
Abstract
Background:
Vesicoureteral reflux (VUR) is frequently found after transplantation, but its impact on graft function, urine tract infection, and graft loss remains uncertain. Therefore our objective was to evaluate the effects of VUR on the outcome of renal transplantation.
Material and Methods:
We included 1008 adult renal transplant recipients of whom a 1-week posttransplant voiding cystourethrogram was available. Study end points included occurrence of bacteriuria, renal function, and graft survival.
Results:
In total, 106 (10.5%) of 1008 graft recipients had a diagnosis of VUR on voiding cystography. The incidence of bacteriuria was comparable in the reflux and nonreflux group (17% vs 17.4%, P = .91). There was no significant difference in renal function at 3 months and 1 year in patients with and without VUR. One- and 5-year graft survival in patients with VUR was 85.8% and 82.1% compared to 87.3% and 83.0% in patients without VUR (P = .68 and P = .80).
Conclusion:
Posttransplant VUR has no correlations with early bacteriuria, renal function, and graft survival.
Background
Urological complications are the most frequent technical adverse event after renal transplantation and can have a significant effect on long-term allograft survival and loss. Vesicoureteral reflux (VUR) into the transplanted kidney occurs frequently after transplantation. 1 However, the effect of VUR on both early and late graft function and graft survival remains doubtful. Early findings indicated VUR as an important cause of late renal-graft failure. 2 More recent studies did not convincingly support this evidence. 3 –9 Urine tract infection (UTI) is a common finding after kidney transplantation, with incidences ranging from 6% to 86%, thereby making it the most frequent infection in renal transplant recipients. 10,11 The aim of this study was to investigate the impact of VUR on short-term and long-term clinical graft outcomes and early postsurgical bacteriuria frequency in our renal transplant series.
Material and Methods
Design
A retrospective cohort study was performed. This retrospective chart review was exempted from the institution’s ethical board review.
Setting
The study took place at the Academic Medical Center of Amsterdam.
Population
In this retrospective study, we included 1008 of 1358 adult patients who underwent kidney transplantation at the Academic Medical Center of Amsterdam, between January 1995 and April 2012. For study inclusion, a posttransplant voiding cystourethrogram (VCUG) had to be available. Absence of a VCUG was the only exclusion criteria for this study.
Data Collection
Patient charts and surgical reports were reviewed retrospectively. Patient baseline characteristics are represented in Table 1.
Baseline Characteristics and Results.
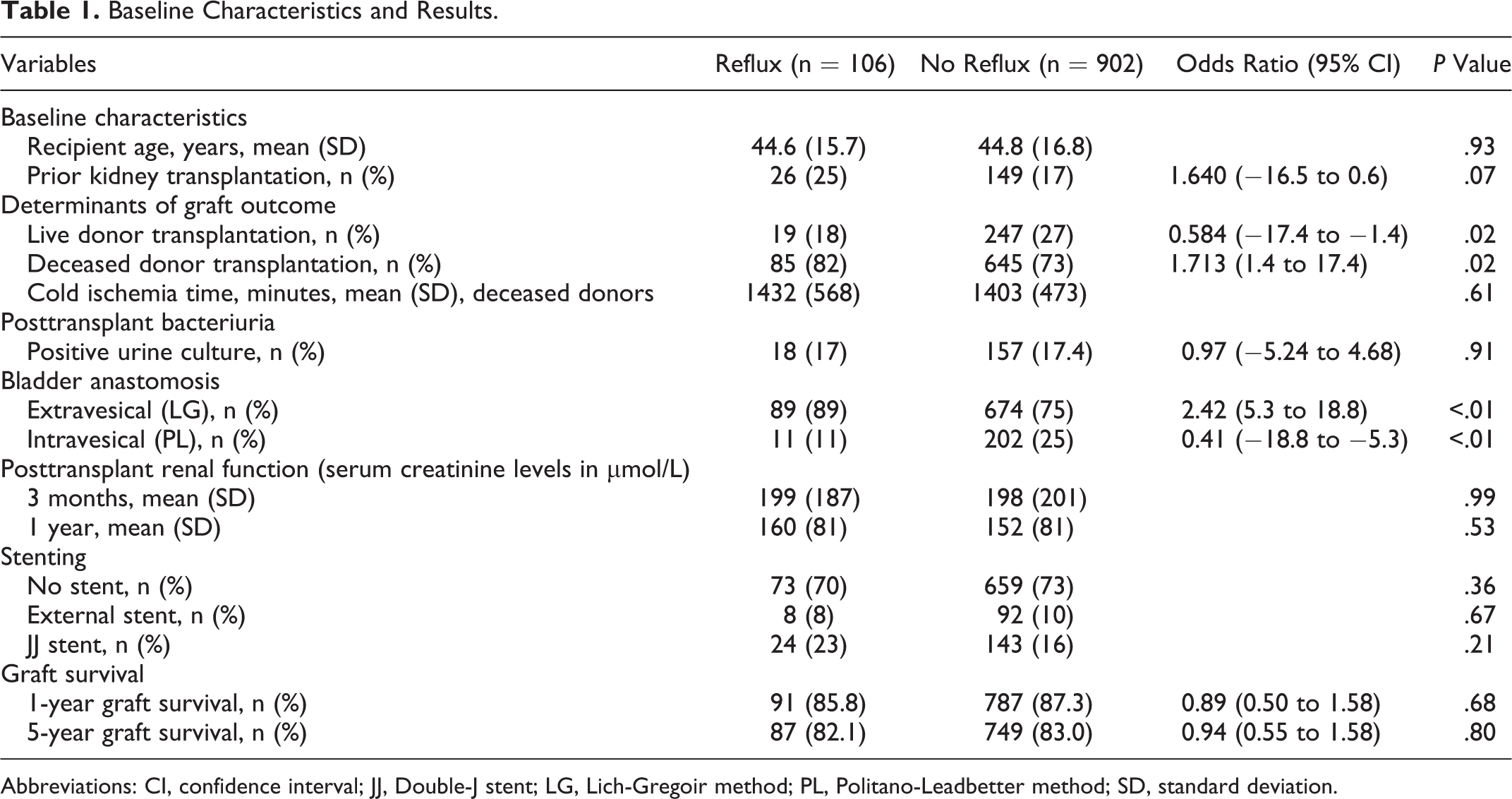
Abbreviations: CI, confidence interval; JJ, Double-J stent; LG, Lich-Gregoir method; PL, Politano-Leadbetter method; SD, standard deviation.
