
Abstract
Nurse staffing and missed nursing care are associated with patient readmissions. However, the mediating role of missed care in this relationship is not well understood. This retrospective study investigated the potential mediating effect of missed care on the relationship between nurse staffing and patient readmissions across 573 U.S. hospitals. Mediation analyses examined whether, and to what extent, missed care explains the relationship between nurse staffing and patient readmissions. Nurse staffing was associated with patient readmissions both directly and indirectly through missed care, which accounted for 10% of the total association. These findings suggest that missed care is an important pathway through which nurse staffing affects readmission rates. Addressing inadequate nurse staffing and reducing missed care are essential strategies for lowering readmissions. The findings have important implications for developing evidence-based interventions and informing policy to improve the quality of care in healthcare institutions.
Background
The relationships among nurse staffing, missed care, and patient readmissions have become a critical area of study in recent years, driven by the goal of reducing preventable readmissions. Adequate nurse staffing is fundamental for delivering high-quality healthcare and minimizing the risk of adverse events and poor outcomes, such as preventable readmissions (Kane et al., 2007; Lasater & McHugh, 2016; Needleman et al., 2011; Shekelle, 2013). Research indicates that higher nurse staffing levels correlate with better patient outcomes, largely due to the provision of timely and effective care (Bruyneel et al., 2015). Despite the substantial evidence supporting the positive relationship between nurse staffing and patient outcomes (Kane et al., 2007; Shekelle, 2013), gaps in our understanding persist regarding how specific staffing levels influence the incidence of missed care and its subsequent effect on readmission. This knowledge gap highlights the need for further research to elucidate the nuanced mechanisms through which nurse staffing directly affects patient readmissions, with missed care serving as a pivotal factor in this equation.
Missed care, referring to the delay or omission of essential nursing interventions, is a critical phenomenon to consider in understanding the dynamics between nurse staffing and patient outcomes (Griffiths et al., 2018; Jones et al., 2015; Kalisch et al., 2009; Park et al., 2018; Zhao et al., 2020). Common examples of missed care items include the provision of emotional support and patient education (Jones et al., 2015). Missed care compromises patient safety and overall care quality, and is influenced by factors such as workload, patient acuity, and communication breakdowns (Kalisch et al., 2011b; Schubert et al., 2008). The consequences of missed care are far-reaching, including medication errors, patient falls, nosocomial infections, critical incidents, and pressure ulcers (Schubert et al., 2008). Furthermore, missed care has been significantly associated with hospital readmissions, imposing substantial costs on patients, families, and the healthcare system as a whole (Brooks Carthon et al., 2015).
Brooks Carthon et al. (2015) illuminated this issue through an analysis of 160,930 patients with heart failure across 419 hospitals in 2005 and 2006. Their findings revealed that seven of 10 missed nursing care activities independently predicted the odds of readmission, even when controlling for patient characteristics. Moreover, in models controlling for patient and hospital characteristics, four missed care activities: care coordination, care planning, teaching/counseling, and treatments/procedures, persistently predicted readmission. These results suggest that the association of certain missed care items with readmissions can be attributed to variations in underlying staffing levels, emphasizing the critical interplay between nurse staffing, missed care, and patient readmissions. This evidence underscores the importance of conducting further research into the potential mediating role of missed care in the relationship between nurse staffing and readmissions, with the ultimate goal of enhancing patient outcomes and optimizing healthcare delivery.
New Contributions
Our study makes significant contributions to the existing literature by being the first to examine the mediating role of missed care in the relationship between nurse staffing and hospital readmissions using a unique methodological approach that combines multiple data sources. Our findings have the potential to inform the development of targeted interventions and strategies to reduce missed care and readmissions, ultimately improving patient outcomes and optimizing healthcare delivery.
Method
Design and Conceptual Model
This cross-sectional, observational study leveraged data from multiple sources to explore the mediating role of missed care in the relationship between nurse staffing and hospital readmissions, while accounting for various hospital factors. Our conceptual model draws upon Donabedian (1966)'s model for evaluating the quality of medical care and the existing literature on the relationship between nurse staffing, missed care, and readmission (Figure 1). Donabedian proposed that healthcare outcomes are the result of a complex interplay between system characteristics (e.g., nurse staffing levels), process variables (e.g., the occurrence of missed care), and outcomes (e.g., hospital readmissions). Specifically, in the context of our study, the model is operationalized as follows:
System Characteristics: Nurse staffing is considered a key system characteristic, influencing both missed care and readmission. Process Variables: Missed care is identified as a crucial process variable, acting as a mediator between nurse staffing and readmission. Outcomes: Hospital readmissions serve as the outcome variable, with the model suggesting that improvements in nurse staffing and missed care can lead to better health outcomes.
