
Abstract
Introduction
Health literacy (HL), which is the ability to obtain, understand, and use health information to make informed decisions about one's health, is extremely important in the context of solid organ transplantation. 1 Throughout the transplant journey, patients must be able to utilize health information to navigate health systems, attend medical appointments, and maintain testing and diagnostic schedules, and other required services. Patients must comprehend, assess, communicate, and apply health information to make informed decisions about their care. Posttransplant care involves complex self-management tasks, including symptom monitoring, infection prevention, and maintaining a healthy lifestyle. Notably, the Centers for Disease Control and Prevention (CDC) has recently defined “organizational HL” as “the degree to which organizations equitably enable individuals to find, understand, and use information and services to inform health-related decisions and actions for themselves and others.” 2 This new definition emphasizes the need for people to use and apply health information rather than just understand it and acknowledges that organizations have a responsibility to address HL. 2
Adequate HL is essential for utilizing health information. Limited HL has been consistently associated with negative health outcomes both in the general population and in transplantation.3–8 Individuals who struggle to understand health information experience higher rates of hospitalization and increased use of emergency room services. They also have a higher risk of drug- and disease-related complications and difficulty engaging in disease-preventative strategies.4–6 In transplantation, lower HL has been associated with increased creatinine levels,7,8 more hospitalizations and readmissions,9,10 and an increased risk of graft failure. 10 People with poor HL are also less likely to be waitlisted for transplant.10,11 Unfortunately, limited HL is highly prevalent, affecting as many as 72% of patients with solid organ transplant. 3
Identifying people at risk of limited HL is challenging, and healthcare providers routinely overestimate their patients’ comprehension. 12 Demographic risk factors such as age, race/ethnicity, education level, and economic status are associated with limited HL, but relying exclusively on such characteristics can lead to incorrect assumptions. Several instruments have been developed to assess HL, 4 but the use of these instruments within a solid organ transplant context has yet to be explored. Previously published views have focused on instruments used in other disease states. Measuring HL has several potential applications. In a clinical setting, identifying specific patients at risk of limited HL could direct healthcare providers to provide additional support and tailor communication strategies accordingly. From a public health perspective, determining the HL at a population level could help inform promotion strategies. Measuring HL has been of utility in research, both as an outcome measure and as an important demographic variable.
Objective
Given this context, the purpose of this review is to address a critical gap in transplantation literature: while the impact of HL on outcomes is well recognized, there is limited awareness of the wide range of instruments available to measure HL and their varying characteristics. This scoping review summarizes how HL instruments have been applied in solid organ transplantation and provides a practical overview to guide clinicians and researchers in selecting appropriate measures for clinical and research settings.
Methods
Design
A scoping review was conducted to explore the existing literature on HL measurement in solid organ transplant recipients. The research question was framed using the PCC (population, concept, context) framework recommended for scoping reviews: population, solid organ transplant recipients (including pretransplant and posttransplant populations); concept, HL measurement instruments; context, any setting within transplantation (eg, clinical or research). A scoping review approach was chosen because the objective was to map the breadth and characteristics of existing literature on HL measurement in solid organ transplantation rather than to evaluate intervention effectiveness or synthesize outcomes. Scoping reviews are valuable for summarizing a wide range of literature, mapping available evidence, and identifying gaps in knowledge.
To identify the relevant literature for the review, a systematic search was conducted using 3 different databases: Medline, Embase, and CINAHL. The search strategy was developed and reviewed with a medical librarian to ensure completeness and accuracy. While the PRESS (Peer Review of Electronic Search Strategies) checklist was not explicitly documented, the review followed best practices consistent with PRESS principles. No supplementary search techniques (such as citation searching, manual review of key journals, or contacting experts) were performed beyond the database search. Terms related to the categories of HL, medical and medication literacy, and transplantation were used in the search. Boolean operators such as AND/OR were utilized to connect the categories. The search took place in August 2024. The comprehensive search strategies are provided in Appendix A.
Studies were eligible for inclusion if they were original articles published and written in English and measured HL in the context of solid organ transplant. The following articles were excluded: (1) case reports, book chapters, letters, editorials, abstracts; (2) studies that did not specify what instrument they used; (3) protocols that were later published with results available; (4) and studies that were not available in English. This scoping review was not prospectively registered.
Data Collection
Search results were compiled into Mendeley, and titles and abstracts duplicates were removed by VP. Full texts were retrieved for abstracts that passed the initial screening and were assessed for eligibility based on the inclusion and exclusion criteria by VP and BM. Any discrepancies between reviewers were resolved through discussion, and when consensus could not be reached, a third reviewer (HM) made the final decision.
The full breakdown of the article selection process is available in Figure 1. A data extraction tool was developed by VP and HM and was piloted with a sample of 5 articles. Refinements were made to the tools before proceeding with the full data extraction (performed by VP and BM and then reviewed by HM). Relevant data were captured in a data collection tool in Microsoft Excel (Version 16.9) and then summarized into tables. Once the transplant literature was identified, the screening tool was researched further, and original validation studies were reviewed. During data collection, articles were initially categorized according to the instrument name reported in each manuscript. After completion of data extraction, these categories were consolidated under their core instrument family to ensure consistency and avoid classification inconsistencies (eg, Brief Health Literacy Screen [BHLS], Subjective Health Literacy Screener [SHLS], and Short Literacy Survey [SLS] grouped).
