
Abstract
Introduction
Evaluation for lung transplantation involves comprehensive assessment of organ function, psychosocial health, and risk for latent infections and malignancy. 1 This process can be stressful for a patient with advanced organ disease. We describe a case of a lung transplant candidate who developed Takotsubo cardiomyopathy (TTC) also known as stress-induced cardiomyopathy, during the evaluation period. TTC is a syndrome of transient regional systolic dysfunction in the apex of the left ventricle without evidence of obstructive coronary artery disease or plaque rupture. The cause is largely not well understood but often follows an extremely stressful event. It is known to occur more frequently in post-menopausal women but is thought to account for 2% of all acute coronary syndromes. 2 The treatment is similar to that of other myocardial infarctions, and the impact on candidacy for transplantation is center specific. The purpose of this case report is to describe the broadening use of bronchoscopic lung valve reduction (BLVR) in providing symptomatic relief to a patient not eligible for transplant. Informed consent was obtained from the individual included in this case. Approval was obtained by the University of Alabama in Huntsville Institutional Review Board.
Presenting Concern
The patient, a 65-year-old female was former smoker (35 pack years) with advanced chronic obstructive pulmonary disease (COPD) (FEV1: 0.44L, 18% predicted), with hyperinflation (RV: 7.94L, 380% predicted), and low diffusing capacity (DLCO: 1.85 mL/min/mm Hg, 9% pred.). Given her limited expected survival and compromised quality of life, she was considered for lung transplantation. The extensive workup required 8 doctor office visits and multiple tests. During her inpatient evaluation week she was diagnosed with TTC, and became ineligible for transplant due to stress-induced cardiomyopathy. She was discharged home on aspirin, atorvastatin, and lisinopril to await potential recovery of heart function.
Clinical Findings
After 6 months of follow-up, the patient had symptomatic improvement, which correlated with normalization of heart structure and function on echocardiography. While she remained stable without further evidence of cardiomyopathy, she was considered for endobronchial valve implantation as compassionate therapy for improvement in symptoms and exercise tolerance.
The endobronchial valve implant is designed to occlude airflow in the target lung lobe thereby reducing lung volume. The device consists of a one-way silicone duckbill valve attached to a nickel-titanium (Nitinol) self-expanding retainer that is covered with a silicone membrane implanted in the target bronchus during a bronchoscopy procedure (
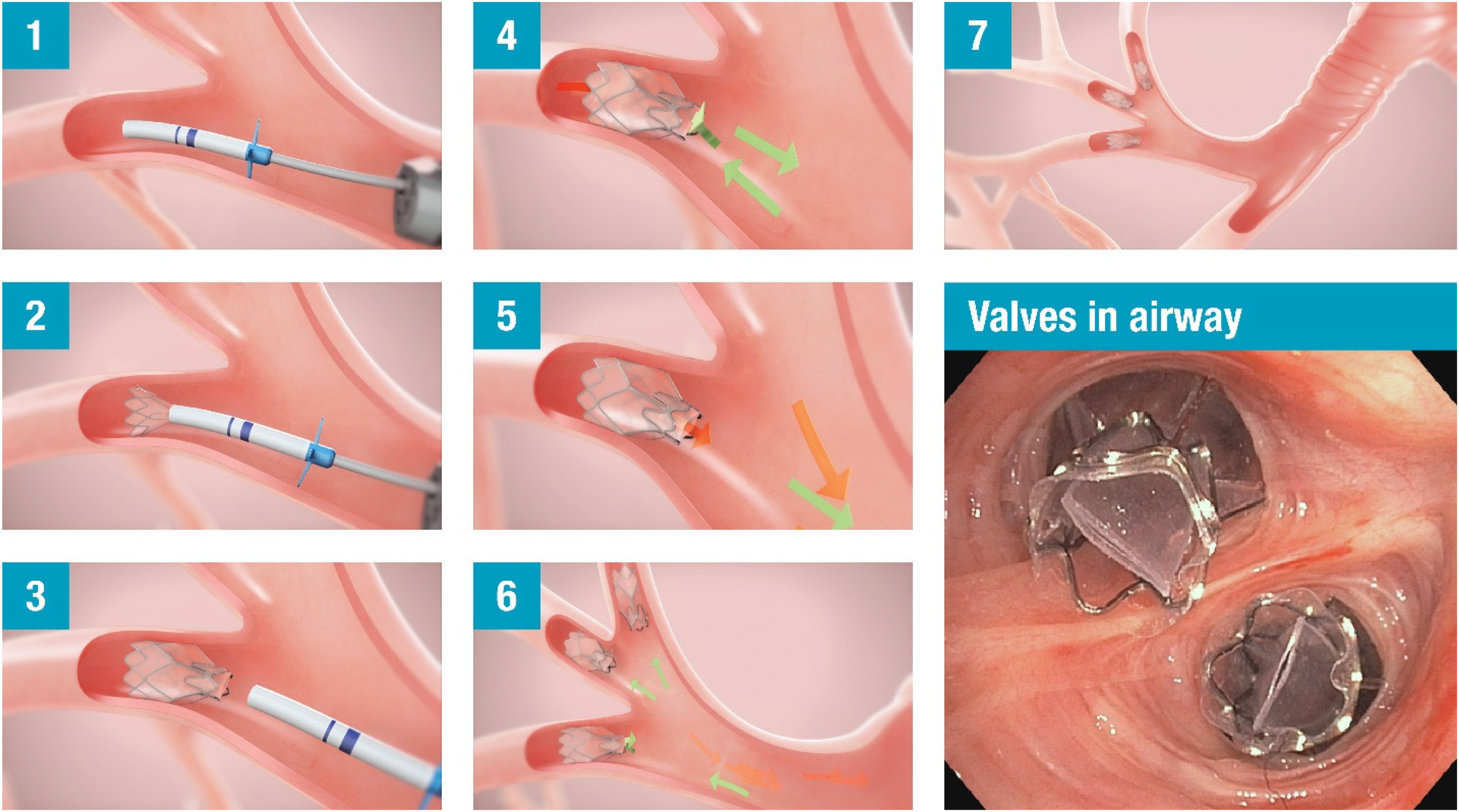
Bronchoscopic lung volume reduction procedure with endobronchial valves.
Endobronchial valve work-up identified her right upper lobe and right middle lobe combination as eligible target for valve implantation, and absence of collateral ventilation determined by Chartis® Pulmonary Assessment System (Pulmonx Corp., Redwood City, CA). She completed pulmonary rehabilitation and underwent BLVR with successful placement of 4 endobronchial valves in the right upper and middle lobes.
Outcome
She achieved lung volume reduction (TLVR of 51%), diminished lung hyperinflation and air trapping (RV: 4.73L, 224% predicted) with significant improvement in her carbon monoxide diffusing capacity (4.35 mL/min/mm Hg, 21% predicted) and daily functions. At her annual return visit, she maintained maximal medical therapy but decreased oxygen requirement. She was able to do household chores, walk to the mailbox without assistance, and stated she had “more energy than she has had in years” with improvement in her quality of life.
Discussion
Patients undergoing evaluation for lung transplantation are subject to a rigorous and stressful process. Furthermore, the strict criteria for lung allocation 4 often exclude patients with serious lung disease and extremely poor quality of life. It is therefore essential to take a proactive approach and expand alternative options for patients with advanced COPD not eligible for transplant and perhaps those waiting for lung transplantation. Increased awareness of BLVR as a treatment option is needed for both the medical professionals and the public.