
Abstract

Keywords
Donation after circulatory death (DCD) has been successfully utilised to expand the potential donor pool and keep up with the ever-increasing demand for livers for transplantation. 1 The main limitation of this approach is the extra warm ischemic injury, which is not experienced in donation after brainstem death (DBD), and which impacts on rates of early allograft dysfunction, primary non-function (PNF), ischemic cholangiopathy and graft failure. 1
In situ Normothermic Regional Reperfusion (NRP) was pioneered in Spain 2 and has emerged as a promising technique to minimise the impact of this additional warm ischemic injury by restoring an oxygenated blood supply to the abdominal organs following circulatory arrest utilising an Extracorporeal Membrane Oxygenation (ECMO) circuit. NRP allows assessment of organ function as well as replenishment of adenosine triphosphate (ATP) reserves prior to cold storage and data so far suggests that it is associated with increased utilisation of organs and reduction in the rates of early allograft dysfunction and ischemic cholangiopathy.2,3
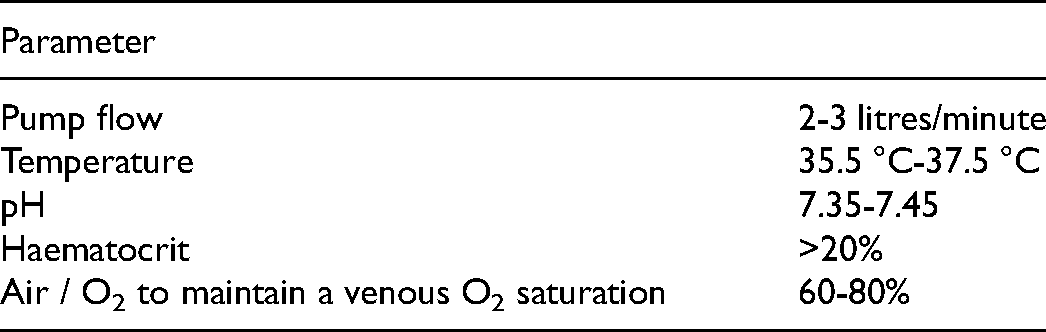
We established a programme of NRP in 2010 and to date have perfused over 137 donors. With this experience, 3 we have developed a protocol with organs perfused with oxygenated blood at 37 °C for a period of 2 hours with the following physiological and biochemical targets: See Table 1.
Normothermic Regional Perfusion Parameters.
As this technology becomes more widespread, there will undoubtedly be a learning curve in each centre that adopts it. While we are certainly advocates of this technology and approach, we wish to underline that despite their limitations conventionally recovered DCD organs remain an excellent life-saving resource 1 and if difficulties arise in establishing adequate flows on NRP then the fallback position should be to promptly return to a strategy of cold perfusion and rapid retrieval to ensure safe and maximal utilisation of organs. During time-critical and pressurised decision making, there needs to be a robust muscle memory approach that does not require the development of new thinking. In medicine the best known of these approaches is the ABC (or Airway, Breathing & Circulation) approach to resuscitation.
As such, we have developed and wish to share our 6Cs troubleshooting algorithm for a rapid and systematic approach to troubleshooting poor flows during NRP (Figure 1). This will help to ensure that issues are swiftly resolved and/or the decision is made to initiate cold perfusion and organ procurement without undue procrastination at the cost of damage to or loss of organs (Figure 1).
