
Abstract
Introduction/Background
The pretransplant period is a vulnerable stage in the lung transplant journey. Patients and caregivers face the stressors of coping with a progressive illness, the loss of autonomy, and anxiety from waiting for an organ.1,2 Education is fundamental; patients must learn skills for navigating the healthcare system and the lifestyle changes required after the transplant. The pretransplant education process within our center currently involves a series of one-on-one consultations with the local transplant respirologist, and a trip to the transplanting center for education and pulmonary rehabilitation. During the Covid-19 pandemic many of these appointments have been performed virtually or by phone, rather than in person.
Recently, our interdisciplinary team collaborated with Lung Saskatchewan and patient stakeholders to develop a 6-part video series that describes the lung transplant process. The English videos, which were adapted from previous work3–5 according to best practice for education for patients pursuing transplants, 6 are intended to supplement the first education session provided by the transplant respirologist. This initial meeting includes basic information about the transplant process (eg, what a lung transplant is, the process involved, potential risks and benefits, and what the expectations are before and after the transplant). The session lasts between 30–90 min depending on the situation and is tailored to the patient's needs and understanding. The videos are 72 min in length, and feature an animated character and caregiver progressing through the transplant process interlaced with testimonials from patients and healthcare providers. The first two videos introduce the viewer to the series and to the impacts of lung disease; videos 3-6 describe the workup, waitlist, operation, recovery, posttransplant medications and required lifestyle changes. The videos are not intended to provide new information; rather they provide visual context and other patient's actual experiences to supplement a process that may seem abstract when described verbally by the physicians. Patients and caregivers were invited to watch the videos. Coinciding with the Covid-19 pandemic, the completion of this project provided an opportunity to pilot and evaluate the education delivered to patients electronically (rather showing the videos in a clinic setting). The objectives of this program evaluation were to 1) determine the patient satisfaction with this new electronic home-based education; 2) confirm the ideal time for the supplemental education; and 3) identify gaps in education and issues that remain.
Design/Methods
Design
This mixed-methods study was approved by the local Behavioural Ethics Board (Beh ID#2143). All participants provided informed consent prior to participation.
Setting
Telephone interviews were conducted with patients from a single center adult-only satellite program in Canada. Patients at this program receive the workup and follow-up care at the home institution. They must also travel out-of-province to the transplanting center for pretransplant pulmonary rehabilitation and the transplant surgery.
Population
All eligible pretransplant lung patients were identified by the study physicians. At the time of the study, the target population consisted of 63% men, the mean age was 61 years, and 77% identified as Caucasian and 17% Indigenous. The top two reasons for transplant referral were interstitial lung disease and Chronic Obstructive Pulmonary Disease (COPD) (46% and 42%, respectively).
Sampling
Criterion sampling was used, whereby all participants who met the criteria (being assessed or listed for lung transplant) were mailed an invitation. Patients who had previously received a lung transplant were excluded. The research associate followed up with the potential participant by phone at least one week later.
Data Collection
Interviews were conducted by a third-party qualitative research associate from the Canadian Hub for Applied and Social Research (CHASR) by telephone using a semi-structured interview guide (drafted a priori by the team, which included patient input). (See Supplemental material) As a quantitative measure, participants were asked to rate statements pertaining to the educational value of the videos on a Likert scale of 1 = lowest to 5 = highest. The qualitative questions explored two unrelated topics: a) those pertaining to this video appraisal (program evaluation) and b) the experience of Covid-19. These analyses were conducted separately. The program evaluation results are described in this manuscript.
Demographic data including residence, diagnosis, stage of process, age, gender, marital status, education, and ethnicity were collected. The interviews were audio-recorded, and field notes were taken to aid in interpretation of the data. Participants were invited to review the transcripts and were provided with a $25 gift card after the interview.
Data Analysis
Quantitative results were reported descriptively. Qualitative inquiry used the principles of phenomenological inquiry 7 to learn about the direct experiences of patients and was analyzed using the techniques of Braun & Clarke 8 with NVivo 12 Pro (QSR International, 2021). Data were collected and analyzed by the third-party research associate.
Broad-based categorization was first applied to establish collections of data pieces (initial codes to digitally flag that which was deemed meaningful to the research questions) that could be further interrogated and determined as substantively connected or not. A secondary review consisted of scanning and locating poignant quotes driving the conversation applicable to the research question(s). Final coding involved taking the initial broad categories and reorganizing, splitting or submerging themes or sub-themes and placing data instances in their most appropriate categories. 9 The aim was to remain inductively close to the data and the constructed and social meanings that cultivate from individual experiences. 7
Procedure
The video series were hosted on the internet. Patients were mailed access to the password-protected videos and the qualitative research associate followed up to confirm interest and schedule a mutually convenient time for the interview after the videos were viewed in their entirety.
