
Abstract
In the United Kingdom, significant ongoing inconsistency exists in wound care nursing education provision and practice. Health economists have identified this to be a major cause of the burgeoning economic and personal cost of successfully, and equitably, healing chronic wounds. While numerous wound care educational resources exist, policies intended to implement a program of reform or change are for some reason not filtering down to, or being implemented by, those who need them most. Policy making processes do not appear to be operating as efficiently as they should, and this merits further scrutiny. A critical discourse analysis of two UK professional body wound care policies provided an innovative insight into the effect of policy production to the research problem. The overarching construct of “Aspiration and Resolution” and its subconstructs were identified. Links between data, analysis, and conclusions were established using Greckhamer and Cilesiz’s (2014) framework to address criticisms over lack of transparency in critical discourse analysis methodology. Findings indicate wound care policy makers must adopt an active, not passive, approach to policy making. An active position, compared with the inertia that appears to currently exist, would take into consideration the capacity to implement policy and not merely increase awareness or disseminate. Wound healing policy making agencies need to make decisions on how to disseminate and implement policy. Active policy making would also adopt target audiences’ decisions to implement policy, instigate activities to improve knowledge and skills, facilitate change, and ensure continued use of policy as part of organizational operations.
Background to Study
Although the topic of wound healing has always been important to nursing, it is reasonable to ask why, in the current strained economic climate in the National Health Service (NHS) in the United Kingdom, when far greater strategic health care priorities such as cancer, stroke, maternity and neonatal health, diabetes, mental health, and respiratory care (Alderwick & Dixon, 2019) are arguably all competing for limited resources, wound care should now take on more significance. Drivers for change are directed toward reducing societal economic costs, patient care inequalities (Academic Health Services Network, 2019), and increasing quality of life.
In the United Kingdom, wound care has more recently attracted attention because of the vast economic costs attached to its management, which have only relatively recently been identified. These costs relate mainly to chronic wounds and the often devastating and damaging effects of living with a wound on a person’s quality of life (Guest, Ayoub, et al., 2017). This economic burden is still considered to be an underestimated “guestimate.” Supported by the research findings of others (Järbrink et al., 2017; Nussbaum et al., 2018; Phillips et al., 2016; P. Vowden & Vowden, 2016), this has focused the minds of government policy makers and health care managers. The increasing costs of chronic wounds to the UK economy and patient quality of life are now thought to be significant (Phillips et al., 2016) and are also being recognized elsewhere. In Australia, for example, Kapp and Santamaria (2015) view such costs as a largely hidden and poorly supported problem. The current cost to the UK health service is £5.3 billion, and, in 2012/2013, approximately 2.2 million wounds were being managed in the United Kingdom (Guest et al., 2015). The need for effective wound management is now believed to be a priority health care policy agenda item in the United Kingdom (Courtenay et al., 2018), and Guest calls for the development and implementation of strategies to improve diagnosis accuracy and healing rates, making a clear link between this and clinical and economic benefits (Guest et al., 2015; Guest, Vowden, et al., 2017).
Wound care is complex (K. Vowden, 2005). It is well established that many factors are responsible for effective wound management (Hess, 2011). A number of key academics and opinion leaders, and, more recently, health economists, believe that a fundamental cause of this excessive financial burden is the substantial variation that exists within education, wound care practice, and the lack of role definition. Guest, Ayoub, et al. (2017), for example, recommend that the different roles of professionals across health care, including tissue viability nurses, need to be much more clearly defined within the patient care pathway. The consequences of this lack of clarity in role are exacerbated because, as observed by Ousey et al. (2015), there is no unifying definition for the role of those working within tissue viability, nor is there a nationally recognized criteria to determine the educational level that must be reached before someone can work in this role. Such discrepancies are thought to be contributing factors to upholding professional standards in wound care (Ousey et al., 2014, 2015; White, 2008; White et al., 2016). The European Wound Management Association has recently finalized the first curriculum in a series of several curricula intended for use in levels 5–7 of the European Qualifications Framework (Pokorná et al., 2017; Probst et al., 2019). The aim of these is to support a common approach to postregistration qualification in wound management for nurses across Europe, and the European Wound Management Association hopes to work toward a close collaboration with European nurse organizations as well as educational institutions to implement these common curricula. However, as this curriculum is proposed for incorporation into existing programs in different European countries, specific details of the teaching and learning methods and assessment and evaluation methods are not included. It is recommended these should follow whatever structure is used by each education provider while incorporating the content and learning objectives provided in this curriculum according to local legislation and procedures. In addition, guidelines and best practice statements are available as educational resources; however, their dissemination and implementation as Ousey et al. (2011) have previously identified appears to be a barrier in that “staff need to be aware of their existence to provide evidence-based care” and “must ensure all practitioners are familiar with this and integrate it into educational programmes” (p. 147).
Highlighting her concerns about the lack of role definition and nonexistence of a skills or knowledge framework that can act as a benchmark for services, Ousey et al. (2014) supports Guest’s earlier concerns regarding the financial consequences and undesirable effects for quality of life, leading to the conclusion that there is an urgency to account for these numerous deep-rooted existing organizational and clinical policy differences and to identify viable options in higher education. These observations confirm Flanagan’s (2005) earlier concerns regarding the existence of organizational and interprofessional rivalry as being significant obstacles to reaching much-needed consensus in wound care education. In this regard, the increasing presence of industry in driving educational material and the potential conflict of interest that may underlie industry developing such materials must also not be ignored.