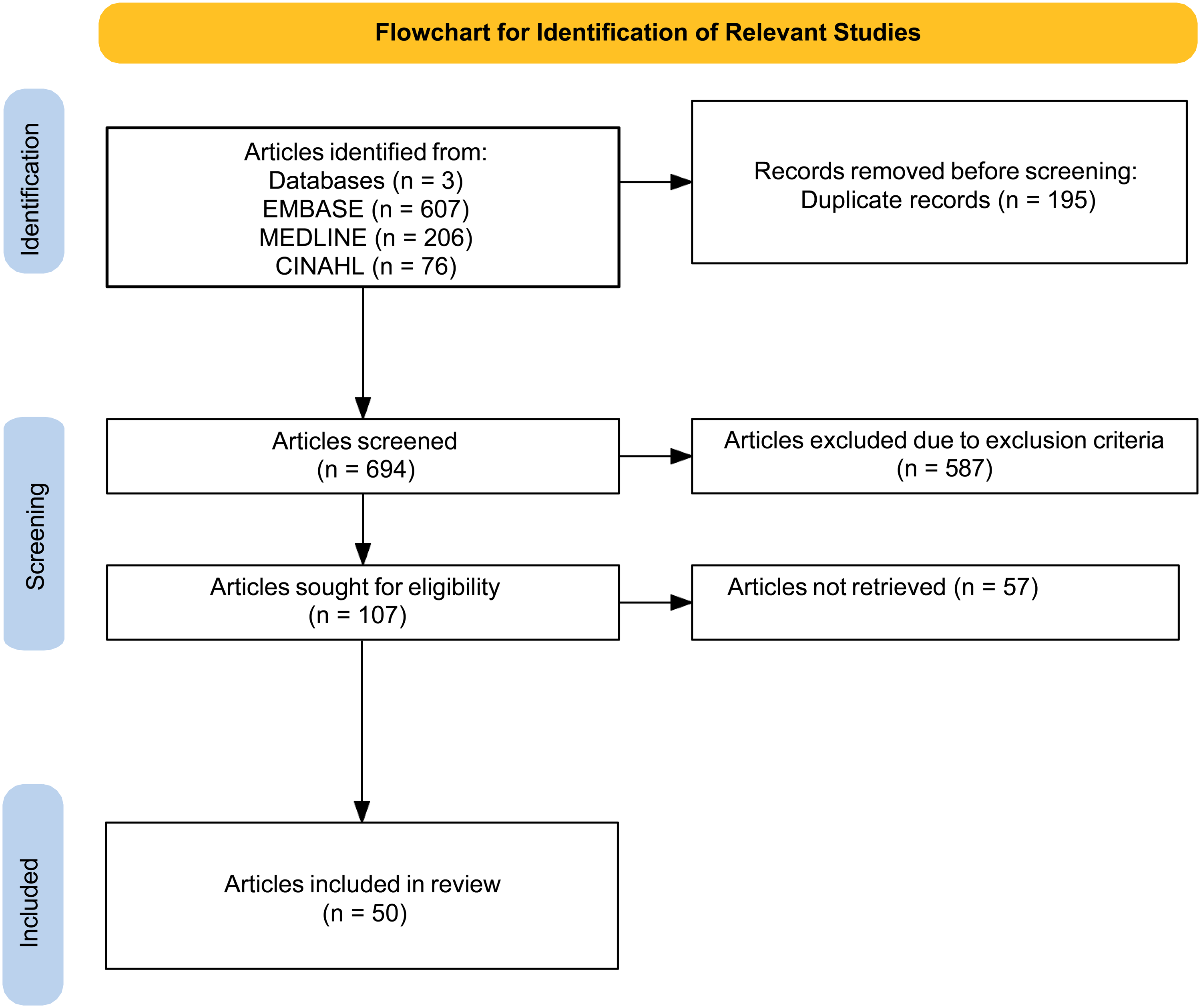
Flowchart for identification of relevant studies.
Outcome Measures
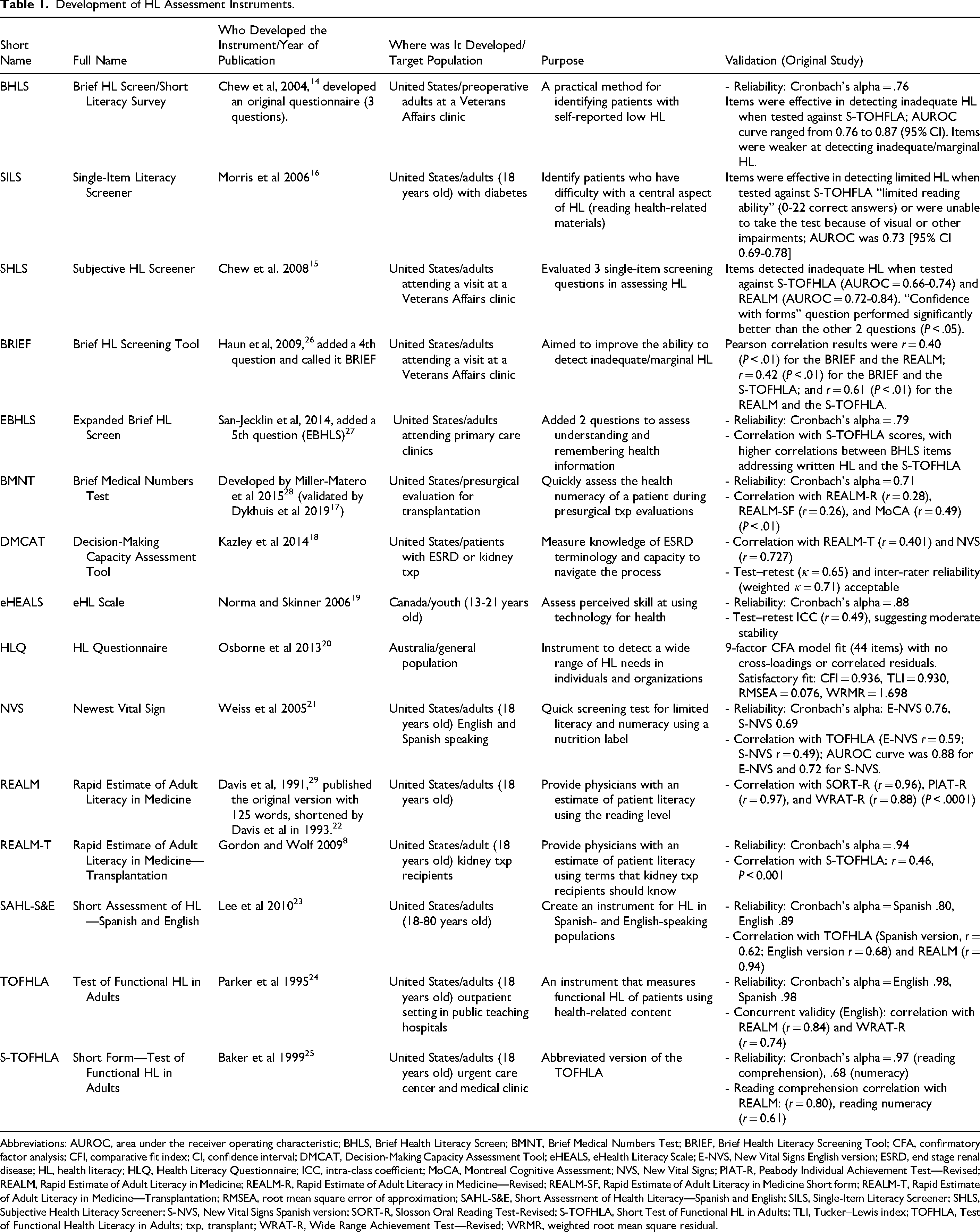
Extracted data included (1) publication details, including author and year; (2) study features, such as country, setting, population, participant count, and HL outcomes; and (3) HL instruments, including details regarding their name, dimensions, number of items, purpose, target audience, administration method, validation process, scoring system, cutoff points, and their strengths and limitations. Tables were compiled to provide a description of how and when the instruments were developed (Table 1), further describe the instruments’ characteristics (Table 2), review studies of the instruments used in transplants (Table 3), and provide a summary of the measures, including strengths and limitations for healthcare providers potentially considering their use in transplant (Table 4). Table 5 summarizes which HL instruments assess key domains such as numeracy, comprehension, digital HL, and functional HL, with the following definitions applied:
Development of HL Assessment Instruments.
