
Abstract
Introduction
Cognitive impairment in liver transplant recipients can lead to poor health outcomes, and identifying at-risk individuals is important to provide timely support. Poor social conditions, including poor socioeconomic status and lack of social support, have been suggested as potential contributors to cognitive impairment. Further, individuals with poor social conditions may experience psychological symptoms, such as depression and anxiety, which can further affect cognition.
Aim
This preliminary study explored longitudinal associations between social conditions, depression and anxiety symptoms, and cognition in liver transplant recipients.
Design
A total of 23 adult liver transplant candidates were enrolled, with 9 receiving liver transplantation, who were followed for up to 1-year post-transplant. Cognition was assessed using the Repeatable Battery for the Assessment of Neuropsychological Status. Social conditions and psychological symptoms were assessed through surveys. Linear mixed-effects models adjusted for age and education were used to examine the relationships between social conditions, psychological symptoms, and cognition. Moderation analysis was also conducted to explore interactions between social conditions and psychological symptoms.
Results
Cognitive scores remained stable over time. Social conditions were not associated with cognition, whereas higher levels of depression and anxiety symptoms were associated with worse cognitive performance. No significant interaction was found between social conditions and psychological symptoms on cognition.
Conclusion
Depression and anxiety symptoms, but not social conditions, showed associations with cognition in liver transplant recipients. These findings suggest the importance of assessing psychological symptoms in this population to identify those at risk for cognitive impairment.
Introduction
Cognitive impairment is a common yet understudied problem among liver transplant recipients. This condition affects up to 36% of liver transplant recipients, depending on the assessment measures and cutoffs used. 1 Cognitive impairment is associated with adverse health outcomes, such as a decline in graft function 2 and reduced health-related quality of life. 3 These findings underscore the importance of early identification of at-risk individuals to support timely management.
Existing literature has primarily focused on clinical predictors of post-transplant cognitive impairment, highlighting potential effects of pre-transplant hepatic encephalopathy, neurovascular and metabolic comorbidities, and immunosuppressant treatment.4,5 However, few studies have examined the influence of non-clinical factors. In the general population, social conditions, including socioeconomic status, social support, and isolation, have been consistently associated with cognition. For example, higher education, active social participation, lower perceived loneliness, and stronger social support are linked to better cognitive performance 6 and delayed progression to cognitive impairment. 7 Conversely, the accumulation of adverse social conditions is associated with greater cognitive decline. 8
Moreover, adverse social conditions are known to elevate psychological distress, including depression and anxiety. 9 In liver transplant recipients, these psychological concerns are prevalent, partly due to uncertainty about graft survival and the burden of long-term management. 10 Given that depression and anxiety are key contributors to cognitive impairment,11,12 individuals facing adverse social conditions and elevated psychological distress may be at greater risk for cognitive impairment. However, few studies have examined how social and psychological factors influence cognition in liver transplant recipients. Understanding their individual and interaction effects may help identify liver transplant recipients at higher risk for cognitive impairment and inform comprehensive care strategies, such as integrating family and peer support, facilitating access to community resources, and including screening and management of psychological distress. These approaches may help mitigate their impact on cognition and improve long-term outcomes in this population. This preliminary, longitudinal study explored associations between social conditions, depression and anxiety symptoms, and cognition from pre- to 12 months post-liver transplantation.
Methods
Design
This study used a longitudinal, single-center observational design. The Beth Israel Deaconess Medical Center institutional review board approved the study (2021P000902). Informed consent was obtained from each participant before being enrolled into the study.
Setting
This study was conducted at the Beth Israel Deaconess Medical Center transplant clinic, an urban transplant center.
Population
The demographic characteristics of the accessible patient population were similar to those of the US liver transplant population. Most patients at the center were White (78.2%), male (65.3%), and aged 50-64 years (44.6%), compared to 68.3%, 61.1%, and 44.8% in the national population, respectively. 13
Sampling
A convenience sampling was used to recruit liver transplant candidates at the Beth Israel Deaconess Medical Center transplant outpatient clinic between September 2022 and June 2023. The inclusion criteria for eligibility included: liver transplant candidates who were 18 years or older and fluent in written and spoken English. Patients were excluded if they were listed for dual-organ transplants and had previously received other organ transplants, such as a kidney. Patients with neurological conditions (eg, dementia and stroke), a history of head injury, or an inability to provide informed consent were excluded. A total of 112 liver transplant candidates were screened for eligibility, and 70 were eligible to participate. Among them, 54 were invited to participate, and 41 provided informed consent. Of those who consented, 12 later declined participation, and 6 became ineligible due to being listed for dual-organ transplantation or removal from the waiting list. The remaining 23 participants completed the baseline assessment.
