
Abstract
Introduction
Although the use of sports compression socks is becoming more popular, there is still a lack of knowledge regarding the helpfulness of these garments for physical movement or sports use. One of the main effects attributed to the use of compression sock is the facilitation of venous blood flow return which is thought to improve performance and recovery.
Methodology
In this study, 10 trained runners performed 2 treadmill running tests for 30 min to 75% of their maximum aerobic speed, without sports socks (control) and with different sports compression socks. We measured popliteal vein flow volume before and after each test using magnetic resonance imaging.
Results and discussion
No differences were observed between the conditions before the test (p > 0.05), but there were differences between the high compression socks condition and the control after the test (p < 0.05). Exercise increased the venous flow in both legs in the control (p < 0.001) as well as in the right leg with the high compression sock type (p < 0.01) but there were no differences in the behaviour of the different sock compression levels (p > 0.05).
Conclusion
The use of sports compression socks with different levels of compression does not increase the volume of venous blood return via the popliteal vein in trained athletes after running for 30 min.
Introduction
The use of sports compression socks (CS) is becoming more popular with the increase in sports participation, especially in endurance sports such as athletics, trail running, triathlons, and cycling, among others. Although there is scientific evidence regarding the different effects of sports CS, there is a lack of knowledge about their mechanisms during physical movement or sporting use [1]. In addition, many of the benefits of CS highlighted by manufacturers have not been validated [2]; moreover, there are many heterogeneity among the variables included in such studies [3].
Sports CS is based on the benefits of compression therapy in cardiovascular diseases [4,5]. Recent studies indicate that compression mechanism to which veins are subjected, obeys more closely Pascal’s Law [6–8]. However, there is scientific evidence that biological mechanisms influence the return of venous flow, like muscular pumps [9–11], respiratory pumps [12], hydrostatic pressure [7–9,12,13], and inertia produced by movement [14].
The design of CS is always based on creating gradual compression which decreases from the most distal to the most proximal region of the leg [5]. Between effects attributed to CS, the following stand out: increased tissue oxygenation [9,15], decreased venous volume [9,10,16], better blood redistribution [17], and increased venous flow velocity [10,13]. There are different materials used for the manufacturing of compression garments like polyamide, polypropylene, lycra, elastane, and nylon. In general, the heterogeneity of the test procedures as well as the differences between the types and levels of compression make the comparison of the various studies evaluating the compression sportswear difficult [2]. Nevertheless, this kind of compression does not cause significant changes in skin regulation or body temperature, forcés development, or perceived exertion or comfort, but increase attenuation and reduce impact in running [2]. The analysis tools and methodology used to analyse these effects include near-infrared spectroscopy (NIRS) [9,15], air plethysmography (APG) [10,16,18,19], strain-gauge plethysmography [7,8,17], Doppler ultrasonography (echo-Doppler) [12,13,20–22], and magnetic resonance imaging (MRI) [23–26]. The variability inherent in using such a wide range of instrumentation makes it very difficult to directly measure the effects CS have on vascularisation. MRI provides accurate data on the mechanical effects of compression in lower limbs [23], and in addition, according to Partsch et al. [26], it is one of the most suitable methods for measuring haemodynamic variables. So far, very little work has been done in sports science using this type of methodology to analyse the effect of CS on vascularisation. On the other hand, regarding the effects attributed to the use of compression garments in endurance modalities, it should be noted that no studies have been found that provide performance improvements with respect to the time used to complete them in race-type tests: marathon/half marathon [27], 15 km trail [28], or 10 km races [29]. For this reason, it is important to take into account the originality using MRI during running fatigue effort with compression garments. Thus, in this present study, we aimed to (a) quantify venous return after submaximal running effort using sports CS, and (b) analyse how venous return flow is influenced by medium or high CS compression. We hypothesised that increased levels of CS compression are directly related to increases in venous flow after a submaximal running exercise.
Methods
Participants
The study sample comprised 10 male runners (age: 35 ± 5 y, height: 174 ± 5 cm, weight: 74 ± 4 kg, VO2 max: 53 ± 4 ml/kg/min) who trained 40 ± 10 km/week at an amateur level, with training experience 5 ± 2 years and all of them familiarized with running in a treadmill. None of the participants had had any injuries in the past year and they did not suffer from any cardiovascular pathology. Selected participants had similar performance level, height and weight in order to eliminate possible interactions due to running biomechanics [14]. The performance level was also important, taking point on the athlete’s familiarization with this kind of effort that is not easy for athletes without experience or low level. The study protocols complied with the mandates set out in the Declaration of Helsinki and was approved by the University of Valencia ethics committee. The participants gave their written informed consent prior to participating in the study.