Abbreviations: AUROC, area under the receiver operating characteristic; BHLS, Brief Health Literacy Screen; BMNT, Brief Medical Numbers Test; BRIEF, Brief Health Literacy Screening Tool; CFA, confirmatory factor analysis; CFI, comparative fit index; CI, confidence interval; DMCAT, Decision-Making Capacity Assessment Tool; eHEALS, eHealth Literacy Scale; E-NVS, New Vital Signs English version; ESRD, end stage renal disease; HL, health literacy; HLQ, Health Literacy Questionnaire; ICC, intra-class coefficient; MoCA, Montreal Cognitive Assessment; NVS, New Vital Signs; PIAT-R, Peabody Individual Achievement Test—Revised; REALM, Rapid Estimate of Adult Literacy in Medicine; REALM-R, Rapid Estimate of Adult Literacy in Medicine—Revised; REALM-SF, Rapid Estimate of Adult Literacy in Medicine Short form; REALM-T, Rapid Estimate of Adult Literacy in Medicine—Transplantation; RMSEA, root mean square error of approximation; SAHL-S&E, Short Assessment of Health Literacy—Spanish and English; SILS, Single-Item Literacy Screener; SHLS, Subjective Health Literacy Screener; S-NVS, New Vital Signs Spanish version; SORT-R, Slosson Oral Reading Test-Revised; S-TOFHLA, Short Test of Functional HL in Adults; TLI, Tucker–Lewis index; TOFHLA, Test of Functional Health Literacy in Adults; txp, transplant; WRAT-R, Wide Range Achievement Test—Revised; WRMR, weighted root mean square residual.