Data Collection
Social Conditions
Social conditions were assessed using self-reported items, including marital status, living situation, annual household income, perceived income satisfaction, and social engagement (eg, how often do you participate in voluntary or charity work?). 14 In addition, perceived social support, social isolation, and satisfaction in social engagement were assessed using the items from the Patient-Reported Outcomes Measurement Information System (PROMIS) short forms: Instrumental, information, and emotional support 4a, Social isolation 4a, and Satisfaction with social roles and activities 4a. Annual household income was categorized as below $54,999 or $54,999 and above, approximating the 20th percentile based on the 2022 US census income data. 15 To comprehensively quantify an individual's social conditions, 16 the Social Vulnerability Index (SVI) approach, which was developed using a deficit accumulation model, 17 was used. PROMIS item responses were rescaled from their original Likert format to a 0-1 scale (eg, 0, 0.25, 0.5, 0.75, 1) for use in the SVI calculation, and other variables (eg, marital status, income) were also scored on a 0-1 scale as appropriate. The SVI was calculated as the sum of individual item scores. Higher SVI scores indicated greater social vulnerability. In addition to SVI scoring, PROMIS items were scored using their original Likert format to calculate raw and standardized T-scores (mean = 50, standard deviation [SD] = 10) to allow for comparison with the US general population. Higher T-scores indicate greater perceived social support, lower social isolation, and greater satisfaction with social roles and activities.
Psychological Symptoms
The PROMIS Depression Short Form 8b and Anxiety Short Form 8a assess the presence of depression and anxiety symptoms, respectively. Patients rated how frequently they experienced symptoms in the past 7 days from 1 (never) to 5 (always). Higher T-scores indicate more frequent depression or anxiety symptoms.
Cognition
The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) assesses global cognition with 12 items in five domains: attention, language, visuospatial/constructional abilities, and immediate and delayed memory. 18 Four alternate forms (A, B, C, and D) were utilized to reduce practice effects in the study. Higher raw scores indicate better global cognition. These scores can be converted to index scores, which are used to determine the level of cognition.
Demographics and Clinical Characteristics
Demographic data, such as race, ethnicity, and education level, were collected using a demographic questionnaire. Clinical characteristics, such as liver disease etiology, were collected through medical record review.
Procedure
All consented patients were scheduled to complete the pre-transplant baseline assessment. Those who received liver transplantation during the study period were scheduled to complete the follow-up assessment at 3-, 6-, and 12-months after liver transplantation, if available. All measures, excluding demographics, were repeated at baseline and follow-up assessments. Study visits were scheduled on the days of participants’ regular clinic visits to reduce participants’ burden.
Participants completed the surveys on social conditions, depression, anxiety, and demographics via Research Electronic Data Capture (REDCap).19,20 A hard copy of questionnaires was available for those who had difficulty completing the surveys online. Participants then completed the in-person, paper-and-pencil RBANS assessment in a private room. RBANS Form A was administered at baseline, and Forms B, C, and D were administered at the 3-, 6-, and 12-month assessments, respectively, after liver transplantation.
Data Analysis
Descriptive statistics were used to summarize baseline demographic and clinical characteristics. Continuous variables were reported as means and standard deviations, and categorical variables as frequencies and percentages. To examine changes in RBANS scores over time and their longitudinal relationship with SVI scores and PROMIS T-scores for depression and anxiety across four time points, linear mixed-effects models were performed, accounting for the within-subject correlation of repeated measures. Fixed effects included SVI, PROMIS T-scores for depression and anxiety, and timepoint, while adjusting for age, gender, race/ethnicity, education, and liver disease etiology. Only age and education were statistically significant and thus included in the final models. Random effects were specified for each participant to account for individual variability in baseline RBANS scores. Moderation analyses were conducted to assess interactions between SVI scores and PROMIS T-scores for depression and anxiety, respectively. Model assumptions were evaluated and adequately met. Normality of residuals was supported by Q-Q plots and the Shapiro-Wilk test. Residual versus fitted plots indicated no evidence of heteroscedasticity or nonlinearity. Variance inflation factors were less than 10, indicating no concerning multicollinearity. Standardized residuals and influence diagnostics indicated no influential observations affecting model estimates, and the distribution of random intercepts supported the assumption of normality. Given the small sample size, effect sizes including Cohen's dz and marginal and conditional R2 were calculated to estimate the magnitude of observed associations. Descriptive statistics were conducted using SPSS version 27 (IBM, Armonk, NY), and linear mixed-effect models were performed using SAS Studio version 3.81.