The test conditions and compression socks
The participants performed two treadmill tests on different days, one week apart, at the same time of day and in a randomised order. On one of these days, they ran without compression socks (woCS) and on the other they wore a high and a medium-strength (differentiated according to the specifications of commercial branding as ‘strong’ (SCS) or ‘average’ (MCS), but do not have more information about the exact level of compression) socks below-the-knee CS, one on each leg, in a randomly assigned way. In the intervening time, they performed supervised maintenance training and were asked not to do any training session 24 h prior the test. The participants were blinded to the differential compression and the objectives of this study.
According to the manufacturer’s description, textile composition of MCS was 79% polyamide, 21% elastane; and composition of SCS was 52% polyamide, 25% elastane, 23% polypropylene. Sizes of CS used in the study were taken by measuring the calf circumference at the widest point, always measured by the same researcher (Size III 32–38 cm; size IV 39–44 cm; size V 45–50 cm).
Experimental design
The running protocol required running on a treadmill (Excite Run 700, TechnoGym SpA, Gambettola, Italy) with a 5-min warm up at 8 km/h, followed by a total run time of 30 min at 75% of their maximal aerobic speed, as determined by an individual stress test performed by each of them a month prior to the study.
Magnetic resonance imaging
Prior to running, the participants underwent an MRI in the supine position to measure the volume of flow in the popliteal vein (is considered a deep vein and is located at the lower border of the popliteus muscle and formed by the union of the tibial veins) in each leg. The same test was performed immediately after they finished the running test. In CS condition, the measurement was done wearing CS, before and after the running test. A Siemens MAGNETOM Sonata 1.5 T MR A30 (software version 4) was used for the MRI. The table-array coils were used for the rear area and the surface-array coils (PA1–PA6) were used for the anterior zone, using six channels for the legs and four channels (BO1–BO2) for the thighs. The athletes were placed in the decubitus supine position, feet first. Cardiac gating was put in place and the runner was instructed to breathe rhythmically to synchronise the acquisition with their respiratory and cardiac frequency. The sequences were obtained from protocols pre-programmed into the software by the manufacturer’s (Sonata, Siemens©). The relationship between the field of view (FOV)—the anatomical area under study—size, the matrix (the number of pixel squares in the image), and the averages (the points read per frame), allows the image quality to be improved. Parameters such as echo time (TE) and repetition time (TR) are used to control the MRI image and can enhance the longitudinal relaxation time (T1; TE < 85 and TR < 700) or the transverse relaxation time (T2; TE ≥ 85–120 and TR ≥ 2000) images (Figure 1).
Statistical analysis
The Statistical Package for the Social Sciences program was used for all our statistical analyses (SPSS®, IBM® Corporation, New York, USA). We checked the normality of the variables (using the Shapiro–Wilk test), and performed a descriptive analysis and t-tests to compare the means between the pre- and post-running test groups for each condition, comparing related samples (same athlete, same leg: woCS and MCS or SCS). Probability levels exceeding 95% (p = 0.05) were considered statistically significant.
Results
Popliteal vein mean blood flow (mL·s−1; 95% confidence interval [CI]) ± SD before running without compression socks (woCS), with medium-strength compression socks (MCS) and with high-strength compression socks (SCS).


MRI software procedures used to measure the mean blood flow through the popliteal vein.