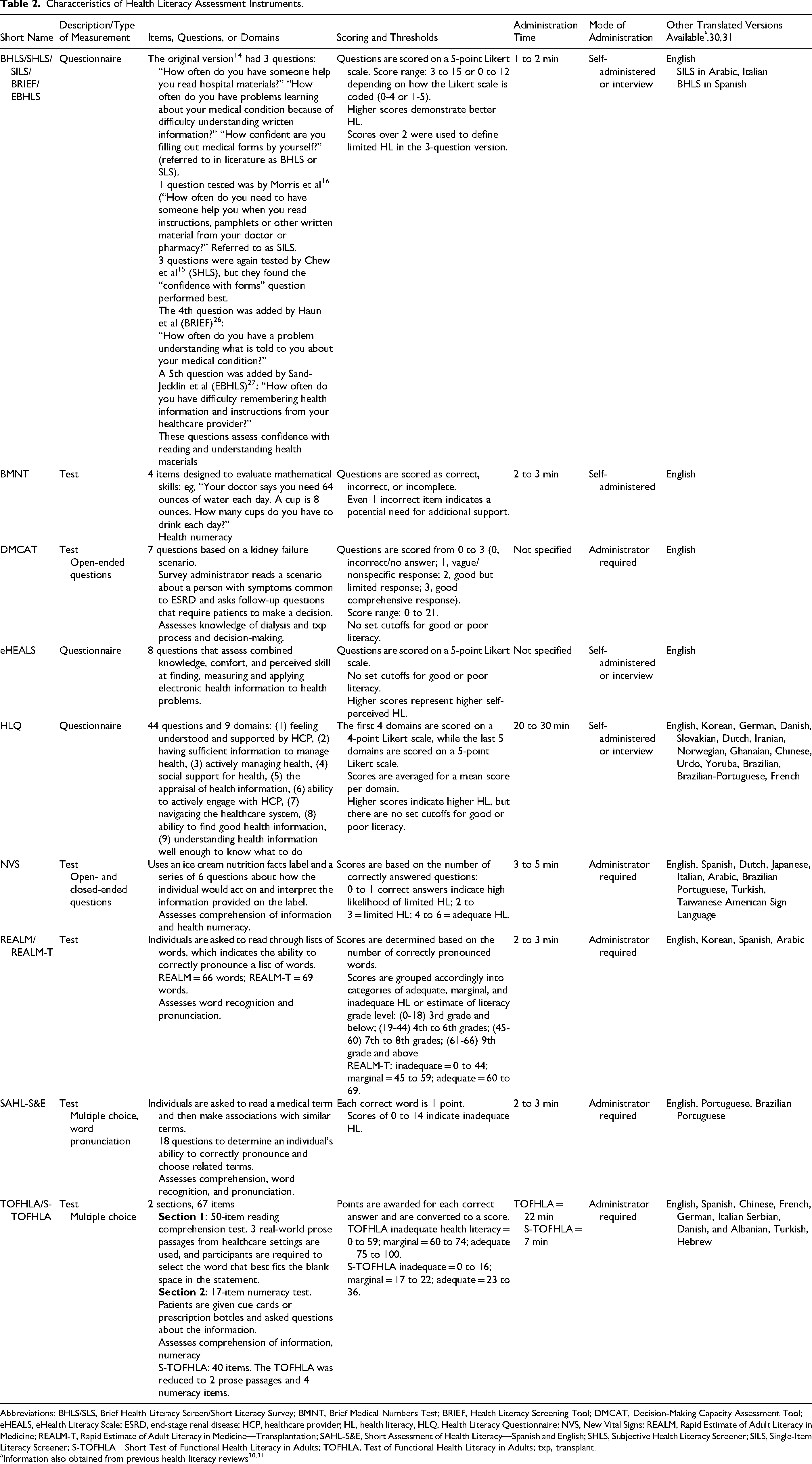
Characteristics of Health Literacy Assessment Instruments.
Abbreviations: BHLS/SLS, Brief Health Literacy Screen/Short Literacy Survey; BMNT, Brief Medical Numbers Test; BRIEF, Health Literacy Screening Tool; DMCAT, Decision-Making Capacity Assessment Tool; eHEALS, eHealth Literacy Scale; ESRD, end-stage renal disease; HCP, healthcare provider; HL, health literacy, HLQ, Health Literacy Questionnaire; NVS, New Vital Signs; REALM, Rapid Estimate of Adult Literacy in Medicine; REALM-T, Rapid Estimate of Adult Literacy in Medicine—Transplantation; SAHL-S&E, Short Assessment of Health Literacy—Spanish and English; SHLS, Subjective Health Literacy Screener; SILS, Single-Item Literacy Screener; S-TOFHLA = Short Test of Functional Health Literacy in Adults; TOFHLA, Test of Functional Health Literacy in Adults; txp, transplant.
Summary of Quantitative Health Literacy Assessment Studies in Organ Transplantation.

Abbreviations: aOR, adjusted odds ratio; aHR, adjusted hazard ratio; BHLS/SLS, Brief Health Literacy Screen/Short Literacy Survey; BMNT, Brief Medical Numbers Test; BRIGHT, Building Research Initiative Group: Chronic Illness Management and Adherence in Transplantation; CI, confidence interval; CKD, chronic kidney disease; DMCAT, Decision-Making Capacity Assessment Tool; eHEALS, eHealth Literacy Scale; EMR, electronic medical record; ESLD, end-stage liver disease; ESRD, end-stage renal disease; HL, health literacy; HLQ, Health Literacy Questionnaire; HR, hazard ratio; IRD, increased risk donors; K-TxEO, Korean version Transplant Effects Questionnaire; LVAD, left ventricular assist device; MoCA, Montreal Cognitive Assessment; MVA, multivariate analysis; NVS, New Vital Signs; RCT, randomized control study; REALM, Rapid Estimate of Adult Literacy in Medicine; REALM-SF, Rapid Estimate of Adult Literacy in Medicine-Short Form; REALM-T, Rapid Estimate of Adult Literacy in Medicine—Transplantation; SAHL-S&E, Short Assessment of Health Literacy—Spanish and English; SES, socioeconomic status; SHLS, Subjective Health Literacy Screener; SILS, Single-Item Literacy Screener; S-TOFHLA, Short Test of Functional Health Literacy in Adults; TxEQ, Transplant Effects Questionnaire—Adherence Subscale; TOFHLA, Test of Functional Health Literacy in Adults; txp, transplant.
Used REALM but did not include under it because the purpose was to validate BMNT.
Used REAM and NVS but did not include under it because the purpose was to validate DMCT.