Results
Of 48 people approached, 22 participants interviewed for this project, 17 participants and 3 caregivers (spouses) watched the entire video series and are included in this manuscript. Being too busy or misplacing the video links were the most common reasons for not viewing the videos. The interviews lasted between 10–60 min (mean 35) and occurred between February-May 2021.
Patient Demographics
The majority of the participants (76%) were male and at least 60 years old (65%). Self-reported demographics are presented in Table 1. Figure 1 depicts a word cloud with the most frequently occurring words about previous research/learning on lung transplantation. “Video” was the most prominent word indicating that participants most frequently watched the new video series, YouTube videos, or videos on the Lung Saskatchewan website. Thematic analysis identified content around the positive and negative aspects of the videos, transplant concerns, and unanswered questions. These results are presented in alignment with the objectives of the program evaluation.
Word cloud for top 50 words in coded material for response to “have you done any research on your Own?”.
Self-Reported Characteristics of Study Participants.
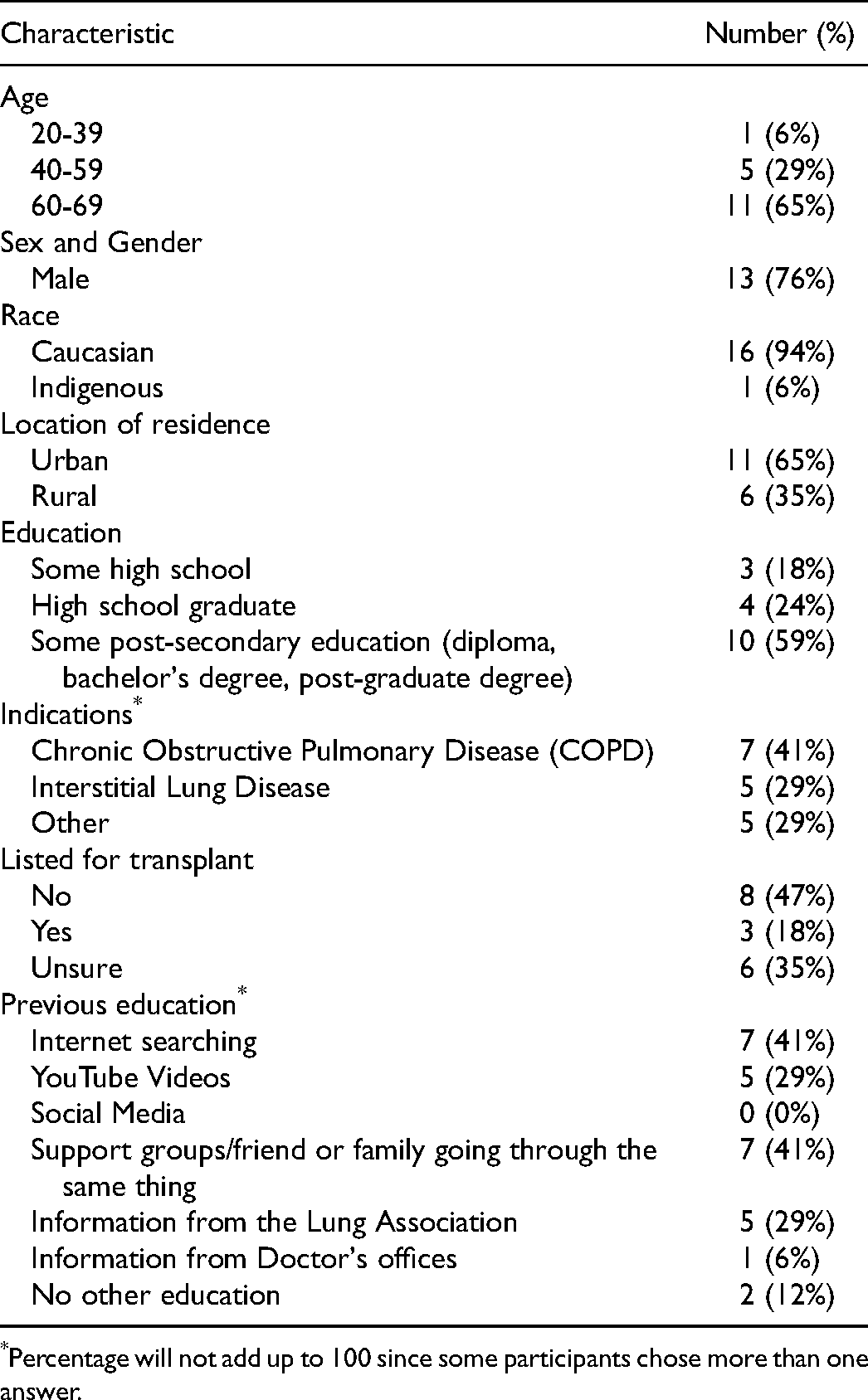
Percentage will not add up to 100 since some participants chose more than one answer.