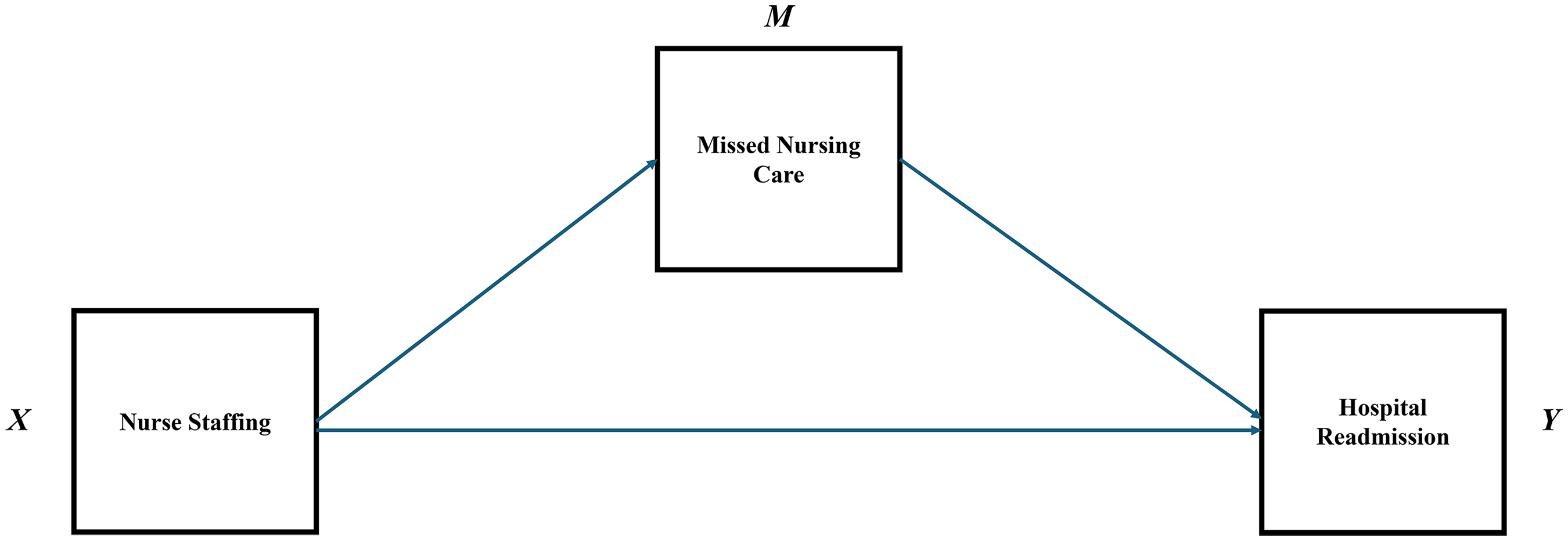
Conceptual model for the relationship between nurse staffing, missed nursing care and readmission.
Sample and Setting
The study was conducted in the United States using data from 573 hospitals in 2015. Eligible hospitals had (a) survey data from five or more inpatient staff nurses and (b) complete data on nurse staffing, missed care, readmission, and hospital characteristics.
Data Sources
Data for this study were obtained from two main sources. The 2015 National Database of Nursing Quality Indicators (NDNQI) annual Registered Nurse survey provided nurse staffing data, including the number of patients assigned to each nurse during their last shift. The NDNQI is a voluntary nursing benchmarking database. This data source is proprietary, accessed through a formal data use agreement with Press Ganey, which owns the NDNQI, as acquired from the American Nurses Association in 2014. Hospital readmission rates were sourced from the publicly available 2015 Centers for Medicare and Medicaid Services Hospital Compare database. Structural characteristics of hospitals were provided by the NDNQI staff, who collect these data from member hospitals. These sources were linked by NDNQI staff using hospital identifiers. The year 2015 was chosen to ensure the availability and alignment of data across all sources.
Measures
Independent Variable: Hospital-Level Patient-to-Nurse Ratio
The measure of nurse staffing used in this analysis was the patient-to-nurse ratio, derived from the NDNQI survey data. This decision was based on our focus on the direct experience of nurses with their workload, as patient assignments directly impact nurses’ ability to deliver care. Although the NDNQI also collects data on hours per patient day (HPPD) quarterly, which includes registered nurse skill mix, those data were not proposed nor obtained for this research project. We acknowledge, however that HPPD is a valuable measure and suggest future studies might explore its utility in sensitivity analyses to corroborate our findings. The patient-to-nurse ratio was treated as a continuous variable and aggregated at the hospital level, representing the average number of patients assigned to nurses in each hospital.