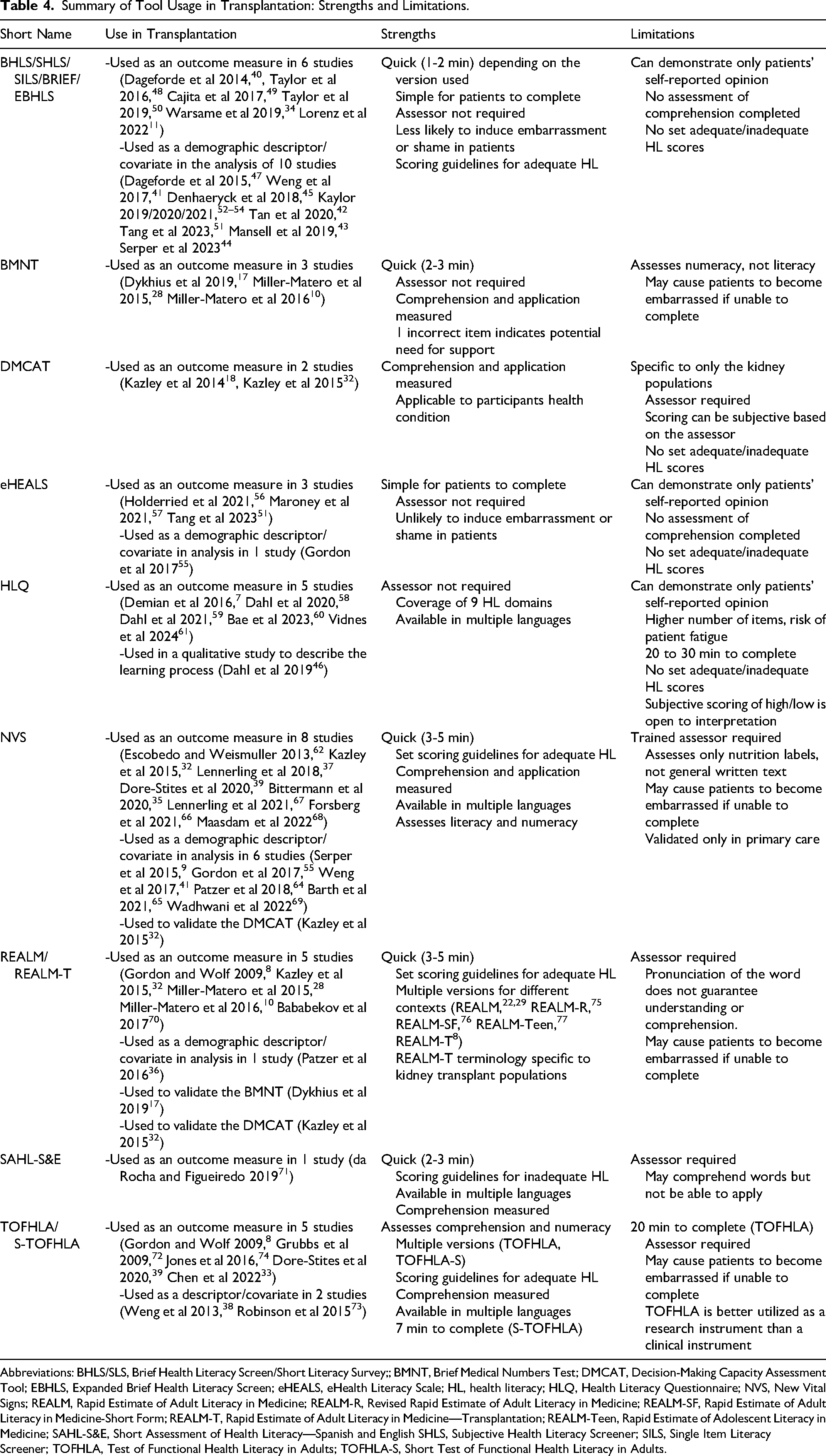
Summary of Tool Usage in Transplantation: Strengths and Limitations.
Abbreviations: BHLS/SLS, Brief Health Literacy Screen/Short Literacy Survey;; BMNT, Brief Medical Numbers Test; DMCAT, Decision-Making Capacity Assessment Tool; EBHLS, Expanded Brief Health Literacy Screen; eHEALS, eHealth Literacy Scale; HL, health literacy; HLQ, Health Literacy Questionnaire; NVS, New Vital Signs; REALM, Rapid Estimate of Adult Literacy in Medicine; REALM-R, Revised Rapid Estimate of Adult Literacy in Medicine; REALM-SF, Rapid Estimate of Adult Literacy in Medicine-Short Form; REALM-T, Rapid Estimate of Adult Literacy in Medicine—Transplantation; REALM-Teen, Rapid Estimate of Adolescent Literacy in Medicine; SAHL-S&E, Short Assessment of Health Literacy—Spanish and English SHLS, Subjective Health Literacy Screener; SILS, Single Item Literacy Screener; TOFHLA, Test of Functional Health Literacy in Adults; TOFHLA-S, Short Test of Functional Health Literacy in Adults.
Domains Assessed by Health Literacy Instruments.