Results
Participant Characteristics
A total of 23 liver transplant candidates participated in the study. The overall mean age at baseline was 51.9 ± 13.1 years at baseline (Table 1). Most participants were male (78.3%) and non-Hispanic White (82.6%), with alcohol-related cirrhosis as the most common diagnosis (30.2%). The majority were married or in a partnership (52.2%), living with someone (78.3%), and satisfied with their income (56.5%). More than 80% of participants engaged in at least one social activity more than once a week. The PROMIS T-scores of social support, social isolation, and satisfaction with social roles and activities were either below or above average, indicating that participants perceived greater social support, were less socially isolated, and were more satisfied with their social roles and activities (Table 2).
Patient Baseline Characteristics (N = 23).
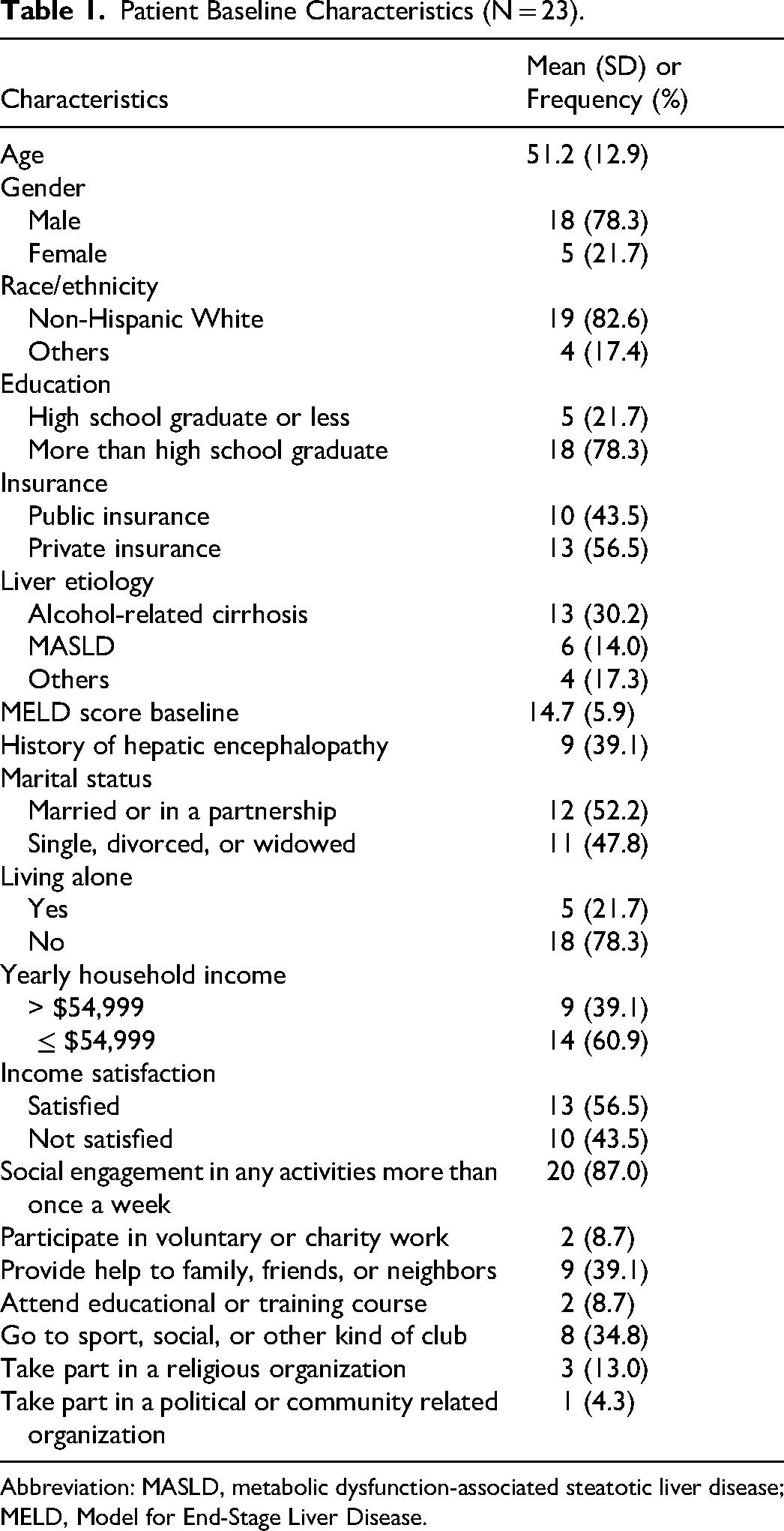
Abbreviation: MASLD, metabolic dysfunction-associated steatotic liver disease; MELD, Model for End-Stage Liver Disease.