Mediating Variable: Hospital-Level Percentage of Nurses Reporting Missed Care
Missed care was measured as a continuous variable at the hospital-level from the NDNQI survey. Nurses were asked to report which necessary care activities were left undone from a list of 16 items. These included adequate patient surveillance, oral hygiene/mouth care, comfort/talk with patients, adequately document nursing care, administer medications on time, treatments and procedures, prepare patients and families for discharge, develop or update patient plan of care, skin care, pain management, teach/counsel patients and family, coordinate patient care, ambulation or range of motion, administer oral feedings on time, help or counsel breastfeeding mothers/support or promote breastfeeding, and central line assessment/maintenance/care. Using these responses, we calculated a hospital-level variable entitled “any missed care,” which represented the proportion of nurses in each hospital who reported leaving at least one care activity undone.
Dependent Variable: Hospital-Level All-Cause 30-Day Readmission
The dependent variable was the risk-adjusted all-cause 30-day hospital-wide readmission score, which is intended to capture all-condition, unplanned readmissions within 30 days of discharge. This measure serves as a broad indicator of hospital quality by evaluating how well facilities prevent unnecessary readmissions. To ensure fair comparisons between hospitals, Centers for Medicare and Medicaid Services employs a two-step risk adjustment process. First, it estimates the impact of patient-specific factors, such as age and clinical diagnoses, on readmission risk within each hospital to isolate hospital-independent effects. Then, it removes these patient-related influences when comparing hospitals, allowing the remaining differences to reflect hospital quality rather than patient case mix (Hoyer et al., 2018; Kansagara et al., 2011). A lower score indicates better hospital performance in terms of risk-adjusted 30-day readmission rates.
Hospital Characteristics
Hospital characteristics were reported by NDNQI member hospitals and linked to our study sample by the NDNQI analyst. Hospital characteristics included ownership (not for profit, government-nonfederal, for profit-investor owned), bed size (less than 100, 100–299, 300+), teaching status (academic medical center, other teaching, non-teaching), and the percentage of critical care nurses. In addition to the characteristics mentioned, we considered including regional location and the educational background of nurses from the NDNQI data. These factors were ultimately not included in the analysis due to our research focus but represent potential variables for future research exploring additional dimensions of the hospital context and nurse staffing.
Statistical Analysis
Descriptive Statistics
All data analyses were conducted using R version 4.4.1. Descriptive statistics included means and standard deviations for continuous variables, and frequencies and percentages for categorical variables. We assessed a range of variables descriptively, including hospital characteristics (ownership type, bed size, teaching status, percentage of critical care nurses), nurse staffing ratios, and the percentage of nurses reporting missed care. These descriptive statistics provided an overview of the sample and context for our mediation analysis. The University of Pennsylvania Institutional Review Board approved this study.
Mediation Analysis
To assess the direct relationship between hospital nurse staffing and hospital-wide patient readmission rates, as well as the potential indirect association through missed nursing care, we conducted mediation analysis using the mediation package in R (Imai et al., 2010; Tingley et al., 2014). This approach allows for the estimation of direct and indirect effects under the potential outcomes (counterfactual) framework, which conceptualizes causal effects by comparing what would happen to the same hospital under different hypothetical scenarios (e.g., if the hospital had higher versus lower nurse staffing levels). Specifically, we examined whether, and to what extent, the effect of hospital-level nurse staffing (independent variable) on hospital-wide all-cause readmission rates (dependent variable) is transmitted through the percentage of nurses who reported missed care (mediator).
In this analysis, the total effect of nurse staffing on readmission rates is decomposed into two components: (a) the indirect (mediation) effect, which quantifies how much of the association is explained by missed care, and (b) the direct effect, which captures the remaining association between nurse staffing and readmissions independent of missed care (Pearl, 2014; Robins & Greenland, 1992). This counterfactual-based method provides more rigorous and interpretable estimates than traditional regression-based mediation approaches by defining causal effects in terms of contrasts between clearly specified hypothetical conditions.
Linear regression with least squares was used for the mediator model, with missed nursing care as the dependent variable and nurse staffing and hospital characteristics as independent variables. Next, we modeled readmission rates as the dependent variable using linear regression with least squares, including nurse staffing, missed nursing care, and the same covariates as independent variables. The mediate function from the R package was then used to estimate the average mediation (indirect) and direct associations. A nonparametric bootstrap approach with 1,000 replications and bias-corrected and accelerated intervals was applied, as recommended for estimating mediation (indirect) associations (Preacher & Hayes, 2008).