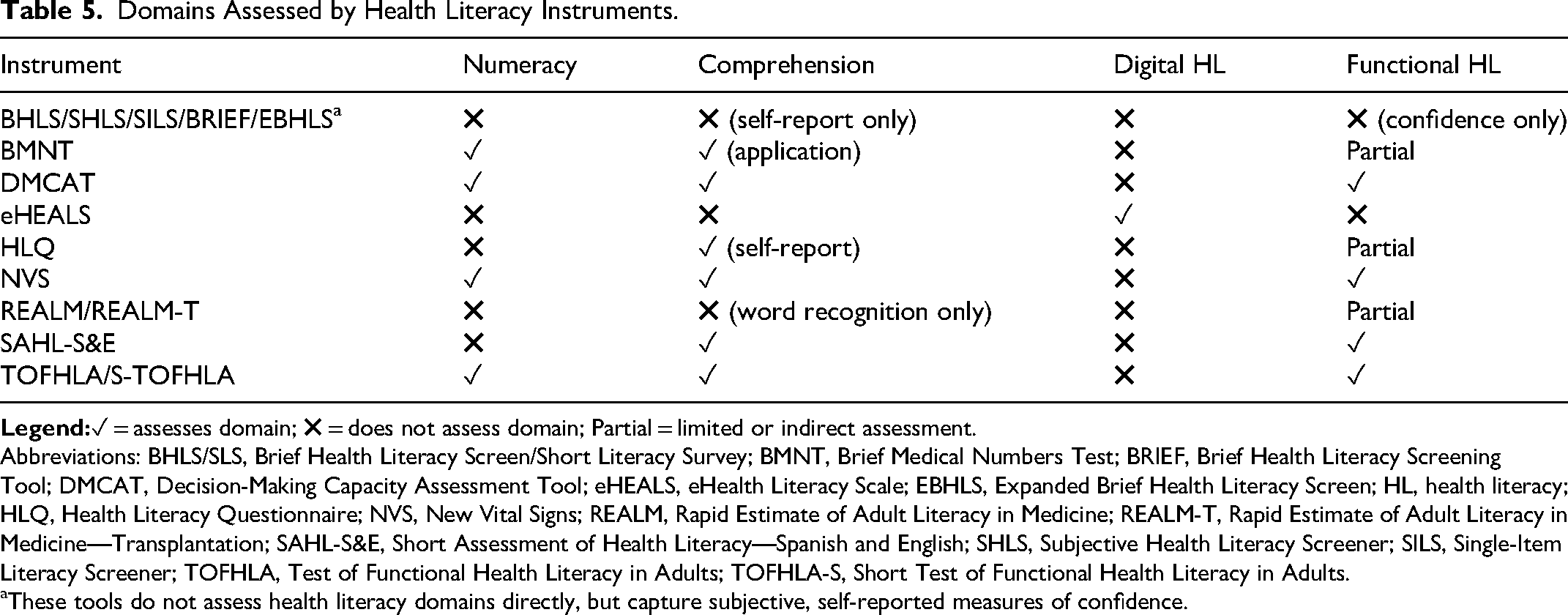
Abbreviations: BHLS/SLS, Brief Health Literacy Screen/Short Literacy Survey; BMNT, Brief Medical Numbers Test; BRIEF, Brief Health Literacy Screening Tool; DMCAT, Decision-Making Capacity Assessment Tool; eHEALS, eHealth Literacy Scale; EBHLS, Expanded Brief Health Literacy Screen; HL, health literacy; HLQ, Health Literacy Questionnaire; NVS, New Vital Signs; REALM, Rapid Estimate of Adult Literacy in Medicine; REALM-T, Rapid Estimate of Adult Literacy in Medicine—Transplantation; SAHL-S&E, Short Assessment of Health Literacy—Spanish and English; SHLS, Subjective Health Literacy Screener; SILS, Single-Item Literacy Screener; TOFHLA, Test of Functional Health Literacy in Adults; TOFHLA-S, Short Test of Functional Health Literacy in Adults.
These tools do not assess health literacy domains directly, but capture subjective, self-reported measures of confidence.
Results
The scoping review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P). 13 The PRISMA flowchart in Figure 1 shows the results of the search strategy. Overall, 721 articles were identified for title and abstract assessment, 94 articles were identified and further reviewed for full-text eligibility, and 50 were included in the review.
HL Instruments Identified
Multiple HL assessments have been used in the solid organ transplant population including the BHLS 14 or SHLS 15 and alternatives such as the Single-Item Literacy Screener (SILS), 16 the Brief Medical Numbers Test (BMNT), 17 the Decision-Making Capacity Assessment Tool (DMCAT), 18 the eHEALth Literacy Scale (eHEALS), 19 the HL Questionnaire (HLQ), 20 the Newest Vital Sign (NVS), 21 the Rapid Estimate of Adult Literacy in Medicine (REALM), 22 the Rapid Estimate of Adult Health Literacy in Medicine—Transplantation (REALM-T), 8 the Short Assessment of Health Literacy (SAHL), 23 the Test of Functional Health Literacy in Adults (TOFHLA), 24 and the Short Test of Functional Health Literacy in Adults (S-TOFHLA). 25 Most of the HL instruments were developed in the United States (n = 12) with intended use for adult patients (those >18 years of age). Only 1 HL instrument identified was developed in Canada and Australia. Most instruments had been validated in 1 or more studies by testing content and/or construct validity and/or reliability. Of note, only a few instruments were validated specifically within transplant populations, including REALM-T (developed for kidney transplant recipients), DMCAT (validated in end-stage renal disease [ESRD] and kidney transplant candidates), and BMNT (validated in transplant evaluation settings). All other instruments were originally validated in general populations and subsequently applied in transplant research without transplant-specific validation. Table 1 presents the development of the HL instruments, including who, when, and where the instrument was developed; an overview of the target population for which it was developed; and the original validation study.
Instrument Characteristics
A summary of the instrument characteristics is presented in Table 2. HL instruments were categorized as questionnaires or tests. Some instruments (BHLS/SHLS, SILS, eHEALS, and HLQ) used more subjective questionnaires, demonstrating patients’ self-reported opinions or confidence level. Other instruments (BMNT, DMCAT, NVS, REALM, SAHL, and TOFHLA) were characterized as tests (or performance measures), which provided objective assessment based on the number of correct or incorrect answers. Depending on the HL instrument, answers to the questionnaires or tests have been scored and assessed under different thresholds. Typically, a higher score indicates higher HL.
Four of the HL instruments identified can be self-administered. Other instruments, such as the DMCAT, NVS, REALM/REALM-T, SAHL-S&E, and TOFHLA/S-TOFHLA, require an administrator. Many HL instruments (n = 5) can be administered within 1 to 5 min. Conversely, the HLQ and TOFHLA take the longest to administer at 20 to 30 min and 22 min, respectively. The S-TOFHLA is a shortened version of the TOFHLA and can be completed in approximately 7 min.
Other instruments also had multiple versions, and their iterations are outlined in Table 2.
