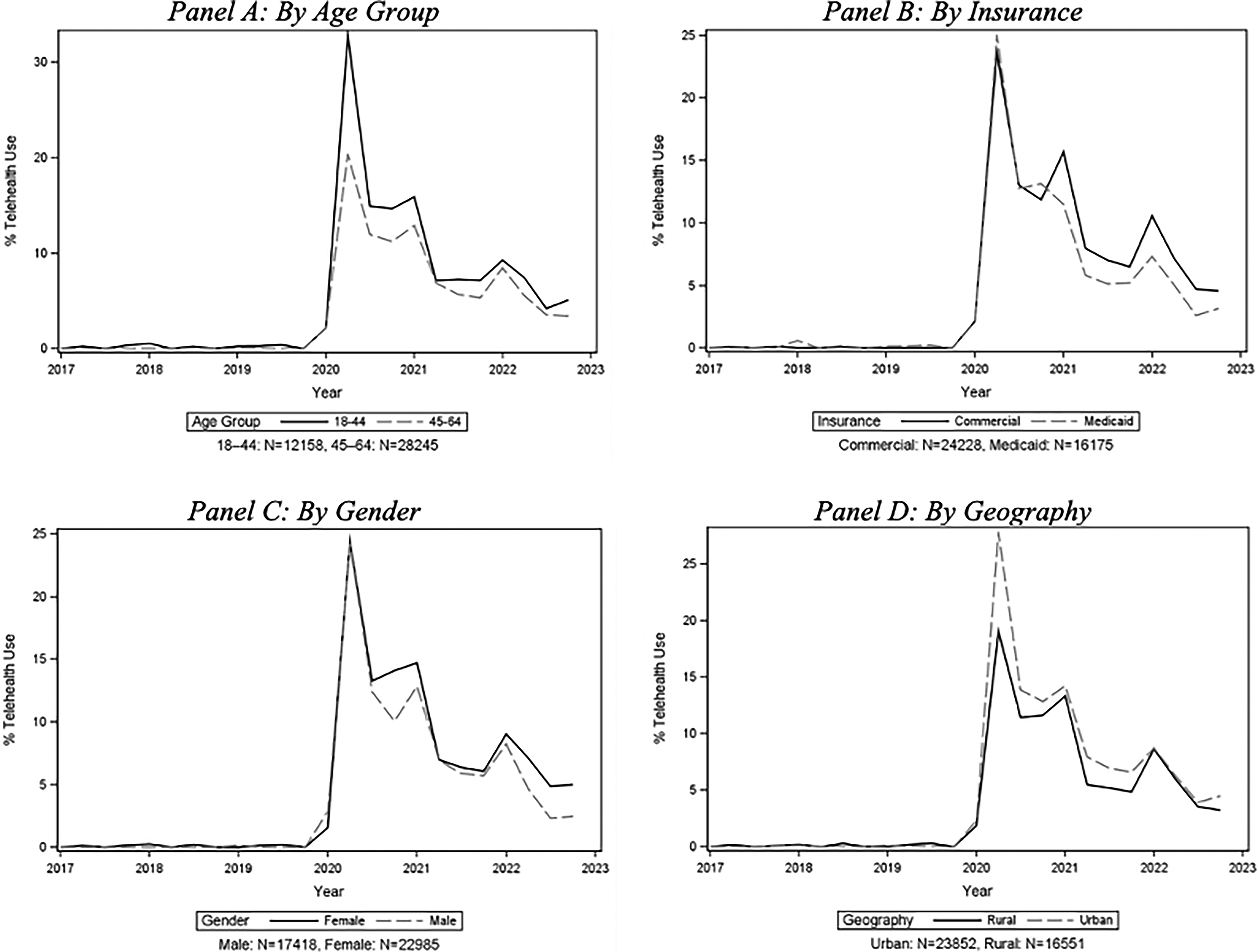
Telehealth use among patients with diabetes diagnosis by quarter and group.