It can therefore be deduced that, while numerous valuable wound care educational resources exist, the policies or “action plans, positions, and/or guidelines”(Mwije, 2013, p. 1) designed to implement a program of reform or change are for some reason not filtering down to or being implemented by those who need them most. Policy making processes do not appear to be operating as efficiently as they should, and this merits further scrutiny.
Defining Policy
Although the policy making process is often reduced to six stages—problem identification, agenda setting, policy making, budgeting, implementation, and evaluation—this is a simplification. Policy can have different interpretations, and its definition in education and health contexts varies significantly (Ball, 1993, 2017). The process is also understood to be “incoherent,” “ill-defined,” and “complex,” characterized by numerous “inputs” and “outputs” (Mwije, 2013), and such complexity does not bode well for policy in health care, which is notoriously multifaceted. As indicated by Bowen and Zwi (2005), policy does not therefore operate in isolation because it consists of political, social, historical, and economic elements that are particularly relevant to the health care system context.
To understand how wound care issues get onto policy agendas, how policy makers treat evidence, and why some policy initiatives are implemented while others fail, for the purposes of this research, this paper draws on Buse, Mays and Walt (2005) definition of policy, which sees it as “courses of action (and inaction) that affect the set of institutions, organizations, services and funding arrangements of the health system” (p. 6). In this context, policy can be made within government, by nongovernment actors, and by organizations external to the health system (Walt & Gilson, 1994) with an impact on health.
Research Methodology—Critical Discourse Analysis
This CDA was undertaken in part contribution to a Doctorate in Education (EdD) thesis by the first author'. This article addresses one component of the CDA in that it pertains only to those wound care policies where policy production macrostructures—those processes involved in the creation of a text (Fairclough, 1989)—are considered. Critical discourse analysis (CDA) is essentially an explanatory, interpretive, and descriptive process of deconstructing reading. CDA is discipline- and context-specific (Weiss & Wodak, 2003) and emphasizes the way in which language is drawn into matters such as power and ideology, which control how language is used, its effect, and how it reflects, serves, and advances the interests, positions, views, and values of those in power.
Despite the general use of CDA in education and sociology, nursing policy research employing CDA methodology is sparse but nonetheless, as suggested by Evans-Agnew et al. (2016), represents a promising methodology for policy research in nursing education. This deficiency may well be due to its inexact approach and criticisms over its methodological shortcomings as expressed by Breeze (2011).
From a teacher activist stance (Niblett, 2017), my rationale for using CDA to explore policy production specifically was to understand how wound care nursing education policy’s discursive practices—“processes of text production, distribution and consumption” (Fairclough, 1992, p. 78)—might be complicit in creating apparent power relations and inequity between policy producers such as nursing regulatory and professional bodies and wound care educators and wound care nurses. Controlling how these relationships are created asserts power through their use of language. CDA has not previously been used to investigate wound care education policy making processes and therefore offered new insight in to this underresearched aspect of wound care education and practice.
CDA has been defined as a “problem-oriented interdisciplinary research movement” (Fairclough et al., 2011, p. 357), which can be enacted through a wide spectrum of different approaches, employing different methods and driven by different theoretical perspectives. Therefore, unlike most research methods in nursing, CDA is not a single methodology or a fixed method and has no unitary theoretical framework or specific guidelines to follow. Instead, each methodological approach to CDA is grounded within a theoretical framework in relation to the nature of discourse and the relationships between discourse, knowledge, and power (Potter & Wetherell, 1987; Wodak & Meyer, 2001). From a CDA position, discourse preserves social patterns such as authority, discrimination, exploitation, dehumanization, naturalization (ideologically driven) “common sense,” unless its usually hidden effects are exposed so that awareness, resistance, emancipation, and social action can bring about social change and social justice (Waugh et al., 2016). In CDA, discursive practices are thought of as “social practices”—bodies of structured, usually institutionalized, activities, that are mediated through language. I therefore considered the particular economic, political, and institutional settings where wound care policy discourse is generated, such as government, professional bodies, and regulatory social structures, alongside their conventions.
Data Handling Process
Similarly, to the nonprescriptive “little toolbox for constructing discourse analyses” described by Jäger (2001, p. 52), Chilton (2004), Fairclough (1992), Manias and Street (2000), and Rheindorf (2019) which can be adapted to researchers’ own needs and tailored to fit their concerns (Schneider, 2013), I built a bespoke analysis framework to specifically address the wound care nursing context. This format allowed me to take account of the key issues relating to professional regulation, institutional change, marketization, power, and society, with the design driven by the problem at the center of the research problem and the discourses presented and analyzed according to the power relations uncovered. For the purposes of this thesis, I use wound care-related policy discourse as the central concept and view the policy process not simply as text but, as Bowe, Ball and Gold (2017) suggest, as production, reification, implementation, and interpretation. I approached the CDA process objectively, systematically treating, as Adams and Thompson (2011) suggest, each policy document and its contents as “participants.”