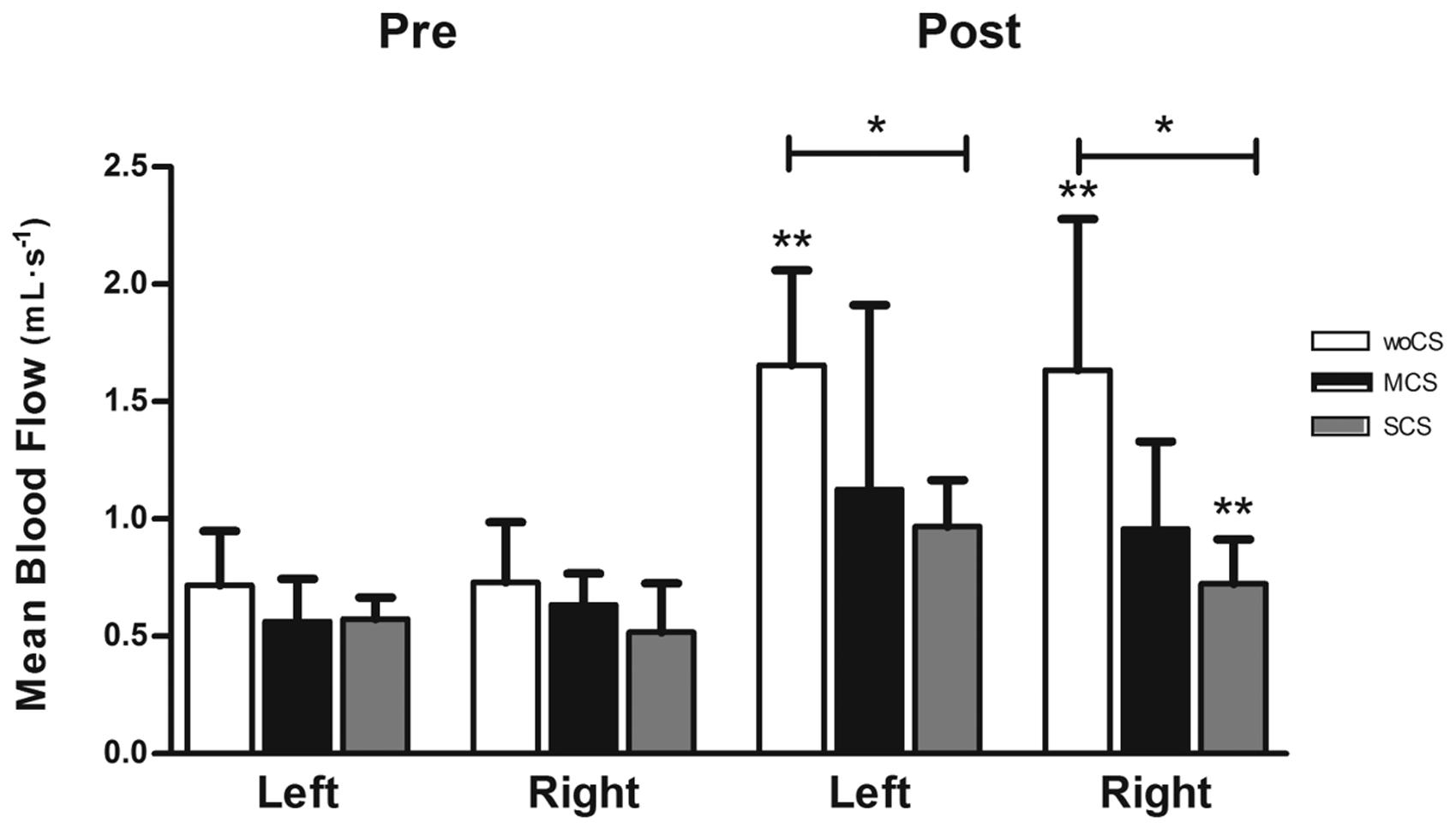
Popliteal vein mean blood flow (mL·s−1; 95% CI) ± SD pre- and post-running test without compression socks (woCS), with medium-strength compression socks (MCS), and with high-strength compression socks (SCS), in the right and left leg. **p < 0.01 vs. pre-run; *p < 0.05 vs. woCS.
Popliteal vein mean blood flow (mL·s−1; 95% CI) post-run without compression socks (woCS), with medium-strength compression socks (MCS) and with high-strength compression socks (SCS).