Results
Descriptive Statistics
Table 1 shows the distribution of hospital characteristics among the study sample of 573 hospitals. Most hospitals were not-for-profit (88.0%), followed by government nonfederal (5.8%), and for-profit investor-owned (6.2%). In terms of bed size, 22.1% of hospitals had less than 100 beds, 48.9% had 100–299 beds, and 29.0% had 300 or more beds. Teaching status varied, with 9.4% classified as academic medical centers, 35.1% as other teaching hospitals, and 55.5% as nonteaching hospitals. The mean patient-to-nurse staffing ratio was 6.3 (standard deviation [SD] = 0.9). On average, 67.7% of nurses reported leaving at least one care activity undone (SD = 8.4). The average percentage of critical care nurses per hospital was 10.4% (SD = 6.0).
Hospital Characteristics (N = 573).
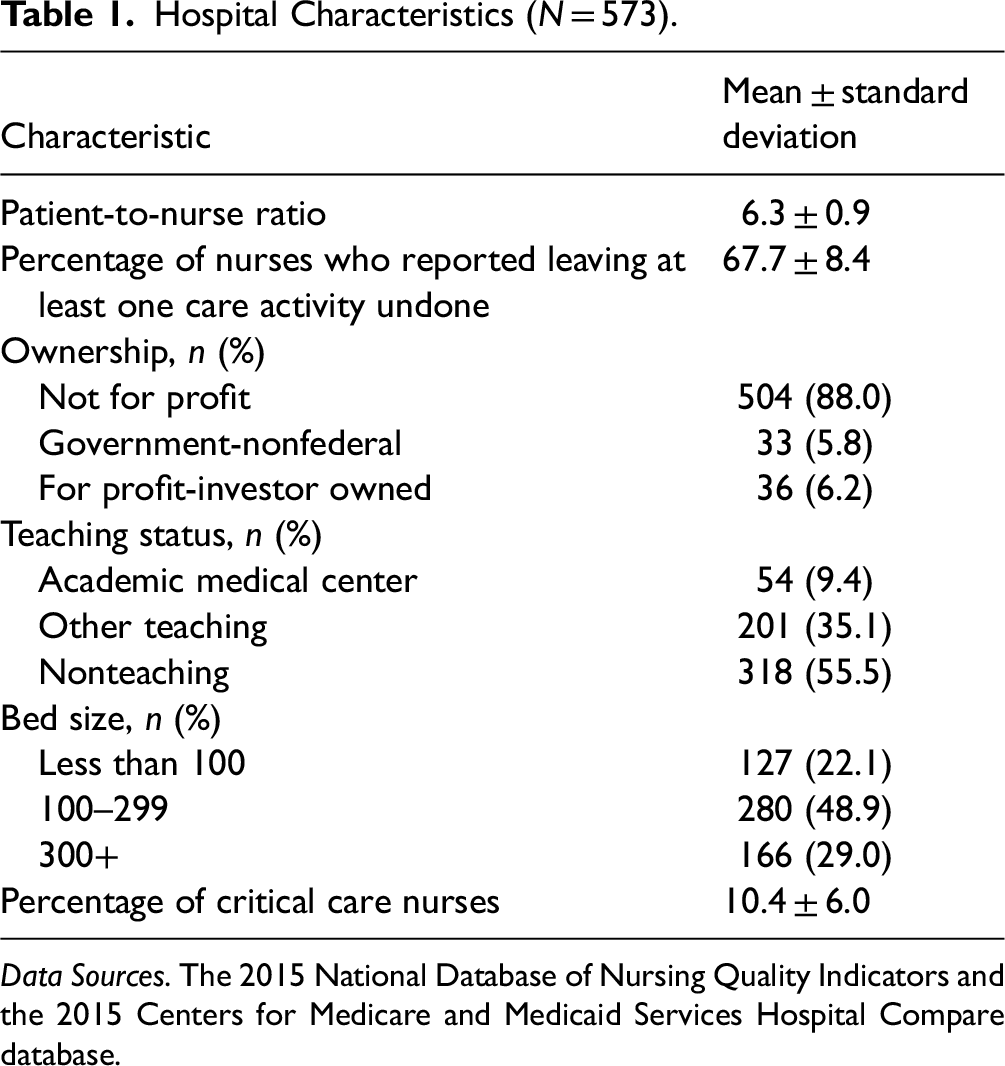
Data Sources. The 2015 National Database of Nursing Quality Indicators and the 2015 Centers for Medicare and Medicaid Services Hospital Compare database.