Policy Selection
Fairclough suggests that texts selected for CDA should demonstrate the existence of ideology and power relationships, meaning that not all texts are eligible for analysis. CDA positions ideology as “constructions of reality” (Fairclough, 1992, p. 87); they are representations of the world which play a powerful role in establishing and shaping social relations of power and domination. In CDA, language is considered as one way through which ideologies are constructed, maintained, and challenged, but the meaning of this language can only be understood through interpretation and reinterpretation of text (Fairclough, 1992). Meaning is therefore not always initially forthcoming and cannot simply be “read off.”
Adopting Fairclough’s interpretation of ideology, through a process of purposive snowball sampling (Gentles et al., 2015) using my own professional knowledge of key regulatory and professional body policies, I identified five nursing and wound care-related policy texts representing the wound care organizational “order of discourse.” Spanning across different discourses, genres, and styles, this selection represented the discoursal element of what Fairclough (2003) refers to as the “network of social practices” (p. 220). I reduced this sample further to enable the analysis to focus on two texts related specifically to wound care (Policies 1 and 2, Table 1), thereby omitting texts related to nursing more widely (Policies 3, 4, and 5, Table 1). Although the sample population of relevant education policy text from government and wound care nursing professional bodies was small, it is typical for CDA to involve only a few texts—even just one or two. I believed this sample to be representative of those policies that best aligned with the research objective.
Policy Documents Included in the Macrostructure Aspects of the CDA.
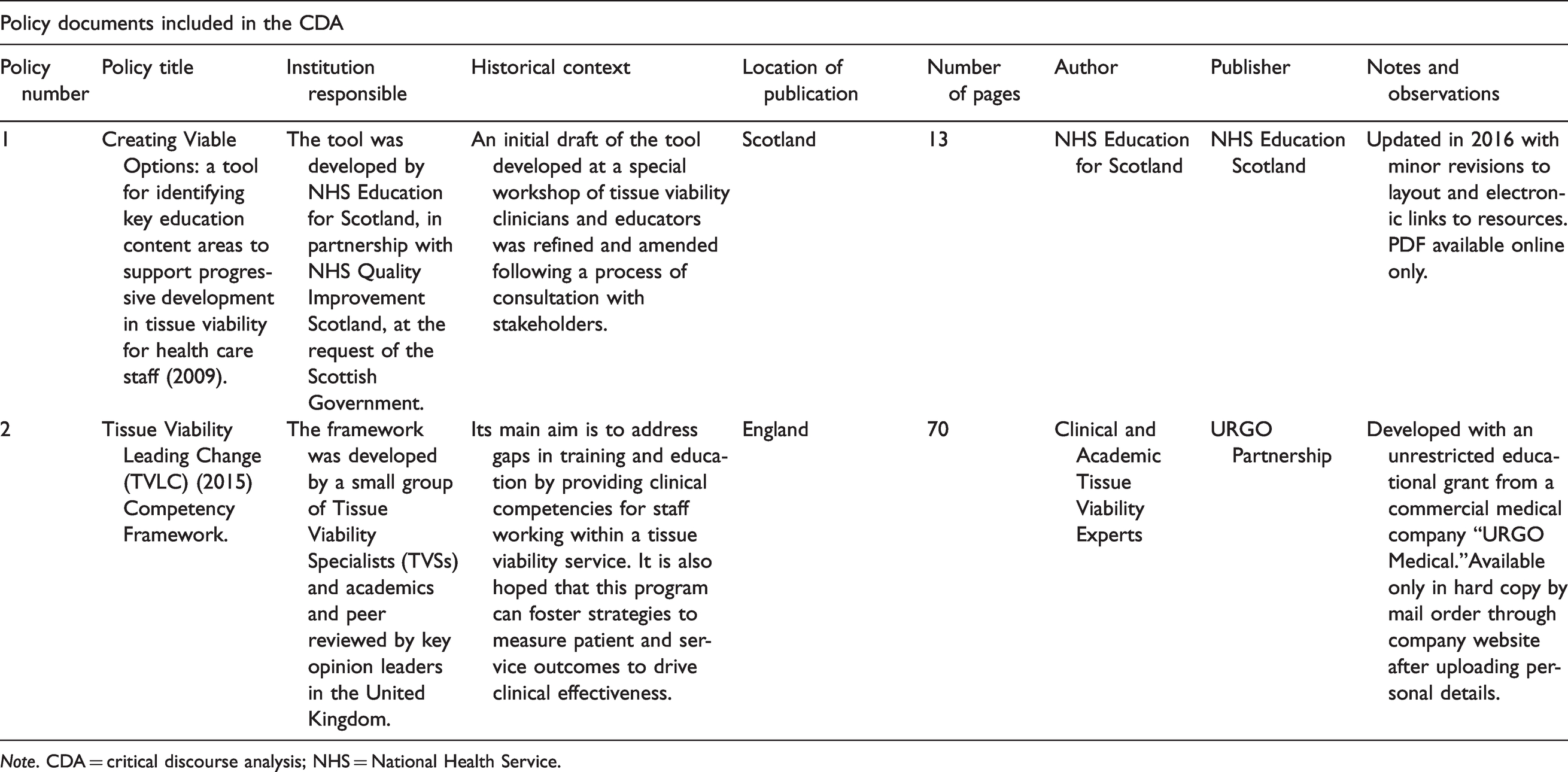
Note. CDA = critical discourse analysis; NHS = National Health Service.