Summary of SVI, Psychological Symptoms, and Cognition Scores Across Time Points.
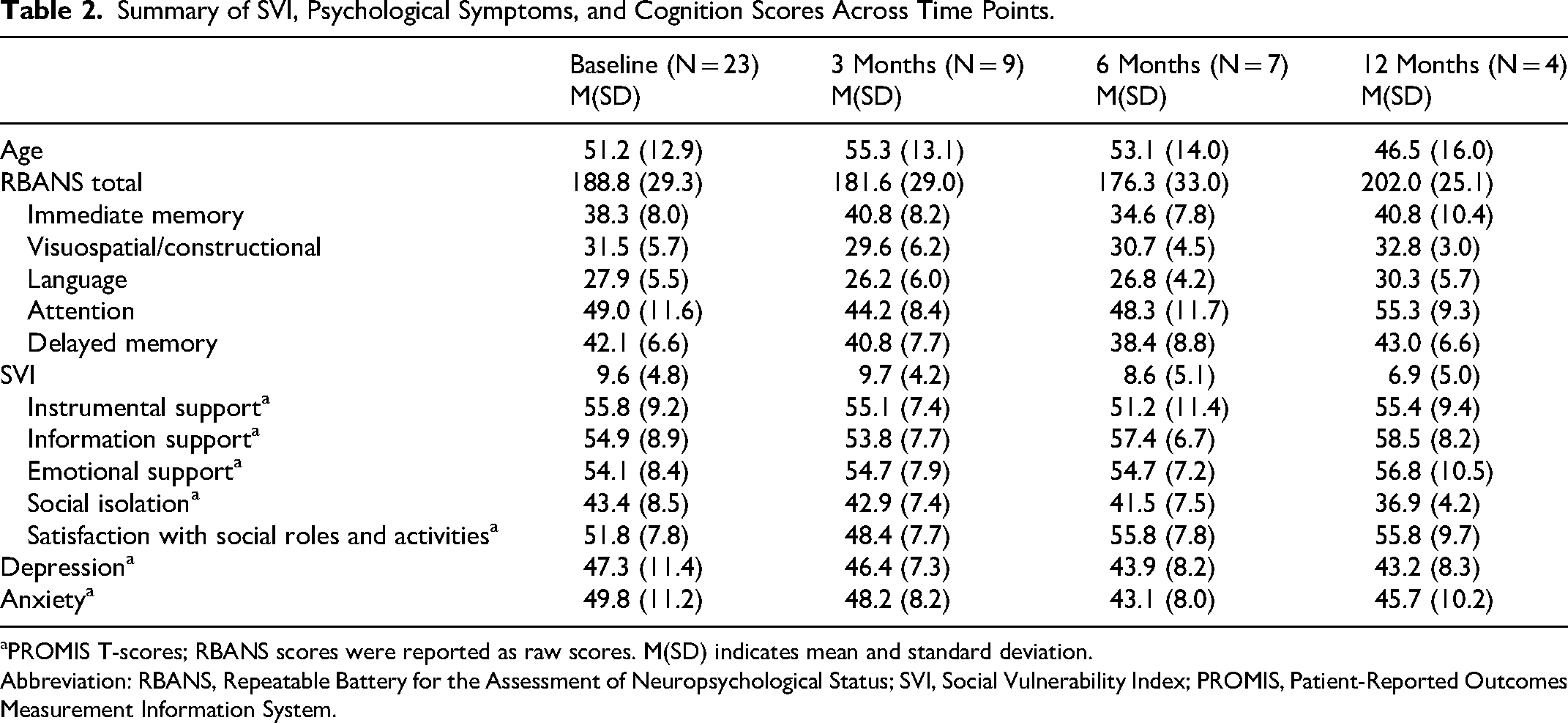
PROMIS T-scores; RBANS scores were reported as raw scores. M(SD) indicates mean and standard deviation.
