
Abstract
Background / Significance of the Problem
Body fat and overall weight gain are common after kidney transplantation, and are known risk factors for poor clinical outcomes such as mortality. 1 Even in patients with normal pre-transplant weight, unmonitored weight gain can lead to overweight or obesity. 2 Therefore, early identification of patients with a high risk for post-transplantation weight or body fat gain is important, as it allows timely initiation of preventive interventions. To identify risk factors for weight/fat gain in the first year after kidney transplantation, an evidence-based approach was chosen.
Clinical Question
Our clinical question was “What variables influence body fat and overall weight gain during the first year after transplantation?” To ensure that causality could be inferred, only longitudinal studies were included.
Search of the Literature
Medline / Pubmed were searched in November 2018 that included longitudinal prospective and retrospective cohort studies that investigated risk factors for weight gain, body fat gain, or body mass index (BMI) outcomes. Our initial returns were updated in March 2022 using the following search strategy:
MeSH DESCRIPTOR Risk Factors MeSH DESCRIPTOR Kidney Transplantation MeSH DESCRIPTORs Body Mass Index OR Obesity OR Overweight OR Obesity, Morbid OR Weight Reduction Programs OR Ideal Body Weight OR Weight Loss OR Weight Gain OR Body Weight Changes OR Body Weight Maintenance OR Resistance Training OR Waist-Height Ratio OR Body WeightAnorexia OR Anorexia Nervosa Underweight 3 OR 4 1 AND 2 AND 5
The literature search yielded 533 articles, the reference lists of which led to 5 more, resulting in a total of 538 articles. Studies were excluded if any of the following criteria applied: No prospective or retrospective cohort design with body weight as outcome (N = 500); review or protocol for future study (N = 4); reporting inconsistencies (N = 1); no measurement at month twelve (N = 10); influencing variables not measured before month twelve (N = 3); not restricted to kidney transplantation (N = 1); or the operationalization of the outcome variable(s) does not allow the drawing of inferences regarding the influencing variable (N = 2); language of publication neither English nor German (N = 1).
Clinical Appraisal
Results of the Literature Review
Of the 538 studies returned by the search, 16 fulfilled the criteria for inclusion in the narrative review. Of those, only 1 focused on body fat gain 3 ; the other 15 explored risk factors for weight gain. All included studies were published between 2001 and 2020; the majority (N = 11) were conducted in the United States. Their common strength was their prospective (N = 11) or retrospective (N = 5) cohort design, which clarified the causality both of factors and of outcomes. Their most common limitation was a small sample size: 7worked with fewer than 100 transplant recipients.
The selected studies investigated a wide variety of risk factors on weight gain over the first years posttransplant. These included genetic, socio-demographic, behavioral, biomedical, psychological and environmental variables. The study results were synthesized narratively. Based on the evidence presented, the risk factors were divided into 5 groups:
Expert opinions
All factors, but especially those with controversial or weak evidence, were discussed with 2 clinical experts independently. Both experts had broad clinical and research expertise in weight gain and solid organ transplantation, held university degrees (PhD or MD) and had published in this field of research. Any variables that at least 1 expert associated with increased risk were counted as potential risk factors. Of the risk factors identified in the literature or those not previously identified as risk factors, the experts assessed only living donation differently from the published evidence: both saw a living donation as associated with better well-being; therefore, the experts recommended not to treat it as a risk factor.