Telehealth use among patients with hyperlipidemia diagnosis by quarter and group.
Similar to gender, prior to the pandemic there were also no differences by rural versus urban residence in telehealth utilization patterns, but there was a consistently higher telehealth utilization rate among urban residents during the pandemic. These pandemic-era gaps included 12.9% versus 9.7% in asthma (p < 0.01), 9.9% vs. 7.9% in diabetes (p < 0.01), and 9.8% versus 7.6% in hyperlipidemia (p < 0.01) ( Table 2 ). These patterns are similarly reflected in the mean plots (i.e., Panel D across Figs. 1 – 3 ), where the rural telehealth utilization rates are largely below the urban telehealth utilization rates.
Patterns differ when stratifying by insurance type and age. For insurance, though small, there were baseline differences in all diseases, with slightly higher telehealth use among commercial patients with asthma (0.4% vs. 0.3%, p = 0.05) and slightly higher telehealth use among Medicaid patients with diabetes (0.3% vs. 0.1%, p < 0.01) and hyperlipidemia (0.2% vs. 0.1%, p = 0.03). During the pandemic, differences between insurance types among patients with asthma and hyperlipidemia disappear, while the differences among diabetes patients reverse (commercial patients saw 9.8% use vs. Medicaid patients seeing 8.3% use, p < 0.01) ( Table 2 ). The mean plots show consistent patterns, with the commercial patients with diabetes seeing generally higher levels of telehealth compared with their corresponding Medicaid patients ( Fig. 2 , Panel B). The plots for asthma and hyperlipidemia are notably more mixed with use rate orders flipping between insurance types across time periods ( Figs. 1 and 3 , Panel B).
Among age stratifications, there were either persistently no differences by age (i.e., in asthma) or continuing differences with higher use seen among younger patients (i.e., in diabetes and hyperlipidemia). In the pre-pandemic era, younger patients with diabetes were using telehealth at a slightly higher rate (0.3% among younger patients vs. 0.1% among older patients, p < 0.01), which amplified during the pandemic (10.8% among younger patients vs. 8.3% among older patients, p < 0.01). Similarly, younger patients with hyperlipidemia saw slightly higher telehealth use baseline levels (0.2% among younger patients vs. 0.1% among older patients, p = 0.02), which also continued during the pandemic (9.5% among younger patients vs. 8.7% among older patients, p = 0.04) ( Table 2 ). These results are similarly reflected in the figures with null results matching similarly tracked lines in asthma (Panel A Fig. 1 ) generally higher levels of telehealth use among younger patients in diabetes (Panel A Fig. 2 ) and in hyperlipidemia (Panel A Fig. 3 ).
As for our regression results—which detail the year-specific effects and time-invariant group differences—we find that, relative to 2019, telehealth use sharply increased in 2020 for all conditions, with probability increases ranging from 12.7 to 15.1 percentage points (all p < 0.05). Although telehealth use declined in subsequent years, utilization remained significantly higher than prepandemic levels through 2022 across all conditions. The largest sustained increases were observed among patients with asthma ( Table 1 ).
Across conditions and time, male patients had a significantly lower probability of telehealth use compared with female patients, with relative differences ranging from −0.6 to −0.7 percentage points (all p < 0.01). Rural residence was also consistently associated with lower telehealth use (all p < 0.01), indicating persistent geographic disparities despite overall growth in telehealth adoption. Patients aged 45–64 were significantly less likely to use telehealth than those aged 18–44 for diabetes and hyperlipidemia, but not for asthma. Insurance type (i.e., Medicaid versus commercial insurance) and race (Black vs. White) were not statistically significantly different in telehealth use ( Table 1 ).
Discussion and Conclusions
Telehealth use increased significantly during the pandemic across all conditions, although overall utilization remained modest. Women consistently used more telehealth than men across all comparisons, and telehealth use among urban patients outpaced rural patients. These findings suggest that differences in telehealth adoption are not solely attributable to observable patient characteristics but may also reflect structural factors such as broadband availability, provider capacity, and differential uptake of telehealth modalities across practice settings.