Percent of Nurses Reporting Missed Care by Nurse Staffing
Figure 2 shows the overall percentage of nurses who reported missing specified care activities by nurse staffing level. The overall percentage of nurses missing any care was 67.7%. As the patient-to-nurse ratio increased, the percentage of nurses missing care also increased, with percentages of 63.6% for a ratio of less than 5.5, 67.9% for a ratio between 5.5 and 6.0, 69.1% for a ratio between 6.0 and 6.5, and 68.6% for a ratio over 6.5. Comforting and talking with patients had the highest percentage of missed care, ranging from 32.2% to 37.4% across different staffing ratios. Other tasks with notable percentages of missed care included teaching and counseling patients and families (22.8%), adequately documenting nursing care (17.8%), and ambulation or range of motion (16.5%).
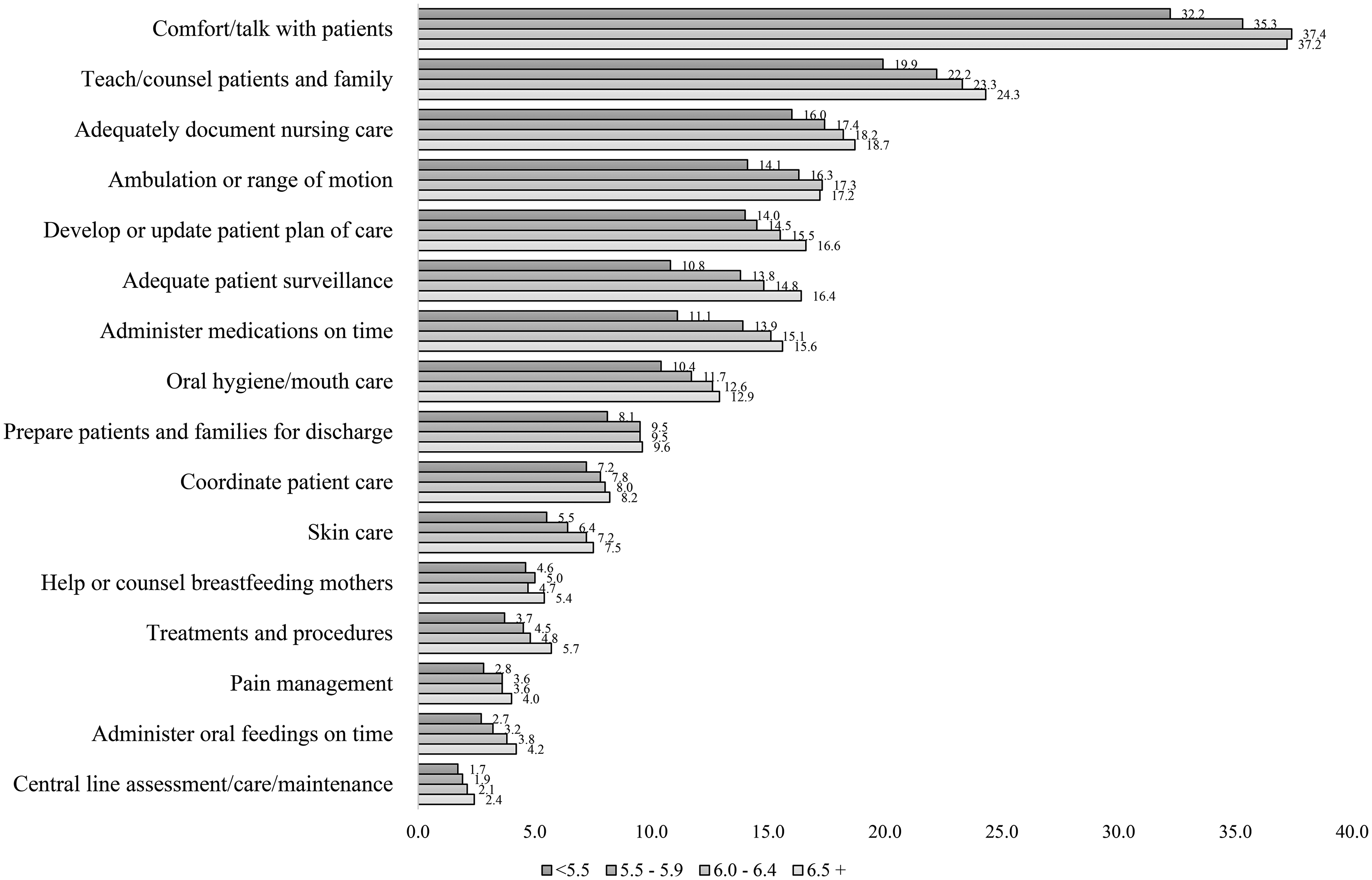
Hospital-level percentage of nurses reporting missed care by patient-to-nurse ratio (N = 573).