Objective 1: Satisfaction
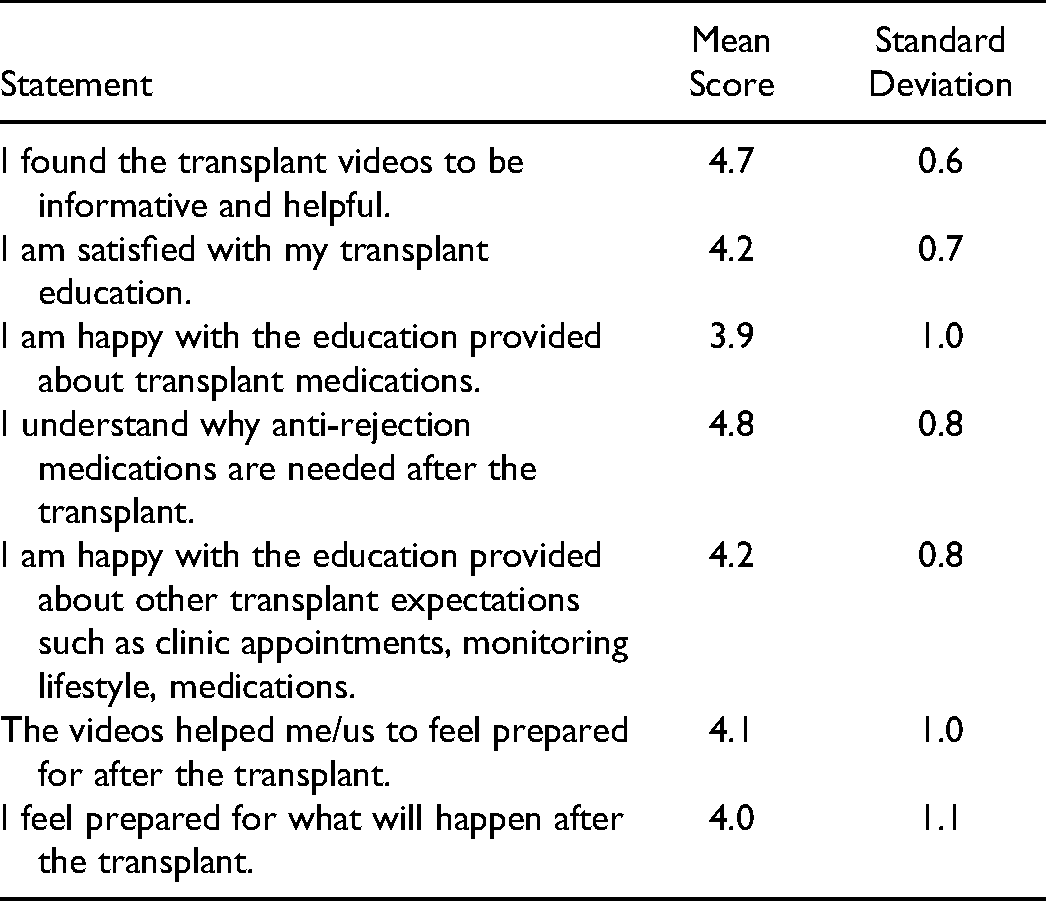
Participants found the videos to be informative and helpful (4.7 on 5-point Likert scale) and were satisfied with their transplant education (4.2/5). The highest scores were received for patients understanding why anti-rejection medications are needed after the transplant (4.8/5) and lowest for happiness with education about transplant medications (3.9) See Table 2. As described by participant 1, the thought of taking so many medications was intimidating.
Video Statement Ratings (Mean and Standard Deviation).
Positive aspects of the videos
Participants appreciated the amount and type of content, and the way it was presented. The content was not overly technical or complicated, covering the right scope of information without being sugar-coated (ie, what to expect throughout the process), while offering a sense of hope. Participant 1 said “it covers what I’m gonna have to do; what's going to happen to my body.” Patients appreciated hearing real-life, experience-based testimonies from individual patients and caregivers. Nearly half of the participants (8/17, 47%) explicitly indicated how much they appreciated genuine accounts. These segments were valued for their relatability, hopeful nature, and practical insights as to what was critical throughout the process.
Negative aspects about the videos
Many participants had difficulty articulating what they liked least about the videos and a third (6/17) could not name anything when directly asked. Participant 4 said, “I don't think there was anything I liked the least… I found it all very informative.” Another participant described the content as “right on the money” (participant 7). Stylistic or technical issues were mentioned by two participants, such as not being able to expand the videos to watch them full screen (participant 14), and the cartoons (participant 16). One participant indicated a desire for more specific information about impending experience at the transplanting center.