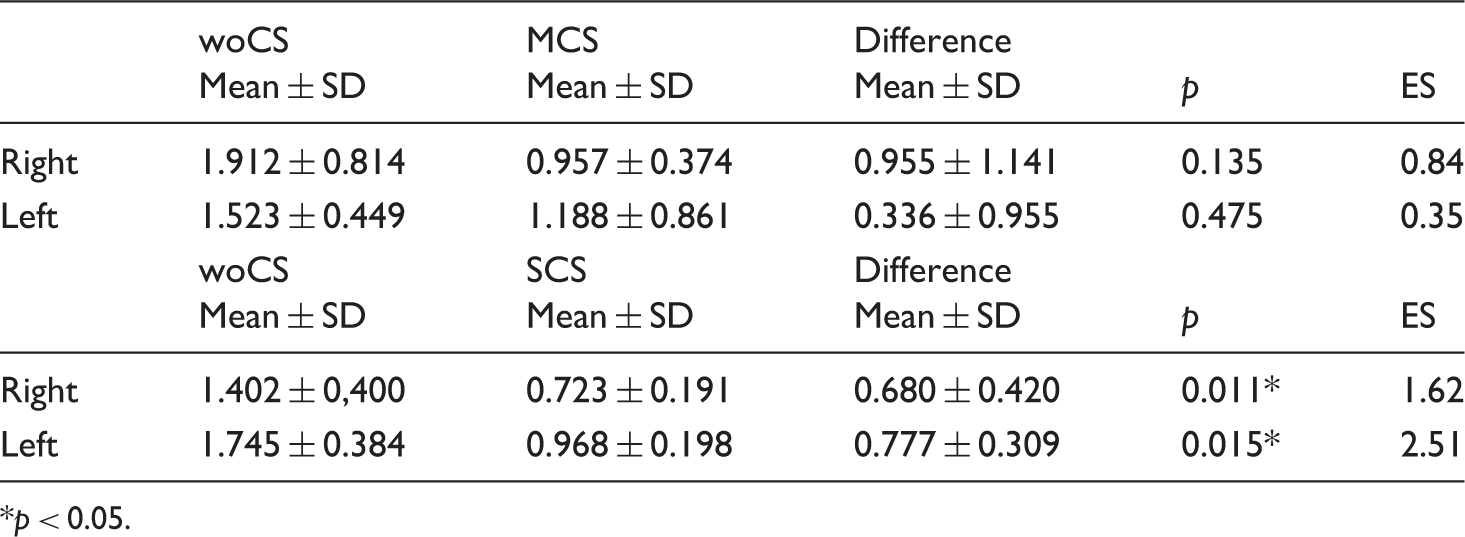
*p < 0.05.
Popliteal vein mean blood flow (mL·s−1; 95% CI) in the right and left leg, pre- and post-fatigue without compression socks (woCS), with medium-strength compression socks (MCS), and with high-strength compression socks (SCS).

**p < 0.01.
There were no statistically significant differences in the venous return found for the MCS and SCS compression levels pre- and post-test (p = 0.392).
Discussion
In this study, we analysed the effect of two types of running sports CS (medium and high-strength) on lower limb venous blood return flow to evaluate the hypothesis that this flow increases when these CS are used compared to the absence of their use.
Results show that the type of compression applied by the CS does not influence the volume of venous popliteal vein blood return flow from the legs before or after running. Although Agu et al. [9] did note that venous flow was higher when CS with a higher degree of compression were used with patients with chronic venous insufficiency (CVI), the results they obtained at rest for different sports CS compression levels did not significantly differ with respect to the woCS condition (p > 0.05). However, this may be because the compression they used was not sufficiently high to achieve this effect: in this sense, it was significantly lower than the 40 mmHg recommended by Partsch and Mosti [25]. However, the results obtained concur with those from Dascombe et al. [15], who also did not observe any differences between different grades of CS compression.
There is great variation in the scientific literature regarding the ideal attributes for improving venous flow, for example, in terms of pressure gradient and the type of material that should be used: gradual [11,15,16,30,31] versus progressive compression [31,32] and the commonly used elastic versus a more rigid [6,19,25] material. Thus, Beliard et al. [33] suggest unifying both the methodological and compression criteria.
According to the CS composition, Reich et al. [34] showed that each manufacturer has their own composition, and pressure measurements for CS show heterogeneous and incomparable results. Therefore, it seems that depending on the structure, composition, orientation and hence garment construction, CS effects in pressure being applied could change [35].
CS are limited because, during exercise such as running, the hydrostatic pressure and muscular pumps require very high compression (>40 mmHg) to achieve a reduction in the venous diameter [8,36,37]. This high level of compression is unlikely to be comfortable, but perceived comfort is a key factor in CS [16] and sports accessories [38] achieving a positive effect. In the clinical/medical setting, there are established compression-level ranges (Classes I, II, III, and IV) depending on the pathology, although doubts still remain about the suitability of different compressive garments in certain situations or pathologies [4,5]. In contrast, in the field of sports science, there is no consensus on the garment type (e.g. ankle, knee-high, or calf-only socks or stockings) or degree of compression required to improve performance and recovery [3].