Age and insurance patterns were condition-specific. Younger adults with diabetes and hyperlipidemia had higher uptake, whereas asthma showed little age variation once telehealth became widely available. Commercial patients were more likely than Medicaid patients to use telehealth for diabetes. These patterns were consistent in adjusted analyses and may reflect differences in disease management needs and perceived urgency of care.
Lower uptake among older adults with diabetes and hyperlipidemia may reflect a combination of digital literacy barriers and disease-related complications (e.g., the asymptomatic nature of hyperlipidemia may undermine the urgency of care, while diabetic retinopathy and neuropathy due to suboptimal glycemic control can impair vision and cause weakness that would interfere with the use of technology). 23 These mechanisms may help explain why age disparities were observed for diabetes and hyperlipidemia but not for asthma or hypertension.
The suitability of telehealth may also vary by the clinical context in which patients are managed. For instance, hyperlipidemia is managed nearly exclusively by monitoring patient lipid profiles via tests, which so long as patients are able to get their lab values, this clinical setting is hypothetically a natural fit for telehealth. Conversely, asthma management tends to be more clinical symptom-based, relying on patient history, their exam, and spirometry and thus may be better suited for face-to-face care. While this may lead one to expect a higher telehealth rate of uptake among patients with hyperlipidemia, we find that patients with asthma saw the highest telehealth use rates. At the same time, it is also possible that patients with asthma may have been more sensitive to upper respiratory concerns that came along with the COVID-19 pandemic.
Given our results in which telehealth utilization was highest among asthma patients compared with the other conditions, it appears that the latter concern may have come to dominate in the aggregate telehealth effect. Diabetes is managed with biomarkers, but treatment is also driven by clinical presentation, so it represents a mixed modality in terms of telehealth compatibility. In this setting, its overall use patterns more closely tracked those of patients with hyperlipidemia.
Although telehealth use declined after its peak in 2020, adjusted results indicate that utilization remained significantly higher than pre-pandemic levels through 2022 across all conditions. This pattern suggests that telehealth has become a fixture of care, to some degree, rather than a temporary pandemic response. However, the persistence of demographic and geographic disparities indicates that expanded availability alone may be insufficient to ensure equitable access.
Overall, these findings highlight increased yet uneven adoption. The pandemic catalyzed a surge in telehealth, but differences across stratifications remain through 2022. Expanding broadband in rural areas, additional support for older adults with diabetes and hyperlipidemia about the importance of follow-up care even if presently asymptomatic, and addressing insurance-related barriers will be essential to improve equitable access.
LIMITATIONS
Our study was limited to commercial and Medicaid enrollees in Arkansas and may not generalize to states with different characteristics. These are also single-diagnosis conditions only, and many patients have overlapping chronic care conditions.
CONCLUSION
Telehealth use surged during the pandemic across all studied chronic conditions. Women, urban residents, and younger adults with diabetes and hyperlipidemia were the most likely adopters, while rural patients and older adults with diabetes or hyperlipidemia lagged. Although overall telehealth utilization declined after its peak, adjusted analyses indicate that telehealth has become an embedded component of care. Ongoing efforts should focus on supporting clinically-appropriate, even, and sustained access across demographic and condition groups.
Footnotes
Acknowledgments
The contents are those of the author. The views expressed in this publication are solely those of the authors and do not reflect the official views of the funders or the U.S. government.
Access to the Arkansas All-Payer Claims Database for this study was provided by support from the Arkansas Biosciences Institute/Arkansas Insurance Department/Arkansas Health Care Transparency Initiative Collaboration.
Author Disclosure Statement
There are no competing interests to report.
Funding Information
This work was funded by a subaward from the University of Alabama at Birmingham (#
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.