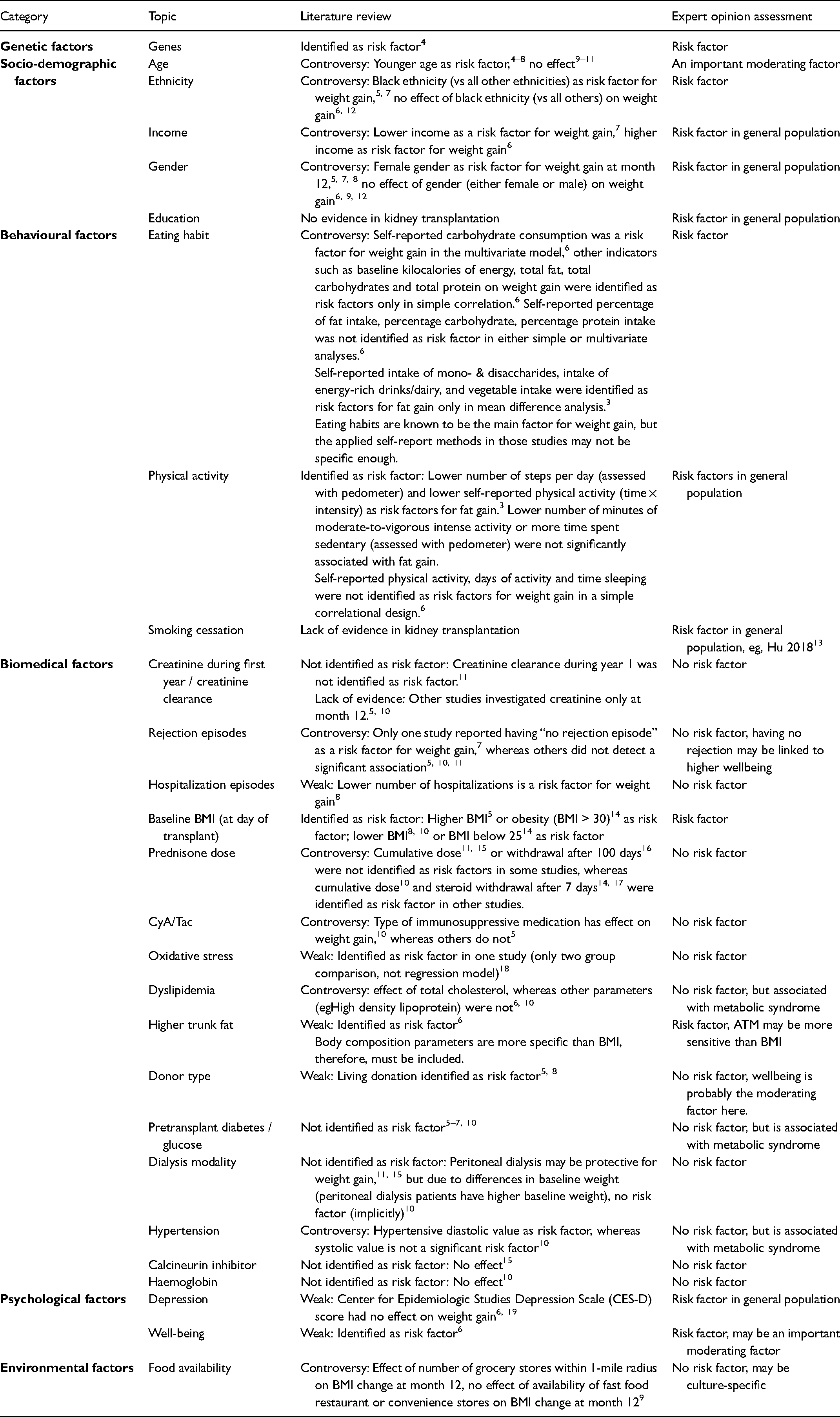
The results of the literature review and expert opinion are displayed in Table 1. Age, gender, genes, income, ethnicity, education, eating habits, physical activity, smoking cessation, baseline BMI, baseline body fat, depression and well-being were identified as potentially relevant factors for posttransplant weight and/or body fat gain.
Risk Factors for Increased Weight (Kg), BMI or Body Fat Percentage at 1-Year Posttransplant.
Integration into Practice
Based on the literature review and expert opinions, a number of potential risk factors have been identified. Before these can be integrated into clinical practice, further steps are necessary. One of these is to critically appraise each identified factor's suitability for clinical use. To do that, the
For example, while assessments of depression and well-being were administered as part of each prospective kidney recipient's assessment for registration to a graft waiting list, they may not be part of routine follow-up care. Implementing them would be resource-intensive, particularly if administered directly by a psychologist, and may not be well-received by all patients. And while the affordability, practicability, cost-effectiveness and acceptability may all be higher for a different type of operationalization and/or of measurement method, eg, self-reporting via questionnaire, those methods would also likely be less accurate. Consequently, in addition to the APEASE-criteria, each proposed assessment method's sensitivity and specificity must also be considered.
Similarly, while dual-energy x-ray (DEXA) scans are the gold standard method to measure body fat, their cost per use (including technician time) makes them unfeasible for frequent application. For routine clinical use or home monitoring, various simple, cost-effective and reasonably accurate methods of calculating body composition are available. Bioelectrical impedance analysis (BIA), for example, is very quick, inexpensive and acceptably precise, generally making it a more feasible option. 18
Evaluation of Evidence-Based Practice
To foster the uptake of routine assessment of risk factors for posttransplant weight and body fat gain in post-transplant care, changes in clinical practice should be tailored to the local setting. A careful analysis of that context (ie, values and beliefs, treatment guidelines, reimbursement policies) may help the interventionists engage stakeholders and decision makers from a very early stage. 19 The assessment of body trunk fat, physical activity, depression and well-being, and eating habits requires patient participation and may even involve considerable effort on their part; therefore, their acceptance and engagement are keys to enhancing their adoption of this intervention. As implementation outcomes, patients’ and health professionals’ acceptance and adoption of the risk assessment may also function as quality indicators for the evaluation of evidence-based practice.
Future Areas for Investigation
The aim of the literature review and expert opinion was to produce a selection of potential factors behind increases in overall weight (BMI) or body fat in the first year following kidney transplantation. It is not yet clear which of those identified have the strongest potential to predict weight gain. Therefore, the next major step will be to reduce the potential risk factors to the most relevant.
Footnotes
Acknowledgements
We thank Prof. Thomas Fehr and Dr Sonja Beckmann for contributing their view on variable selection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.