The development of HL screening instruments over time reflects a trend toward creating increasingly concise and targeted methods to identify patients with inadequate HL. Early measures like the BHLS/SLS 14 focused on general literacy challenges with three questions, while subsequent instruments, such as the SILS 16 condensed the assessment to a single question for simplicity and ease of use. Instruments like the Brief Health Literacy Screening Tool (BRIEF) 26 and Expanded Brief Health Literacy Screen (EBHLS) 27 continued to expand on earlier work by adding new questions to improve sensitivity and cover broader aspects of HL, such as understanding verbal information and recalling instructions. More specialized instruments, such as the BMNT 17 and DMCAT, 18 shifted focus to specific contexts like numeracy during transplantation evaluations and decision-making in chronic illness management. The eHEALS 19 and HLQ 20 instruments expand beyond basic literacy to assess skills such as using technology and identifying broader HL needs. The NVS 21 introduces numeracy as a critical component, using a practical task of interpreting a nutrition label. Similarly, the REALM family 22 focuses on estimating patient literacy levels using reading ability, with adaptations for specific populations, such as the REALM-T, 8 which is tailored for transplant recipients. The TOFHLA 24 and its shortened version, the S-TOFHLA, 25 are considered gold-standard assessments, combining both literacy and numeracy within a health-related context. Instruments like the SAHL-S&E 23 address the needs of bilingual populations by providing validated assessments in both Spanish and English. Additional instruments have also been translated into other languages, as described in Table 2.14–32 To facilitate quick comparisons for clinicians and researchers, Table 5 summarizes which HL instruments assess key domains such as numeracy, comprehension, digital HL, and functional HL.
HL in Measurement in Solid Organ Transplantation
The most common HL instruments used in transplantation were the BHLS (and iterations) with 16 studies, followed by NVS (15 studies), REALM (8 studies), TOFHLA (7 studies), and HLQ (6 studies). Most articles pertained to kidney transplant (n = 35), followed by liver (n = 4), heart (n = 3), and lung (n = 1) transplants. This imbalance underscores that the evidence base for HL measurement is most mature in kidney transplantation, while research in other organ groups remains limited.18–32 An additional 7 articles included multiple types of transplants, with 2 articles including hematopoietic/bone marrow transplant. Eighteen studies evaluated HL in pretransplant populations, and 24 studies evaluated posttransplant populations. An additional 8 studies included both pretransplant and posttransplant populations. While most studies exclusively involved patients (n = 47), 1 study also included kidney donors, and 2 studies included caregivers of transplant recipients.
As summarized in Table 3, most studies used HL as an outcome measure, with some investigating factors associated with low HL, such as being waitlisted or evaluated for transplantation, receiving a transplant, adhering to medication, and being rejected. Kazley et al 32 and Chen et al 33 found that patients with higher HL had an increased likelihood of being listed for transplant compared to those with lower HL. Limited HL was associated with increased risk of waitlist mortality and reduced likelihood of listing. 34 Lorenz et al 11 and Bittermann et al 35 found that patients with lower HL were less likely to be waitlisted. While Demian et al, 7 Patzer et al, 36 and Serper et al 9 found that lower HL was associated with medication nonadherence, Lennerling et al 37 found no correlation between HL and adherence. Weng et al 38 found no association between S-TOFHLA scores, specifically, and medication adherence, and Dore-Stites et al 39 found no association between adherence and TOFHLA. In other reports, HL was assessed but not used as an outcome measure. Rather, the authors used it to describe their population and/or treat HL as a covariate in the study analysis (eg, Weng et al, 41 and Tan et al 42 ).
The search strategy identified 2 published protocols,43,44 which were not included in Table 3 as they did not report any results. Two published articles were also excluded from Table 3 as follows. Denhaerynck et al 45 used the SHLS instrument, but it was not a significant factor in the study's analysis; Dahl et al used the HLQ to evaluate HL as part of the learning process in 10 qualitative interviews but did not relate HL to any transplantation outcomes. 46
Discussion
This review highlights the diversity of HL instruments used in transplant populations and underscores the absence of a universally optimal measure. Each HL instrument has distinct strengths and limitations. Questionnaires such as BHLS, eHEALS, HLQ, SHLS, and SILS rely on patient self-reported understanding or confidence in navigating health information. While easy to administer, self-reporting may overestimate or underestimate a person's actual HL skills. Conversely, assessments such as BMNT, DMCAT, NVS, REALM, SAHL, and TOFHLA are more objective, assessing functional skills like reading, numeracy, or word recognition. However, they may cause embarrassment for patients who struggle with elements of literacy. HL instruments also differ in the specific domains they assess. For example, some instruments focus narrowly on word recognition and pronunciation (e.g., REALM and SAHL), while others evaluate reading ability or print literacy (e.g., TOFHLA). Few instruments assess how one comprehends and utilizes health information in a real-world context. Furthermore, no instrument accounts for broader, important contextual factors such as system-level barriers or individual patient experiences with the healthcare system, which also impact HL.
Several instruments have multiple variations, which can complicate interpretation and comparison. For example, the REALM family includes REALM-SF (a 7-item short form for quick screening), REALM-R (with more complex words), and the REALM-T (tailored to transplant terminology). Both the REALM and REALM-T were identified in transplant literature (n = 6). Similarly, TOFHLA and its shortened version, S-TOFHLA, were commonly used. TOFHLA provides a comprehensive assessment of reading comprehension and numeracy using real healthcare materials, whereas S-TOFHLA offers a quicker alternative focused on reading comprehension. Short Likert-scale questionnaires such as SLS, BHLS/SHLS, BRIEF, SILS, and EBHLS share similar core questions, with BRIEF and EBHLS adding extra items. SLS and BHLS/SHLS are essentially the same instruments under different names. This overlap adds complexity when categorizing and comparing HL instruments.