The first selected text was Creating Viable Options (NHS Education for Scotland [NES], 2009), which provides guidance for organizations and individuals on preparing education and development programs on tissue viability. It should be noted that an updated version of this text was published in 2015 and this version was included in the analysis (NHS Education for Scotland [NES], 2015). It sets out key content areas for education to support progressive development in tissue viability expertise for health care staff as they progress through their careers. It was developed by NES, in partnership with NHS Quality Improvement Scotland, at the request of Scottish Government.
The second selected text was Tissue Viability Leading Change (TVLC) Competency Framework (URGO Partnership, 2015), which is a framework developed by a small group of tissue viability specialists and academics. Its main aim was to address gaps in training and education through the development of a number of measurement tools to drive clinical effectiveness. This included the development of clinical competencies for staff working within a tissue viability service and strategies for measuring patient and service outcomes. It is interesting to note that it was developed through an unrestricted educational grant from a commercial medical company URGO Medical.
Although the sample is small, it represents both ends of the wound care education spectrum: public and private. Although these two key actors operate in the same context, they do so through different channels, with different processes and are driven by different goals. It was important for my sample to capture this disconnect and the complexity and tension that this creates within the field.
Machin (2013) recommends that CDA analysts provide complete and accurate descriptions of each document because this permits a more complete and accurate analysis. As shown in Table 1, I included the social and historical context in which each of these policy documents was produced alongside the source, place, authors, date, size, publisher, and location of publication for each document. After policy selection, I viewed each text as a “link in a chain of texts, reacting to, drawing in and transforming other texts” (Fairclough & Wodak, 1997, p. 262) and examined the relationship that existed between them, or their “intertextuality” (Fairclough, 1992) because, as Grant and Hardy (2004) and van Dijk (1987) suggest, it is meaningless to analyze them in isolation and generate related understanding in separate texts. Morgan (2010) argues that CDA only has a relevance and practical application at any given time, in any given place, and for any given people and is context-specific. To help frame the document selection in this way, I first approached the text in an uncritical neutral manner, then again with a more critical analytical approach. During these subsequent readings, I revisited the text at different levels, raising questions about them, imagining how they could have been constructed differently, and mentally comparing them with related texts.
Data Analysis Method—Building the Data Analysis Framework
I developed a tabulated matrix using Word (Table 2) to satisfy the unfolding nature of the method and various redrafting. The hands-on and tactile nature of the analysis process, involving “chopping and changing” notes of paper, somehow brought me closer to the data. Greckhamer and Cilesiz (2014) warn that, given its interpretive nature, it is possible to challenge discourse analyses on the process by which conclusions are reached. I therefore ensured the framework built made links between data, analysis, and conclusions transparent by using this tabulated discourse analysis process. After critiquing numerous cycles of the policy’s discourses and seeing concepts emerge, as in the approach taken by Greckhamer, I developed a rubric, an extract of which can be seen in Table 2. The two rows were numbered according to the policies in Table 1, and the six columns were labelled as follows: policy number, policy name, data unit in context, data unit, concept, and construct (including subconstructs). This matrix format also shows how data “anchors” (text excerpts) connect to data units (specific points of reasoning or concepts), then to constructs and supporting subconstructs. This chronicling process involved multiple cycles and, although the framework appears to represent a linear process of moving from the data to the constructs, like any representation, it is an oversimplification of the analysis process. However, it shows enough to convey the logic of my interpretations and the analysis process.