Percent of Patients Readmitted by Nurse Staffing Levels
Figure 3 displays the percentages of patients readmitted for various primary diagnoses by nurse staffing levels. Most patients were readmitted with a primary diagnosis of heart failure, with the percentage readmitted ranging from 21.4 to 22.2 (mean: 21.7). Chronic obstructive pulmonary disease also exhibited high percentages of readmitted patients, ranging from 19.6 to 20.2 (mean: 20.0). Conversely, the lowest percentages were observed among elective primary THA and/or TKA patients, ranging from 4.6 to 4.7 (mean: 4.6). For six out of the seven diagnoses, the highest patient-to-nurse ratio category had a higher percentage of patients readmitted compared to the lowest patient-to-nurse ratio category.
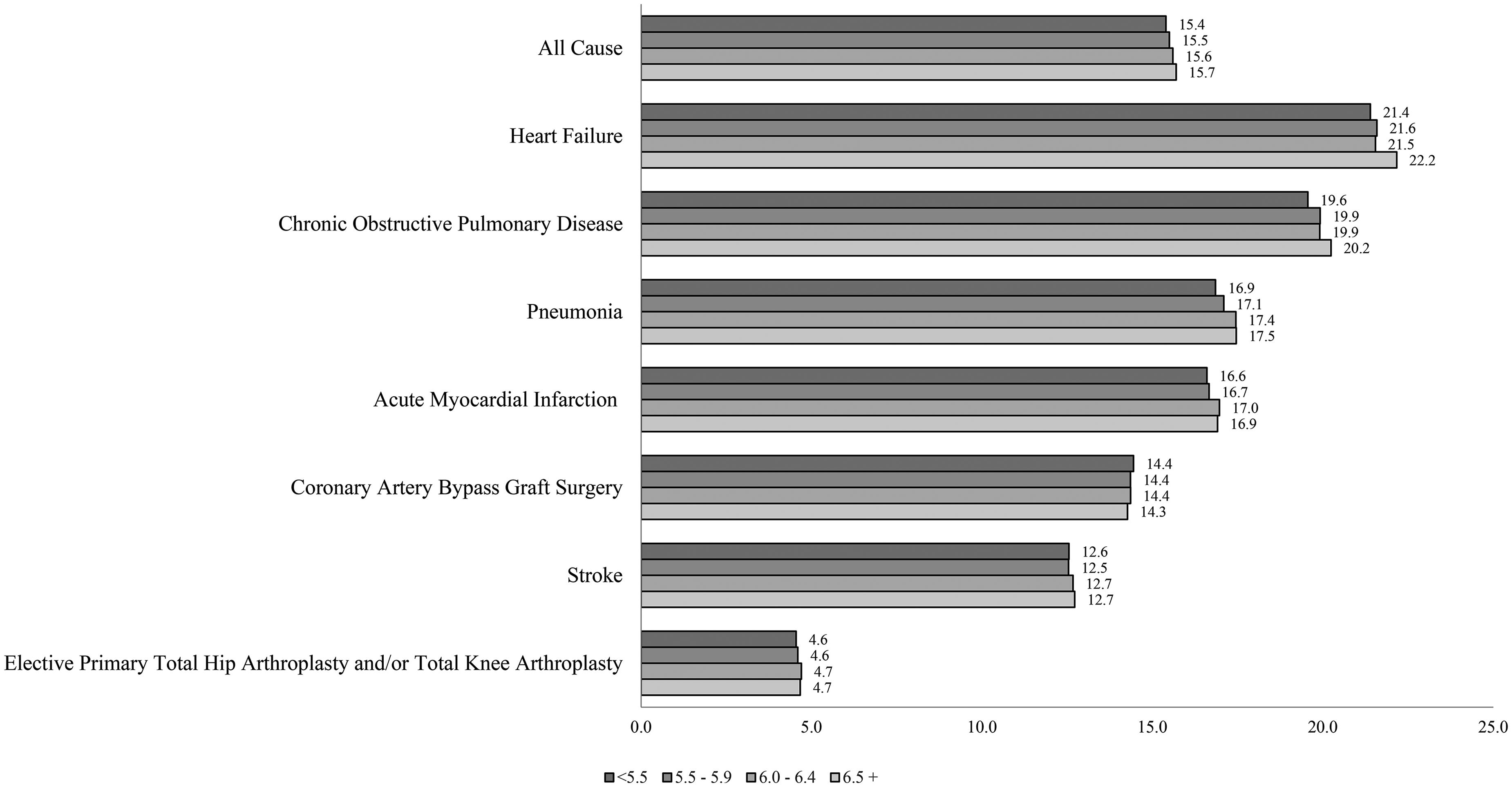
Hospital-level readmission rates by patient-to-nurse ratio (N = 573).