Since no comprehensive measure exists, certain instruments may be more suitable in specific settings. For example, when HL is assessed as a primary outcome in research, instruments with detailed scoring systems (eg, TOFHLA) or those that offer assessment of multiple domains (eg, HLQ) may offer a more nuanced understanding. Where HL is assessed as a covariate, simpler instruments (eg, BHLS family) may be sufficient. In clinical settings, quicker instruments may be more practical. Instruments such as the BRIEF family or NVS take 1 to 5 min to complete and may be more practical compared to the TOFHLA or HLQ, which require 20 to 30 min. Furthermore, some instruments (eg, DMCAT, NVS, REALM, SAHL, and TOFHLA) require trained personnel for administration, which can complicate workflow. Of note, many of these instruments were validated or used in outpatient clinical settings. Application of these instruments in other settings may affect validity and results.
In the transplant setting, subjective tools (eg, BHLS, SILS, and HLQ) are well-suited for initial screening during routine clinic visits because they are brief, self-administered, and impose minimal burden on patients and staff. In contrast, objective tools (eg, TOFHLA, NVS, and REALM) provide a more comprehensive assessment of functional literacy and numeracy and may be preferable during pretransplant evaluations, where understanding complex instructions and medication regimens is critical for eligibility and long-term success. For long-term follow-up, subjective tools may again be practical for monitoring changes in perceived confidence and identifying emerging challenges, while objective tools could be reserved for cases where adherence issues or complications suggest a need for deeper assessment. Ultimately, combining both approaches in high-risk patients may offer the most robust strategy for tailoring interventions. Among the transplant studies we identified, associations between HL and outcomes such as adherence were inconsistent. Some studies linked low HL to nonadherence, while others found no correlation. These discrepancies likely stem from methodological differences, population heterogeneity and instrument focus, underscoring potential limitations with HL measurement and the need for standardized measurement approaches in transplant research.
HL is deeply intertwined with cultural, linguistic, and socioeconomic factors, yet most instruments identified were developed and validated in English-speaking populations, primarily in the United States. While some tools, such as SAHL-S&E, provide validated versions in Spanish and English, few offer multilingual adaptations or account for cultural nuances. Similarly, most tools assume a baseline level of formal education and cognitive function, which may limit applicability for patients with low literacy, limited schooling, or cognitive impairment. These validation gaps can result in misclassification of HL in minority populations, leading to inequitable support, poorly tailored health interventions, and the reinforcement of existing health disparities. These gaps highlight the need for instruments that are culturally sensitive, linguistically adaptable, and inclusive of diverse patient populations to ensure equitable assessment and care.
This systematic review has several limitations. First, the search strategy specifically included the term “health literacy,” which means studies that failed to explicitly mention HL in the title or abstract may have been missed. Additionally, the review focused on instruments that directly measure HL; instruments that primarily evaluate health-related knowledge or disease-specific understanding were excluded. While the original validation studies for each HL instrument were analyzed, secondary validation studies that may have assessed the instruments in additional populations or settings were not included. Furthermore, several studies used the instruments primarily as descriptive covariates rather than as main outcomes, which may reduce interpretive depth regarding their impact on clinical endpoints. Generalizability may be limited since the review relies heavily on instruments developed in the United States, and cultural and linguistic differences can impact HL. Furthermore, all studies were in English. The studies also differed in quality and sample sizes, and many were focused on kidney transplant populations.
Identified instruments assess individual HL, whereas organizational HL, as emphasized by Healthy People 2030, 2 is increasingly recognized as critical for equitable care. This distinction is important because organizational factors can significantly impact patient comprehension and engagement. Finally, although scoping reviews do not typically assess publication bias formally, it is possible that studies reporting significant associations between HL and outcomes were more likely to be published, introducing potential bias that should be acknowledged.
Conclusion
As HL becomes an increasingly important focus in health-based research, the number of instruments for measuring HL continues to grow. However, no single instrument offers a comprehensive measure of HL. This review highlights the HL instruments used in transplant populations, outlines their strengths and limitations, and guides healthcare providers and researchers seeking to integrate HL assessment into clinical practice or research. To enhance practical utility, we suggest recommendations for selecting instruments based on context:
For rapid clinical screening or research contexts where HL is a covariate, brief tools such as the BHLS, SILS, and NVS are ideal for quick administration. For research-focused assessments, where HL is the primary outcome, comprehensive instruments like the TOFHLA, S-TOFHLA, and HLQ provide detailed insights into multiple domains. In digital health contexts, the eHEALS was specifically designed to assess patients’ ability to navigate and use digital health resources. In caregiver-centered or broader contexts, instruments such as the HLQ allow for multidimensional assessment and can be adapted for caregiver involvement or proxy reporting.
By integrating HL assessment into transplant care and research, healthcare teams can better identify patients at risk, tailor communication strategies, and ultimately improve outcomes across the transplant trajectory.
Supplemental Material
sj-docx-1-pit-10.1177_15269248261432238 - Supplemental material for A Scoping Review and Practical Approach to Measuring Health Literacy in Solid Organ Transplantation
Supplemental material, sj-docx-1-pit-10.1177_15269248261432238 for A Scoping Review and Practical Approach to Measuring Health Literacy in Solid Organ Transplantation by Vanessa Phommavong, Breanna Morrison, Nicola Rosaasen, Kathryn Haubrich, Irène Pandraud-Riguet and Holly Mansell in Progress in Transplantation
Footnotes
Acknowledgements
The authors would like to thank Heather Tornblom, the medical librarian, for assistance with the search strategy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Kidney Foundation of Canada.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.