Extract of CDA Rubric (Based on Greckhamer & Cilesiz (2014) Framework).
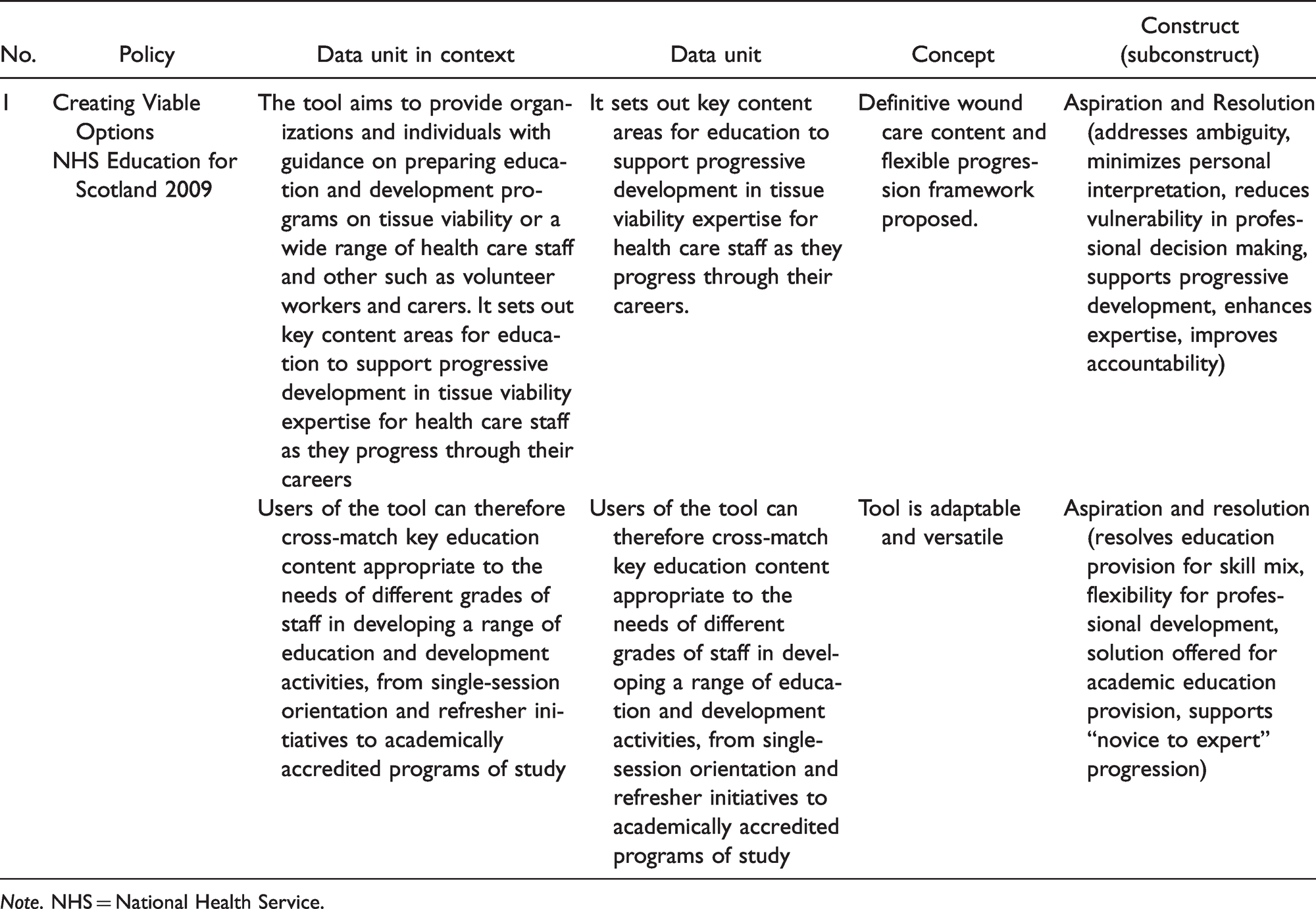
Note. NHS = National Health Service.
I viewed each text as a “link in a chain of texts” (Fairclough & Wodak, 1997, p. 262) that reacted to, drew upon, and transformed other texts. I also considered intertextuality—the relationship that existed between the policies. The cells were then populated with the associated data, and I identified the working concepts and generated constructs using the coding process outlined later.
Process of Coding Text Data
After categorizing the policies according to their macrostructures, I started the coding process. After several “analysis revolutions,” or cycles of independent analysis involving identifying, verifying and refining (by means of merging, splitting, changing, and adding), I identified separate “data units” that I then conceptualized. To help create congruence with the research background and research question, I included the original context from which the data units were extracted.
Creating Constructs From Discourse
Through the process of identifying the “data units” and the general concepts they represented, I classified similarities before categorizing these into the overarching construct of Aspiration and Resolution and its subconstructs (Table 3).
Overarching Construct and Subconstructs Relating to Policy Macrostructures.
Analysis
This construct of Aspiration and Resolution considers the consultation, ownership, and distribution features of the policy production macrostructures, those processes involved in the creation of a text (Fairclough, 1989). To understand the meaning of actions as a whole, how parts related to one another, and general models of textual development, I used the following macrostructures: (a) Under what circumstances were the texts produced? (b) Who produced them? (c) For what purposes were they produced? (d) What constraints were placed on text production?
Under what circumstances were the texts produced?
Only one government and one professional body policy text (Policies 1 and 2) were identified. At the time of selecting the Policy 1, Creating Viable Options—a tool for identifying key education content areas to support progressive development in tissue viability for health care staff—was fairly outdated, but has, during the course of this research, since been revised with very minor amendments (NES, 2009/2015). The low number of texts identified was peculiar because it was at odds with the escalating economic and public health concerns identified. The origins, enactment, and implementation of these policies were arguably determined by and dependent on the agenda priorities of their producers. In Policy 1, for example, tissue viability was identified as a priority. However, a closer inspection of the circumstances under which it was produced shows that this emphasis was more of a “one-off” event, with wound care only one component of a wider strategic government quality improvement initiative taking place at the time. Extant today, with only minor amendments in 2015, this policy remains the only credible “go to” resource for wound care educators and practitioners in Scotland.
The presence of industry in wound care education in Policy 2 is worthwhile to note. Production of Policy 2—TVLC Competency Framework (URGO Partnership, 2015)—was only made possible as a result of private investment, because of “an unrestricted commercial educational grant and other commercial sponsorship” (URGO Partnership, 2015, p. 7) and not through the allocation of public funding for wound care. This observation is reminiscent of the pharmaceutical industry some years ago, where nurses became a consumer target for a powerful industry and, arguably, wound care might be entering a similar realm. The pharmaceutical industry was widely criticized for exploiting health care professionals by using a range of techniques, including sponsoring similar teaching materials and research funding.
Neither producers claim responsibility for enactment, implementation, enforcement, or evaluation of their policies.
b. Who produced them?
The “acknowledgments” in policy documents are generally not read, let alone analyzed, so adopting a CDA perspective on these sections provided unique and unusual insights into policy ownership and the “tribalism” that appears to exist, affecting policy production and enactment.