Abbreviation: RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; SVI, Social Vulnerability Index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Cognition
The mean RBANS raw score at baseline was 188.8 ± 29.3 (Table 2), and the mean index score was 84.1 ± 11.9, indicating below average. A total of 14 (60.9%) scored below average.
A total of 9 participants received liver transplantation. The mean time from baseline to liver transplantation was 114.2 ± 118.6 days. All completed the 3-month post-transplant assessment, while 7 (77.8%) completed the 6-month assessment and 4 (44.4%) completed the 12-month assessment. While changes in RBANS scores over time were not statistically significant, Cohen's dz indicated that within-subject effect sizes were −0.47 at 3 months, 0.28 at 6 months, and −1.10 at 12 months. These values reflect a small improvement at 3 months, a small decline at 6 months, and a large improvement at 12 months relative to baseline scores.
Associations Between Social Factors, Psychological Factors, and Cognition
In the unadjusted models, SVI (β = –0.75, 95% Confidence Interval [CI]: −3.33, 1.83) and PROMIS depression (β = –0.06, 95% CI: −0.89, 0.78) were not associated with RBANS scores. Similarly, SVI (β = –1.04, 95% CI: −3.52, 1.44) and PROMIS anxiety (β = 0.15, 95% CI: −0.67, 0.97) showed no associations with RBANS scores (Table 3). In the adjusted models accounting for age and education, PROMIS depression (β = –1.20, 95% CI: −1.89, −0.52) was associated with RBANS scores, while SVI remained not associated (β = 0.00, 95% CI: −1.68, 1.69). Similarly, PROMIS anxiety (β = –0.92, 95% CI: −1.67, −0.17) was related to RBANS scores, while SVI showed no association (β = –0.43, 95% CI: −2.25, 1.38). The association between SVI and RBANS scores did not differ by PROMIS depression (β = 0.03, 95% CI: −0.10, 0.16) or PROMIS anxiety (β = 0.01, 95% CI: −0.11, 0.12), indicating that psychological symptoms did not moderate the relationship between social conditions and cognition. The adjusted model with interaction terms explained over 80% of the variance in RBANS scores, as indicated by the conditional R2 values (Table 3). Marginal R2 values indicated that the fixed effects, comprising SVI with either PROMIS depression or anxiety, explained 68%-73% of the variance in RBANS scores, demonstrating their meaningful contribution to the model.
Associations Between SVI, Psychological Symptoms, and Cognition.