On the other hand, the data obtained in this study showed that the volume of venous flow was greater after running because exercise increases perfusion of the muscular bundles involved in the movement. However, we observed a non-significant decrease in the venous-return flow while wearing CS with respect to the woCS condition before exercise, and this trend was significant after exercise (1.912 ± 0.814 woCS vs. 0.957 ± 0.374 mL·s−1 MCS, p = 0.135; 1.402 ± 0.400 woCS vs. 0.723 ± 0.121 mL·s−1 SCS, p = 0.011 in the right leg; 1.524 ± 0.449 woCS vs. 1.188 ± 0.861 mL·s−1 MCS, p = 0.475; 1.475 ± 0.384 woCS vs. 0.968 ± 0.198 mL·s−1 SCS in the left leg). These results agree with those from Sperlich et al. [39] who also observed lower venous flow after exercise in the CS condition in cyclists. These results are contrary to the application of compression to facilitate venous return [5], given that they produce the reverse situation. In this sense, other studies have suggested hypotheses that could explain our results, as outlined below.
Evacuation of fluid via non-venous routes such as the lymphatic drainage system: Buhs et al. [40] found that leg perimeter at rest significantly increased by 2.3 ± 1.0 cm woCS (p < 0.001) but decreased −0.5 ± 0.7 cm (p = 0.003) when wearing CS. In addition, the runners included in this study were healthy and had effective muscle pumps [9]. It is also possible that the better perception of inflammation and heaviness of the legs in other studies [16,31] may reinforce this hypothesis. Transfer of extravascular fluid to the intravascular space: Lurie et al. [24] also observed a 3.6% decrease in subcutaneous, but not sub-fascial, tissue when applying compression using different systems. This suggests that the compression is partly caused by the transfer of extravascular fluid to the intravascular space and superficial and deep veins, accounting for the absence of any differences in the sub-fascial tissue volume. Surface versus deep venous system: Downie et al. [23] observed how the surface area of the superficial calf veins did not reduce as much as that of the deep veins when under compression (39% vs. 64%). In this line, in an observational study of the effect of CS or bandaging in a patient with varicose veins, Partsch et al. [26] found that low-level compression, such as that exerted by class II therapeutic CS (22 mmHg), produced a slight reduction in the size of deep, but not superficial, veins. On the other hand, Sperlich et al. [39] found that venous flow velocity reduced after exercise while wearing CS in both deep and superficial thigh veins. Thus, they posit that anatomical differences may not correspond to haemodynamic differences; it appears that venous flow velocity should not be modelled using the Poiseuille Law because the shape of veins is not always cylindrical because they acquire an elliptical shape while under compression [23].
Given that the volume of venous flow strongly and proportionately decreases post-run while wearing CS, our comparison between different time-points in this study did not show any statistically significant differences between the woCS and CS conditions (p = 0.392), although there were differences between the MCS and SCS pairwise comparison results (Table 3). As also suggested by other authors [33], our results indicate that further study of the true haemodynamic effect of sports CS during exercise is still required. This would require sports scientists to reach a consensus in several aspects, including: (a) normalising the type of sports CS manufacturing (gradual or progressive compression, and/or with a high or low pressure-gradient); (b) unification of the methodology and instrumentation used to measure the haemodynamic variables. In this sense, ultrasound techniques [12,13,20,22,24,37,40] and magnetic resonance imaging [12,23,24,26,37,40] techniques would appear to be the best options for directly measuring these variables. When designing a venous flow measurement protocol, it is also important to account for the possibility that popliteal vein function could be affected by the capacity of the superior vessels [12], or that there may be differences in the haemodynamic behaviour of different veins even during the same intervention type [23,26]; (c) consideration of the effect compression might have on venous haemodynamics during and immediately after exercise, which could confirm an improvement in recovery. Regarding this line of enquiry, Lattimer et al. [16] observed a reduced venous return volume in patients wearing CS, but the ejection fraction during the first second after cuff deflation was better while wearing CS. Thus, although MRI is one of the most reliable means to determine anatomical and haemodynamic variables, perhaps ultrasound should be considered a useful tool for making more flexible measurements at different anatomical regions and time points. In conclusion, the present study has demonstrated that the use of sports socks with different types of compression does not increase the volume of venous return from the popliteal vein after performing a running exercise, but it does produce lower values compared to the condition without wearing CS.
Footnotes
Acknowledgements
The authors would like to thank all the runners who kindly participated in the study. We would also like specially acknowledge to PhD. Mr. Vicente Tormo for his support, great knowledge and to his smile during this study (R.I.P), and Ruben Hinajeros (ERESA Clinic, Valencia).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.