Objective 2: Timing
Most participants indicated that the videos should be watched early in the workup process, since this meant there was “time to process the information that we were given, before it became critical that we understand it.” (Participant 1). There were caveats to this such as ensuring videos were not watched at the time of diagnosis (to avoid potential psychological distress) and perhaps watching the videos more than once to reinforce education. Some participants indicated that it was useful to watch the videos after initial conversations with doctors had taken place, since the videos reinforced concepts introduced by medical professionals.
Objective 3: Gaps
Transplant concerns
Participants expressed their fears about aspects of the transplant process, including medications, expenses, and precautions in daily life. Some indicated that the content presented was not necessarily what they were expecting. According to participant 15: “Well it was easy to understand [videos] but kind of hard to swallow knowing that I’d eventually have to go through with that.” Some participants felt intimidated by the medications (eg, nomenclature, mechanism, number of pills, cost), but recognized that clinical situations vary. The thought of life after the transplant was anxiety provoking for some. Participant 1 said, “I think those testimonials sort of really reinforced the fact that the surgery is great, but it's only the first step. There's a lot of work that goes in afterwards, just as much as before a transplant.” The inherent risks involved in the surgery were intimidating, as well as the impact on other stakeholders involved in the donation process, and on caregivers.
Questions unanswered
Participants had some remaining questions about transplantation even after viewing the videos. These included questions about what happens logistically during the out-of-province trips to the transplanting center (n = 6) (eg, what you need to take/pack, how you might get there, cost, accommodations, the role of the caregiver, and what the trip involves). Lingering questions revolved around health status and what is meant by being healthy enough for transplant or how having a lung transplant may impact a co-occurring condition or vice versa (n = 5). Financial supports (n = 2), post-surgery recovery and restrictions (n = 2), the surgery (n = 1), and whether to proceed with the surgery itself or its timing (n = 1) were also discussed. Demographic intake questions posed by the researcher revealed other unanswered questions. For example, 8 participants were not completely sure whether they were listed for transplant or for how long they might have been on the list.
Discussion
Quantitative and qualitative feedback from participants in this program evaluation confirmed that the electronic video series was a timely method for improving pretransplant knowledge during the Covid-19 pandemic. Participants perceived the videos to be helpful and they appreciated the insights of fellow patients, knowing their successes, or feeling their hope. This is not to say there was no emotional struggle in hearing about the risks, medications and aftercare involved, but rather that the videos helped inform in a way that provided a psychological preparedness for what is to come. Participants indicated that the videos would be most useful earlier in the process (ie, after a patient has some pre-existing knowledge, but has not yet been to the transplanting center).
While most participants did not explicitly offer suggestions for improving the videos, this endeavor uncovered valuable information for improving the pretransplant experience. Participants expressed concerns regarding medications, expenses, and day-to-day precautions, and articulated lingering questions about the logistical aspects of transplant, the role of a caregiver, financial issues, and health before and after the surgery. Uncertainty was also discovered regarding placement on the waitlist. These misunderstandings speak to a need for clearer communication between healthcare professionals and patients and increased areas for focused education.
This qualitative study provided rich feedback from participants who viewed the video series, but more study is needed to investigate barriers and reasons from those who did not. The participants were primarily Caucasian, and diverse perspectives are required. Furthermore, the results of this single-center program evaluation are not generalizable to other settings.
Conclusion
Supplemental home-based video education was valuable for providing education information during the Covid-19 pandemic and will be implemented as standard of care within our institution permanently. Based on the success of this program evaluation, the videos will be provided electronically to patients after their first visit with the transplant respirologist. One-on-one visits with the healthcare team will be focussed to address the outstanding gaps identified in this program evaluation, such as placement on the waitlist, and logistical aspects of the transplant process. A resource will also be created to highlight financial supports available to patients.
Supplemental Material
sj-docx-1-pit-10.1177_15269248221107048 - Supplemental material for A Mixed Methods Assessment of Home-Based Video Pretransplant Lung Education
Supplemental material, sj-docx-1-pit-10.1177_15269248221107048 for A Mixed Methods Assessment of Home-Based Video Pretransplant Lung Education by Holly Mansell, Mark E. Fenton, Julian S. Tam, Nicola Rosaasen, Louise Cardinal and Nicole Nelson in Progress in Transplantation
Footnotes
Acknowledgments
The authors thank Rachel Tang from CHASR for providing a third-party program evaluation report that facilitated the writing of this manuscript, as well as Erin Kuan, Jennifer May, Jill Hubick and Trent Litzenberger from Lung Saskatchewan for their support and review of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Respiratory Research Centre at the College of Medicine, University of Saskatchewan. Lung Saskatchewan funded the development of the video intervention that was used in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.