Since devolution in the late 1990s, the NHS is no longer one large body responsible for the whole of the United Kingdom—health and social care are now organized and funded by the devolved governments in Wales, Northern Ireland, and Scotland. For example, in England, NHS England is the umbrella body that oversees health care and is an independent body, which means that the Department for Health cannot interfere directly with its decisions. Clinical Commissioning Groups are responsible for commissioning health care for their local areas. In Scotland, health services are devolved to the Scottish Government and cover 14 regional health boards across Scotland. Their role is roughly equivalent to that of Clinical Commissioning Groups in England in that they plan and deliver health services based on the needs of local communities.
A “top-down” approach to instigating the wound care policy agenda in Scotland is apparent in Policy 1, as its production was instructed “at the request of the Scottish Government,” who then worked in partnership with NHS Quality Improvement Scotland over the production. However, the tissue viability clinicians, educators, and stakeholders involved in its development are not credited anywhere for their contribution to the final document, and mention of their role is limited to the first draft. In contrast, in Policy 2—Tissue Viability Leading Change—acknowledgments and details of the authors and extensive list of peer reviewers are publicized, with those involved personally credited, with their job titles and employers noted.
A further interesting discrepancy can be found in the geographical representation of Policy 2. This policy commits to “promoting equity and transferability of expertise across the UK” (URGO Partnership, 2015, p. 3), but the development team, with the exception of one representative from Wales, worked in England, and there is no representation from Scotland or Northern Ireland. This is suggestive of the organizational and interprofessional rivalry previously witnessed by Flanagan (2005) and a tangible example of “tribalism” within the wound care community. Given the extent of the unrestricted commercial educational grant made available, it is arguably remiss that this occasion was not viewed as an opportunity for much wider collaboration across the United Kingdom to enhance more widespread continuity. Similarly, in Policy 1, it is implicit that this policy was produced and promoted solely for Scottish practitioners and not considered as a UK-wide initiative.
An interesting feature to note is that wound care policy was apparently developed through commercial investment.
c. For what purposes?
Both documents appear to be dependent on control over the wider nurse education agenda.
While tissue viability was high profile in Scotland in the 2008 to 2009 period, this was only as part of a wider initiative in which the tool was developed by NES, in partnership with NHS Quality Improvement Scotland, at the request of the Scottish Government. Since this time, although the presentation has been updated, the content itself has not changed to any great extent.
Similarly, Policy 2 relied on the availability of the commercial interests of wound care product sponsorship at that time, and it remains to be seen whether such a quality document, in terms of its content and appearance, would have occurred in the absence of these interests.
d. What constraints were placed on the production of the text?
The producers of Policies 1 and 2 do not claim to have a mandate for policy enactment or assign responsibility for its distribution and implementation to any particular entity. The extent to which, for example, those with wound care education responsibilities working in higher education are familiar with their existence or indeed whether they have been implemented or evaluated remains unknown.
Follow-up research by Ousey et al. (2016) demonstrates a low uptake of the TVLC policy. This suggests this policy has not, for the moment at least, been adopted nationally. A growing dependence on commercial sponsorship to deliver a national wound care framework poses certain professional ethical problems, particularly when nurses are expected to trade their professional and personal data in exchange for access to vital knowledge.
Discussion