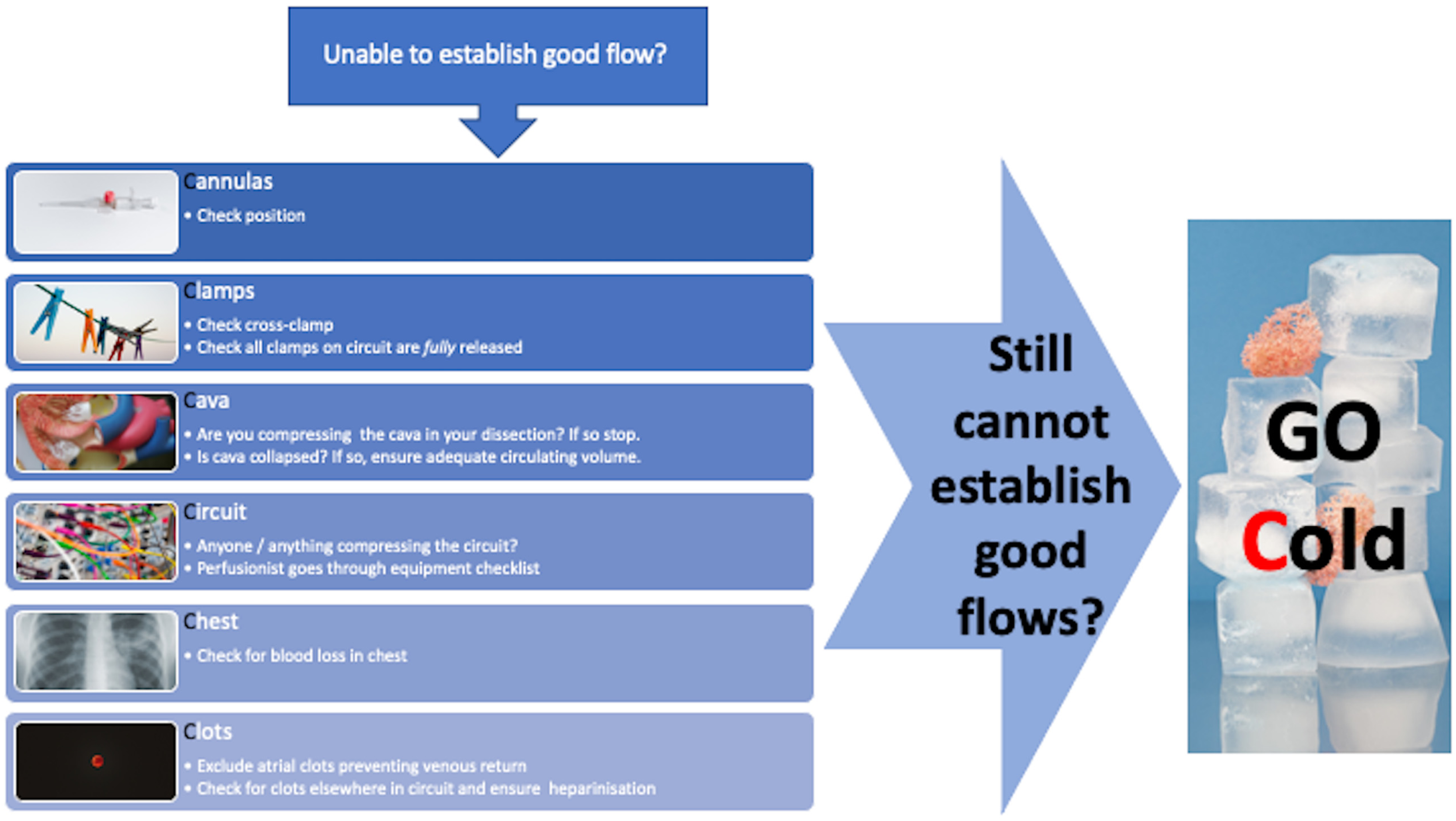
The 6Cs troubleshooting algorithm for Normothermic regional reperfusion.
Footnotes
Abbreviations
Author Contributions
JR, RG, AB and CW have made a substantial contribution to the conception and writing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Andrew Butler is part owner of a patent on the circuit used by the OrganOx metra device; he does not feel this has any relevance to this article. The remaining authors declare no conflicts of interest.
Funding
This framework was developed within the Cambridge Transplant Unit, which is funded in part by the National Institute for Health Research Blood and Transplant Research Unit (NIHR BTRU) in Organ Donation and Transplantation at the University of Cambridge in collaboration with Newcastle University and in partnership with NHS Blood and Transplant (NHSBT). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health or NHSBT. JR was also supported by a NIHR Academic Clinical Lectureship.