Mediation Analysis
A summary of the mediation analysis is provided in Table 2. The patient-to-nurse ratio at the hospital level had both statistically significant direct and indirect associations with hospital-wide all-cause 30-day readmission rates. A higher patient-to-nurse ratio was directly associated with higher hospital-wide 30-day readmission rates, independent of the percentage of nurses who reported leaving at least one care activity undone (b = 0.16, p < .001). Additionally, there was a significant indirect association. A higher patient-to-nurse ratio was linked to a higher percentage of nurses reporting missed care, which in turn was associated with increased readmission rates (b = 0.02, p = .006). The percentage of nurses reporting missed care accounted for approximately 10% of the total association between the patient-to-nurse ratio and hospital-wide all-cause 30-day readmissions.
Direct and Indirect Associations Between Nurse Staffing, Missed Nursing Care, and Hospital Readmission (N = 573).
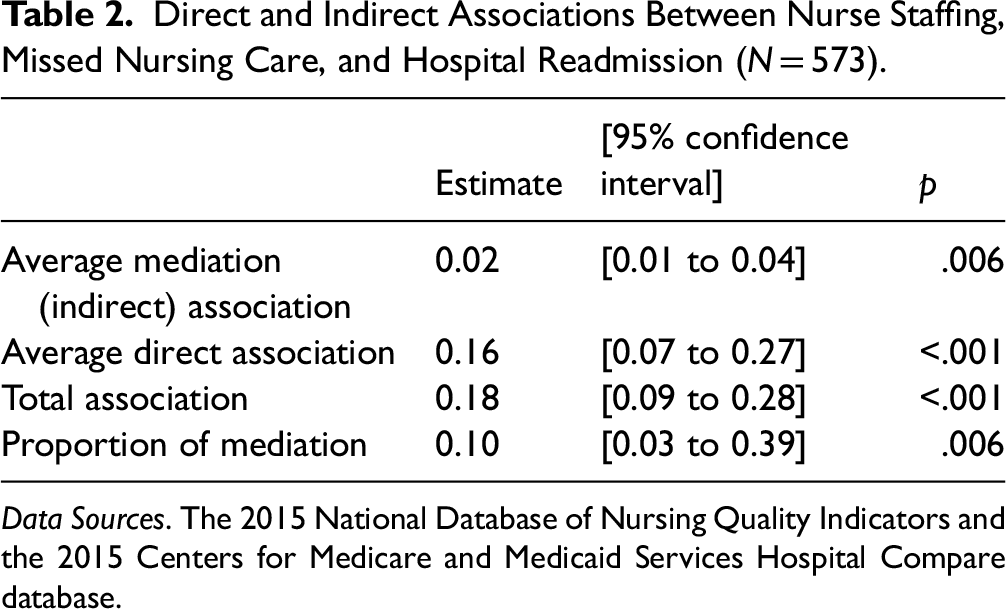
Data Sources. The 2015 National Database of Nursing Quality Indicators and the 2015 Centers for Medicare and Medicaid Services Hospital Compare database.
Discussion
This study provides valuable insights into the relationships between nurse staffing, missed care, and readmission rates in U.S. hospitals. The two key findings are: (a) nurse staffing is directly associated with missed care and readmissions and (b) missed care accounted for 10% of the total association between nurse staffing and all-cause 30-day readmission. These findings are consistent with existing literature which has consistently shown that understaffing leads to the omission of critical nursing activities (Kalisch et al., 2011b; Lake et al., 2020), which in turn has negative consequences for patient safety, patient satisfaction, and nurse job satisfaction (Kalisch et al., 2011a; Papastavrou et al., 2014; Recio-Saucedo et al., 2018; Schubert et al., 2008).
The first key finding that nurse staffing is directly associated with missed care is likely due to the fact that nurses with heavier workloads have less time to spend with each individual patient and are more likely to prioritize certain tasks. Our study findings are substantiated by Kalisch et al. (2011b) who similarly found a negative association between missed care and the staffing measure hours per patient day. Our study found the care activities most commonly missed include comforting and talking with patients and teaching and counseling patients and families. These findings are consistent with the literature, which similarly finds that talking to and comforting patients is most frequently reported as missed (Griffiths et al., 2018). Moreover, similar to the findings of Lasater and McHugh (2016), our study further establishes a direct link between nurse staffing and the rate of patient readmissions for a wide variety of medical conditions.