Selected features of Fairclough’s CDA framework (Fairclough, 1989) were used to help guide the discussion. This framework consists of three interrelated processes of analysis, each tied to three interrelated dimensions of discourse (Figure 1). Each dimension requires a different kind of analysis.
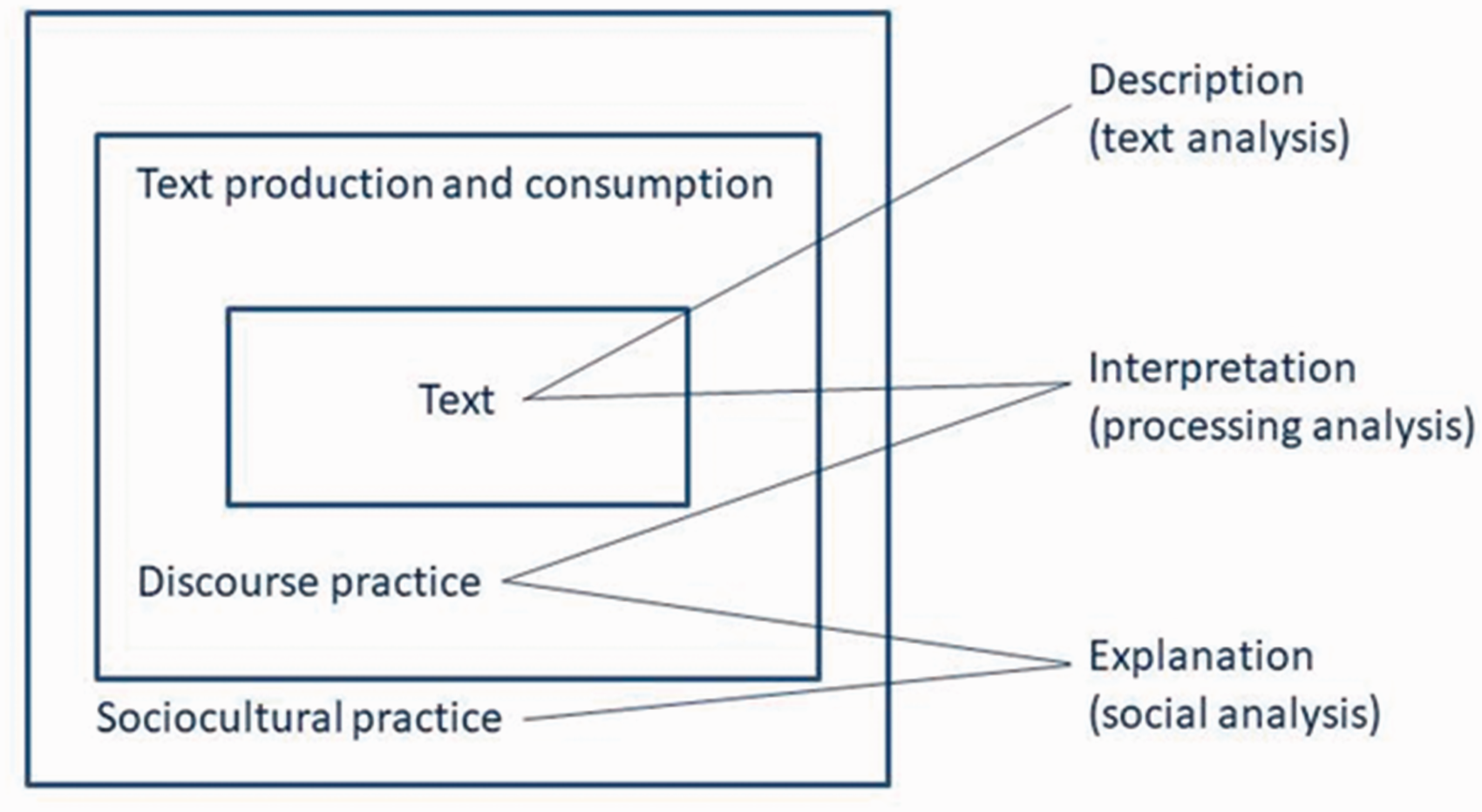
Fairclough’s CDA Framework (From Locke, 2004, p. 42).
Both policies have in common a “shared knowledge” about the world they inhabit, allowing them to work together and minimize conflict or misunderstandings. Theoretically, this position should empower policy producers to join forces and collaborate, but wound care education remains fragmented.
A lack of control is evident over ability to prioritize wound care as an agenda item, and there is an absence of accountability for policy enactment, both fundamental reasons for fragmented wound care education provision. Producers have arguably proliferated policy as and when it has suited them. However, access by practitioners to such vital learning resources and essential knowledge is lost because producers cannot, or perhaps do not wish to, legislate and take responsibility for its enactment and implementation.
Nonetheless, there are several examples where semantic evidence supports the ambitious intentions of both policy producers. In Policy 2, for example, the subjunctive mood is used extensively throughout. This is a linguistic technique used to explore the conditional or imaginary using indicative verbs (Table 4) to convey a hypothetical situation and a mood of hope and aspiration, not one of action, accountability or attainment. In this instance, “hoping” conjures up in the mood of those reading the policy a certain sense of abdication of any responsibility by the producers for its production so that the policy comes across as almost “released,” implemented at the mercy of current circumstances in education and practice.
Examples of the Subjunctive Mood Used in Policy to Convey Hope and Aspiration.
Furthermore, rather than policy supporting the preferred standardized approach evident in the background literature, this ambition is undermined because its content is described as nonprescriptive, subject to local variation, and for personal interpretation.
This knowledge and practice gulf between policy production and its implementation generates significant confusion around wound care nurses’ precise scope of practice, in turn compromising their professional accountability and fitness to practice. The power imbalance between policy producers, who arguably take no responsibility for enactment, and nurses, who are expected to access, interpret, and implement policy, is unfair and unjust.
In CDA, an important factor for all discourse and communication is who controls, and changes, the topic, much the same as when editors decide which news topics are covered in the media. Considering discourse as a form of social action, the government (Policy 1) and commercial organizations (Policy 2) can permit (or refuse) topic primacy. Policy 2, for example, gives no explanation for why the preexisting Scottish framework mentioned could not instead have been updated and rolled out across the United Kingdom, “although the National Association of Tissue Viability Nurses in Scotland has published core competencies for TV Nurses (2003), these are not used nationally across the UK” (URGO Partnership, 2015, p. 2)—or indeed why it was then necessary to initiate the commercially funded alternative.
This failure to reach national consensus on wound care education is further eroded because of the underrepresentation of contributors from across the country, and it is worthwhile considering here Fairclough’s idea of “power” (1995, p. 1), whereby people have different capacities to control how texts and thus discourses are produced, distributed, and consumed. In contrast to public services, the wound care industry, by virtue of funding, as shown in Policy 2, has demonstrated an innate capacity to own the means of production and power and is manifesting itself through the potentially insidious ownership of wound care education by bourgeois capitalist organizations (Marx, 2011). In addition, van Dijk (1995) notes that it is commonplace for social power and dominance to be well-organized and institutionalized as this allows for increased control and the reproduction of power structures through routine. He suggests that the power of industry in wound care is successful because it is reenacted in routine activities which are not questioned but instead regarded as normal.
