
Abstract

Keywords
The innovation and application of digital health interventions to support delivery of healthcare services is emerging at an unprecedented rate. This was particularly the case in midst of the COVID-19 pandemic, in which there was a need to minimize face-to-face interactions to prevent risks of contagion within the clinical setting. Whilst there are challenges associated with implementation of digital health interventions, potential benefits of these innovations have demonstrated to continue beyond minimizing the spread of infection with encouraging outcomes at both an individual patient and public health level.
Kidney transplantation presents as the best therapy option for many if not most individuals with advanced and progressive chronic kidney disease (CKD). Outside of the myriad of medical management modalities that may improve survival and quality of life outcomes in CKD, self-management interventions with a focus on improving physical activity and exercise behaviors has gained tremendous acknowledgement in recent years as a strategy to improve patient outcomes. 1 Prehabilitation is a recent concept that aims to optimize the patient's overall fitness before a major surgical procedure to promote recovery and outcomes overall. It revolves around implementing specific lifestyle changes and typically consists of physical exercise training programs, dietary management, and psychosocial interventions. 1 Prehabilitation is now gradually considered to be an essential part of the enhanced recovery pathway for those receiving kidney transplantation. 2
A recently published multi-center clinical trial from the UK by Greenwood and colleagues 3 concluded positive findings on evaluating the effects of a digital health intervention (Kidney BEAM) to enhance physical activity in people with CKD including transplant waitlist patients. In particular, the Kidney BEAM physical activity platform demonstrated to significantly improve mental health-related quality of life in patients with CKD. Teleprehabilitation has already been introduced in other surgical specialties during the COVID-19 pandemic, with encouraging results in terms of safety and patient experience. Franssen and colleagues 4 conducted a feasibility study for high-risk surgical patients (defined as those with oxygen uptake at the ventilatory anaerobic threshold ≤ 11 mL/kg/min or oxygen uptake at peak exercise ≤ 18 mL/kg/min) with colorectal cancer included in a home-based bimodal teleprehabilitation program. Results from their study garnered positive findings for the program in terms of its feasibility, measured by participation rate, dropout rate, adherence to the physical exercise training session's frequency, intensity, and time and retention rate. There was a high adherence rate towards the program's physical training requirements and at the end of it, most if not all patients were satisfied with their experience in the program according to responses from the patient appreciation questionnaire.
Building on these results, we suggest that kidney transplant centers and referring teams consider a virtual approach to prehabilitation in patients referred for transplantation and in those who are waitlisted ( Figure 1 ). The fact that these patients are often highly motivated and information technology-literate should help with such a strategy. Most waitlisted patients in developed countries own a smartphone. Further research focusing on feasibility, outcomes and cost-efficiency are needed to determine optimal teleprehabilitation strategies for this patient population.
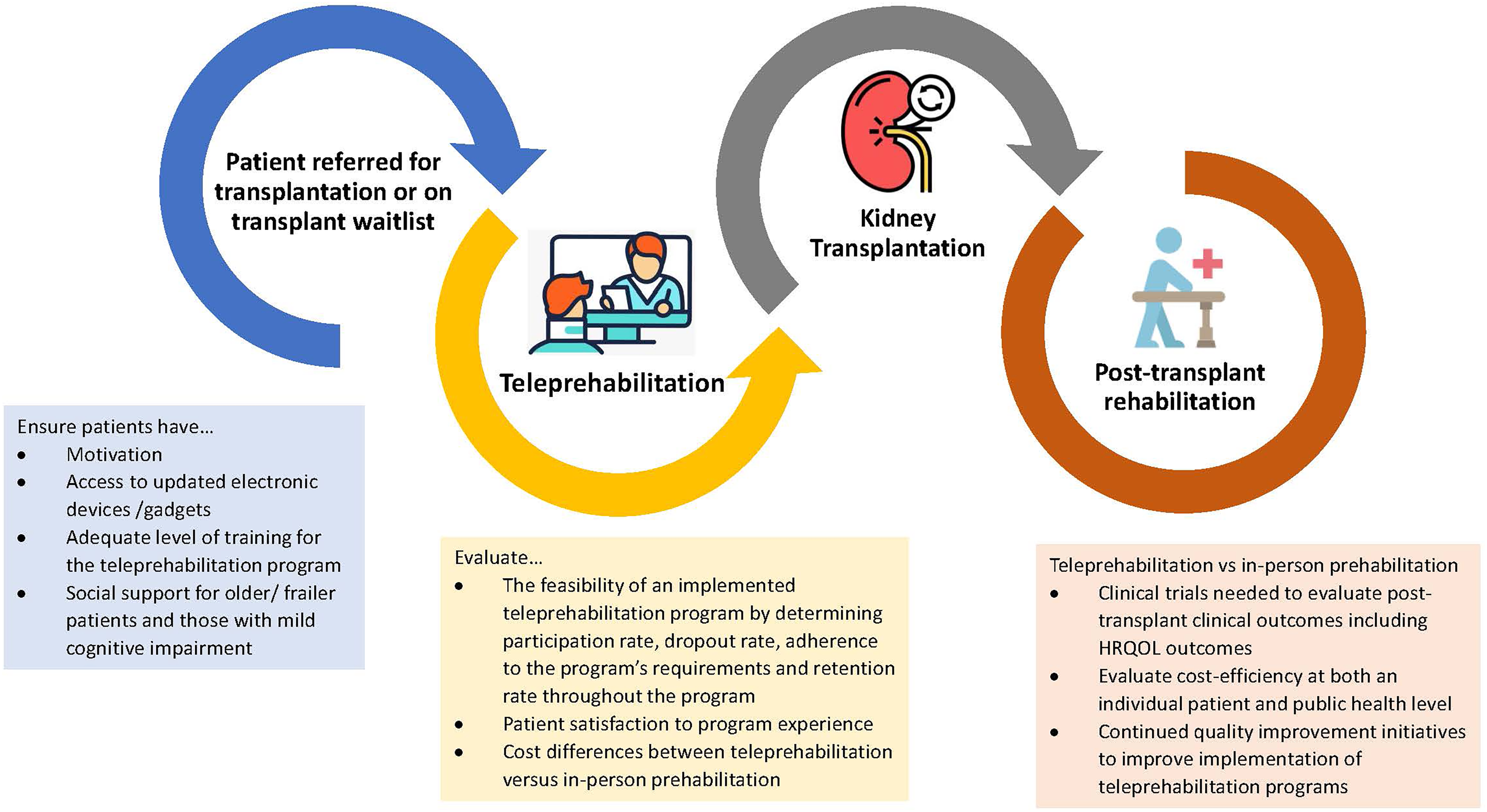
Proposed approach to teleprehabilitation in kidney transplantation health-related quality of life.