The second key finding was that missed care is one of the mechanisms explaining the relationship between nurse staffing and readmission. This finding extends prior evidence that missed care mediates the relationship between staffing levels and measures of patient satisfaction (Bruyneel et al., 2015) and falls (Kalisch et al., 2012). This is the first study we know of, however, to extend the implication of missed care as a mediator of staffing effects into the posthospitalization period.
This study contributes significantly to the conceptual understanding of how nurse staffing levels affect patient outcomes. By uncovering the process through which inadequate staffing leads to missed care and subsequently affects patient outcomes, this research provides a deeper insight into the mechanisms at play. This process-oriented perspective extends beyond the well-known direct relationship between staffing and outcomes, offering a more nuanced understanding of the impact of nurse staffing on healthcare quality and patient safety.
Given the significant amount of missing data related to hospital readmissions categorized by condition-specific diagnoses, we used all-cause 30-day readmission as the primary outcome to ensure a more complete and representative analysis. However, future research is needed to investigate whether the mediating role of missed nursing care varies by specific patient diagnoses, as different clinical conditions may involve distinct care needs and pathways to readmission.
Missed care can substantially heighten the risk of hospital readmission for several key reasons. Firstly, it often results in inadequate patient education and discharge planning. This omission may leave patients ill-prepared to manage their conditions at home, potentially leading to complications and a subsequent readmission (Oh et al., 2021). Secondly, it may interrupt the care coordination process, preventing a seamless transition to postdischarge healthcare and social services (Rosen et al., 2018), thereby increasing readmission risk. Thirdly, it may result in a lack of ongoing surveillance, which can mean complications such as infections are not identified promptly (Halverson & Scott Tilley, 2022), potentially requiring patients to be readmitted for treatment. Notably, the most frequently overlooked care activity, engaging in conversation and providing comfort to patients, underscores how unresolved issues during the hospital stay can escalate after discharge, further increasing the likelihood of readmission.
The broader implications of staffing levels, both directly and indirectly, complicate the management of readmission risks. While our findings highlight the direct impact of nurse staffing on readmission rates as being more significant than missed care, the quality of care may also suffer from nurse burnout caused by understaffing, potentially affecting the overall care quality. This issue is not limited to nurses but may also involve other critical staff such as social workers, influencing postdischarge outcomes and readmission rates. Despite this, the necessity of addressing missed care alongside ensuring adequate nurse staffing remains paramount. An integrated approach that marries sufficient staffing with enhanced care processes is essential for effectively lowering readmission rates through improved nursing services.
This study's implications for healthcare practices and policy are comprehensive, highlighting the urgent need for systemic improvements. Ensuring sufficient nurse staffing levels is critical for healthcare administrators. Recognizing and addressing missed nursing care is essential for both managers and frontline nurses. Missed care not only exacerbates the negative effects of insufficient staffing but also demoralizes nurses striving to meet high care standards. It is essential for administrators to cultivate an environment that supports high-quality care by empowering nurses with decision-making authority, access to necessary resources, and supportive work conditions, including effective nurse management. Additionally, stronger care coordination, transitional care models, and family caregiver education and supports should be integrated as distinct interventions to reduce missed care and avoidable readmissions (Chartrand et al., 2023; Levoy et al., 2022; Morkisch et al., 2020; Rodakowski et al., 2017). Policy changes at the federal level such as those suggested by the Centers for Medicare and Medicaid Innovation, should be considered. For example, testing an alternative payment model for hospital nursing could incentivize better staffing and care practices. These actions are key to decreasing missed care occurrences, enhancing nurse satisfaction, and reducing turnover rates (Lake et al., 2019).
Limitations
This study has some limitations that are important to consider. The cross-sectional design restricts our ability to infer causality, highlighting the need for caution when interpreting the findings. Additionally, our reliance on U.S.-based, hospital-level data limits the applicability of our conclusions to healthcare systems in other countries. While the integration of data from diverse sources strengthens our analysis, potential biases exist within those sources. For example, hospitals participating in the NDNQI might be more likely to have superior staffing and outcomes, due to the disproportionate participation of Magnet hospitals and hospitals interested in monitoring nursing quality indicators in the database. This selection bias makes our results most applicable to hospitals with characteristics similar to those of our sample. Despite these limitations, our study provides valuable insights and paves the way for future longitudinal research in representative samples to definitively establish causal relationships.
Conclusion
This study provides valuable insights into the relationship between nurse staffing, missed care, and readmission. The findings suggest that missed care plays a mediating role in the relationship between nurse staffing and readmission. Healthcare organizations can implement strategies to optimize nurse staffing levels and develop targeted interventions to reduce missed care and patient readmissions.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Nurses Foundation, Division of Cancer Prevention, National Cancer Institute (Grant No. The Margretta Madden Styles Credentialing Research, 1KM1CA156715).