In terms of acknowledgments, it is also worthwhile considering if there are ideological reasons why, unlike in Policy 2, the names and positions of those directly involved in the NHS policy consultation and production process are omitted in Policy 1. While some exclusions are “innocent” in that they are details that readers are assumed to know already, like Van Leeuwen (1996), we suggest that exclusion in this way, where particular social actors do not appear in a text, helps to obscure or downplay responsibility for a policy, meaning that any individual or group involved in the production cannot be apportioned blame.
The wound care discourse is influenced by social structures and shows the reproductive effects of the discourse on perpetuating or changing such structures. Four factors, explained below, relate to the production of wound care policy and have implications for wound care education and practice and represent powerful factors that influence the ways in which wound care policy is produced and enacted.
Agenda Sovereignty
Dominance over the wound care education and practice agenda is top-down—policy production is regulated by government and commercial agenda interests.
Control Over Access to Knowledge
Access relating to CDA is concerned with who has access to certain types of discourse or role and thus control over the access of other people. Access is therefore strongly related to power, and certain roles afford more access than others (van Dijk, 1995). For example, selection and representation of review members, timings of policy production, and choice of corporate investors all concern control of access. Access (or lack of it) therefore plays an important role in reinforcing existing power relations between recognized formal government and corporate organizations and wound care nurses. Lack of access to policies and their enactment is the greatest concern here, and the situation is perpetuated where the dominated group (wound care nurses), rather than resisting or condoning the situation, accept and comply with the status quo, legitimizing the power and even finding it “natural.”
“Trading” personal data in exchange for accessing valuable educational resources funded by commerce creates potential professional ethical issues. However, given the current restrictions of employer funding for continuous professional development (CPD) wound care education, such commercial interest adds weight to the tripartite partnership model previously suggested by Fletcher and Ousey (2010), Ousey et al. (2016), and Watret (2005) of practice, education, and industry, because it offers a potentially pragmatic solution to the current deficit in wound care education delivery and a model for the future.
Enactment Impotence and Author Accountability
Policy producers have no mandate to legislate for wound care policy enactment and can also avoid accountability through anonymity. The upshot of this impotence is a dilution of current efforts to standardize the wound care education curriculum. Policy content is often instead reduced to mere suggestion and recommendation and is thus nonprescriptive and subject to local interpretation, meaning that the existing structure of inequity and ambiguity is perpetuated.
Marketization of Wound Care Education
The growing “consumption” of wound care education as a good or service is apparent. Collectively referred to as commodities, consumption is a key aspect of modern capitalism, consistent with Fairclough’s (1989) conditions relating to the rise of consumerism and including economic conditions such as the ability to produce large varieties of commodity in large quantities and technological conditions, as demonstrated, for example, in the plentiful availability of Policy 2 to wound care nurses across the United Kingdom. Advertising discourses are also essential to consumerism, and these are apparent in the flyleaf of Policy 2 in the form of the company logos belonging to the main and lesser associated investors, pervading the context of education. For example, the charitable organization, the Wound Care Alliance UK, is also supported by URGO Medical, the main funding sponsor. While the creep of such capitalism, the system of economics that emphasizes private ownership, might currently be regarded skeptically in nurse education as a whole, capitalism represents free markets, choice, competition, and entrepreneurship to the wound care education market and could promote economic growth and freedom, as described by John Maynard Keynes (Keynes et al., 1971) and Adam Smith (Smith, 1987). However, it should be borne in mind that this can also serve to replace, create, maintain, or even exaggerate current inequalities in wound care education and practice.
Study Limitations
One limitation relates to the CDA only addressing UK professional body policy. Because wound care education policy is recognized as being a more widespread concern, it is recommended that future CDA encompasses additional European countries and the U.S. policy.
Conclusion
The aspects of wound care policy production and enactment revealed by the CDA are important to acknowledge due to the implications for nursing practice.
Without recognizing how individuals within organizations receive, adopt, and adapt evidence or organizational factors that constrain or facilitate adoption or implementation of policy and the interests and values at play within organizations influencing responses to policy issues, and if organizations choose not to adopt, adapt and act, policy will, as Greer et al. (2002) point out, remain idle. Disregarding the processes involved in policy issues, particularly implementation and interpretation, and the ways in which these can be part of what forms and reforms policy, fails to explore the whole picture surrounding policy. Furthermore, ignoring the interpretation component of the policy process, the whole picture remains unknown and “the values within policies can be critiqued, refined and even resisted” (Jones, 2013, p. 7). How policy is experienced by users themselves also remains undiscovered. The findings suggest that health service managers and wound care educationalists would benefit from becoming more familiar and involved with policy making processes and understanding their effect on education provision.
Wound care policy makers must now adopt an active (Bowen & Zwi, 2005), not passive, approach to policy making. An active position, compared with the inertia that appears to currently exist, would take into consideration the capacity to implement policy and not merely increase awareness or disseminate, as found in the CDA. As argued by Dodson et al. (2012), wound care policy making agencies need to make decisions on how to disseminate and implement policy. Active policy making would also adopt target audiences’ decisions to implement policy, instigate activities to improve knowledge and skills, facilitate change, and ensure continued use of policy as part of organizational operations.
Footnotes
Acknowledgments
The authors thank Professor Ian Rivers, Professor of Education for Social Change, University of Strathclyde, Glasgow and first supervisor of the EdD thesis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.