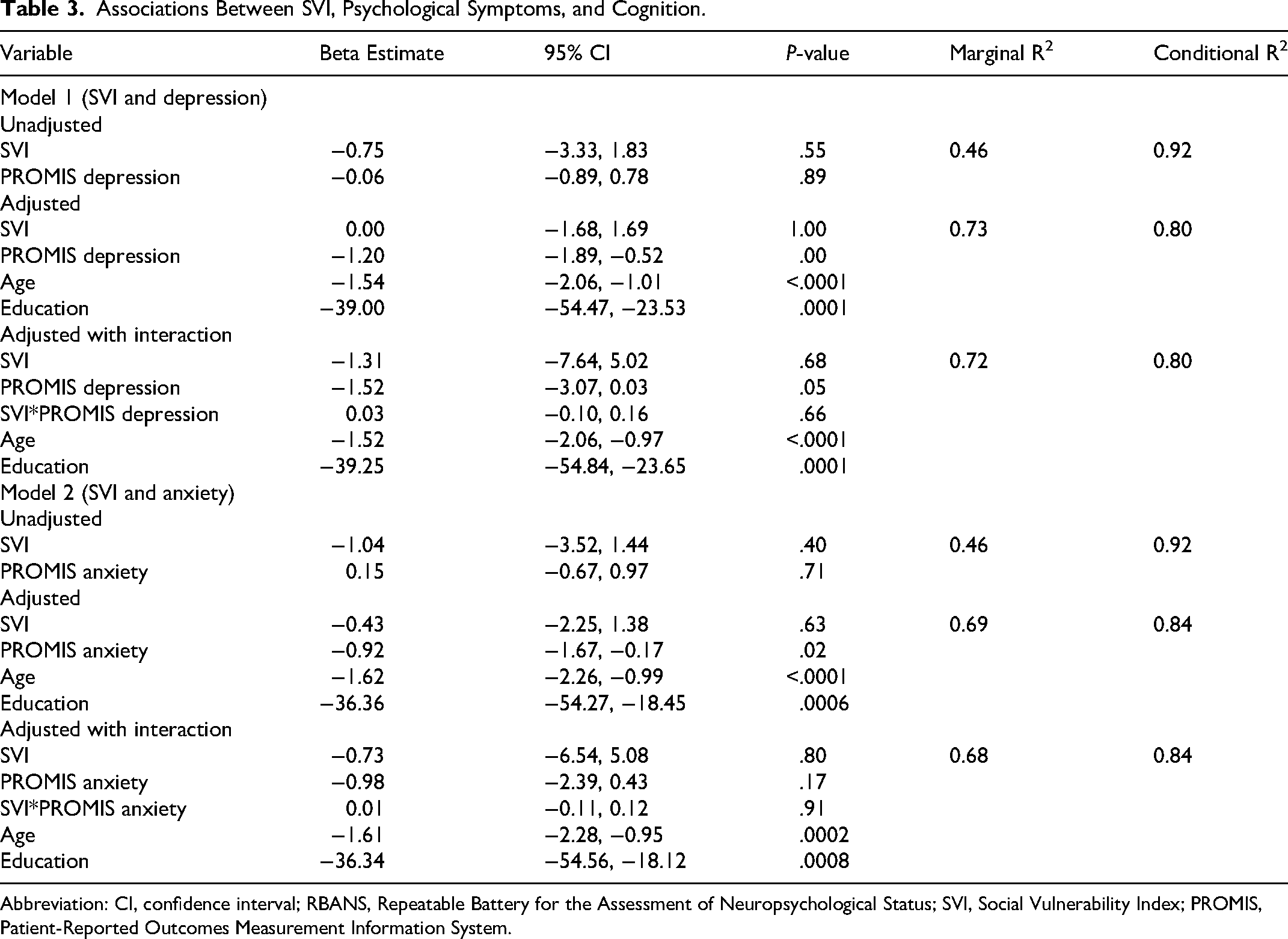
Abbreviation: CI, confidence interval; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status; SVI, Social Vulnerability Index; PROMIS, Patient-Reported Outcomes Measurement Information System.
Discussion
This preliminary, longitudinal study explored the associations between social conditions, depression and anxiety symptoms, and cognition from pre- to 12 months post-liver transplantation. More than 50% of participants showed below-average cognitive performance at baseline. Cognition was not significantly changed post-transplant. Social conditions were not associated with cognition after transplant, while higher depression and anxiety symptoms were associated with worse cognition. These findings suggest that psychological factors may play a critical role in cognition among liver transplant recipients.
Cognition remained relatively stable over the first year following liver transplantation in this study. Although a slight improvement was observed between the 6- and 12-month assessments, this may be partly attributable to differences in participant characteristics, such as increasing mean age at the 12-month follow-up. Given the small sample size, our findings may not fully capture the trajectory of post-transplant cognitive change. While limited evidence is available regarding cognitive trajectories after liver transplantation, existing studies suggest that cognition may remain stable, improve, or decline during the first-year post-transplant. Some recipients demonstrate improved cognition during the months following transplant,21–23 whereas others experience continued decline.22,24 Notably, recipients with cognitive impairment before transplant tend to have persistently lower cognitive scores even after transplantation. 22 Moreover, some individuals with normal cognition before transplant may experience a gradual decline during the first year after liver transplant. 21
This study found that depression and anxiety may be related to cognition after transplantation. After adjusting for age and education, higher levels of depression and anxiety symptoms were associated with lower cognitive performance. These findings are consistent with previous findings in general populations, which suggested depression and anxiety can contribute to cognitive decline.25,26 Depression and anxiety disrupt interconnected brain regions, including the prefrontal cortex and hippocampus, potentially leading to impaired cognition such as attention and executive functioning.27,28 However, given the repeated measures in this study, the direction of this relationship remains undetermined. Persistent cognitive impairment after transplantation may contribute to greater psychological distress, which may in turn affect cognitive performance. This interplay may complicate post-transplant recovery and daily functioning. While depression and anxiety are prevalent in liver transplant recipients, 10 there is limited research on their relationship with cognition in this population. Our findings highlight the need for further investigation to better understand this relationship and emphasize the importance of identifying and managing psychological symptoms in liver transplant recipients as part of post-transplant care.
This study found that social conditions were not associated with cognition among liver transplant recipients. While further investigation is needed to fully understand the relationship between the two in this population, one possible explanation is that the eligibility criteria for liver transplantation may have led to a sample with generally favorable social conditions. Specifically, candidates for liver transplantation often have higher social support and meet certain socioeconomic criteria, 29 which may have resulted in a study population with relatively high social conditions. Indeed, the data show that the mean T-scores for social conditions assessed by PROMIS were above average, indicating that participants generally had strong perceived social support, were satisfied with their social roles, and experienced low social isolation.
This limited variability in social conditions may also explain why social conditions did not moderate the relationship between psychological symptoms and cognition. This finding suggests that the relationships of depression and anxiety with cognition appeared consistent regardless of social conditions. Depression and anxiety are known to impair social functioning, leading to reduced social support, increased loneliness, and perceived social disability, which can further exacerbate psychological symptoms.30,31 Further, lower socioeconomic status is a known risk factor for depression and anxiety, which can in turn reduce productivity and negatively affect socioeconomic status. 32 Future studies with more socioeconomically diverse populations are needed to better understand the complex interplay of social conditions, psychological symptoms, and cognition in the liver transplant population.
While this study provides initial evidence on the relationship between social conditions and psychological symptoms with cognitive changes after liver transplant, there are a few limitations. Participants were enrolled at varying time points in their transplant journey, which may have introduced heterogeneity in baseline cognitive performance and influenced post-transplant cognition. Variations in the interval between baseline assessment and transplantation may have affected post-transplant cognition, potentially confounding the observed associations with social conditions and psychological factors. The small sample size limits the generalizability of the findings. Only a small number of participants received liver transplantation during the study period, resulting in limited post-transplant data and reducing the strength of longitudinal analyses. Since patients were recruited from a single transplant center with specific eligibility criteria, there is potential selection bias, which may restrict the applicability of the findings to broader populations. In addition, clinical outcomes such as graft function, which may influence post-transplant cognition, were not included in the analysis and could confound the observed relationships. Although no participants experienced graft failure during the study period, variations in graft function could influence cognition. Finally, although clinical factors, such as hepatic encephalopathy and Model for End-Stage Liver Disease score, have been associated with cognition in liver disease, these variables were excluded from the analysis as they were only relevant and available before transplant. Including them as static covariates in a longitudinal model could have introduced bias or misclassification, making it difficult to fully adjust for these potential confounders.
Conclusions
In conclusion, these preliminary findings suggest that depression and anxiety symptoms may play an important role in cognition among liver transplant recipients, whereas social conditions were not associated with cognition. These findings highlight the importance of considering psychological symptoms, along with clinical factors, in clinical practice to better identify patients at risk for cognitive impairment after liver transplantation. Future research involving larger and more diverse populations is needed to confirm these findings and inform the development of strategies to address cognitive impairment and improve overall health outcomes for liver transplant recipients.
Footnotes
Acknowledgements
The authors thank all study participants for their valuable contributions. Study data were collected and managed using REDCap electronic data capture tools hosted at Beth Israel Deaconess Medical Center.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Northeastern University, (grant number N/A).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB: Consultant for GSK and Intercept; Clinical trial funding from Chemomab, CymaBay, Gilead, Intercept, and Mirum; Serves as an editor for Clinical Liver Disease and DynaMed.