For this study, documented end points included occurrence of bacteriuria during the initial hospital stay (asymptomatic or UTI), renal function (serum creatinine levels after 3 months and 1 year), and graft survival. Graft survival was defined as being alive with a functioning graft (free from dialysis or repeat renal transplantation). Diagnosis of bacteriuria included both asymptomatic bacteriuria and UTI. The diagnosis of UTI was based on both clinical symptoms (dysuria, urgency, frequency, fever, and tenderness of renal allograft) suggestive for UTI along with bacteriuria. In case of clinical diagnosis of UTI, bacteriuria was defined as a positive midstream urine specimen culture showing growth of an uropathogen with at least 104 colony-forming units per milliliter (CFU/mL). Asymptomatic bacteriuria was defined as a bacteriuria (at least 105 CFU/mL) without any clinical symptoms suggestive for UTI. Specimens were taken after catheter removal and during the initial hospital stay. Surveillance for bacteriuria occurred through screening for leukocyturia within the urine sediment. In case of leukocyturia, a urine culture was taken. A urine culture was also taken in case of fever or urinary tract symptoms.
Data Analysis
Continuous data were given as the mean, the 95% confidence interval, and the standard deviation. For comparison between these continuous data, which had a normal distribution, the independent samples t test was used. Discrete data were displayed as counts and percentages and for comparison of categorical data we used z tests. Kaplan–Meier analysis was used to calculate graft and patient survival. A 2-sided P value of <.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS statistic for Mac OS, version 21.0 (IBM Corp, Armonk, New York).
Procedure
All transplantations were performed through an extraperitoneal approach in the iliac fossa. All recipients received 1 gm of cefamandole intravenously as antibiotic prophylactic 30 minutes prior to incision. In 2011, cefamandole was switched to 1 gm cefazolin. The method used to establish urinary continuity was either the extravesical ureteroneocystostomy (Lich–Gregoir method) or the intravesical ureteroneocystostomy (Politano–Leadbetter method), according to personal preference of the surgeon . Until July 2005, all ureter–bladder anastomoses were performed without stenting. From July 2005 onward, all renal transplant recipients received a 5-day 8F external stented ureteroneocystostomy. The stent was introduced into the bladder through a direct suprapubic bladder puncture and positioned in the transplant renal pelvis. From 2007, the stent protocol changed. Living renal transplants had continuous use of the external 8F splint, but the deceased donor renal transplants received a 12-cm long 6F ureteral double-J stent for 6 weeks. Postoperatively, all patients had an indwelling bladder catheter, which was removed in all patients on day 7 after urinary leakage had been excluded by VCUG. Voiding cystourethrogram was reviewed by a radiologist and scored on the presence of VUR in the transplanted kidney. When contrast fluid was present in the transplanted ureter or pyelum, VUR was diagnosed. No grading was used. All patients were followed at our center for at least 1 year after successful transplantation. After 1 year, most patients were transferred to their referral center.
Results
In total, 106 (10.5%) of 1008 graft recipients had a diagnosis of VUR on VUCG. Table 1 presents the baseline characteristics and the results. No significant difference was observed in renal function at 3 months and 1 year between both groups.
The incidence of bacteriuria was 17.4%. Incidence rates did not differ significantly between patients with or without reflux; 17.0% of the patients with VUR were diagnosed with a bacteriuria and 17.4% of the nonreflux group (P = .91).
Rates of VUR did differ with the implementation technique, with a higher incidence of VUR with the Lich–Gregoir method compared to the Politano–Leadbetter method (12.0% vs 5.0%; P < .001). The UTI rate was 24.9% with the Lich–Gregoir method compared to 15.2% with the Politano–Leadbetter method (P < .01).
Rates of VUR did not significantly differ with different stenting protocols. The incidence of VUR in the nonstent group was 10.0%, compared to 8.0% in the external stent group and 14.0% in the double-J stent group (P = .178).
Bacteriuria rate did show a difference between stenting protocols with an incidence of 23.0% in the nonstent group compared to 3.0% and 1.7% in the external stent and the Double-J stent group (P < .05), respectively.
There was no significant difference in graft survival at 1 and 5 years between both groups, as can been seen in the Kaplan–Meijer survival curve in Figure 1.
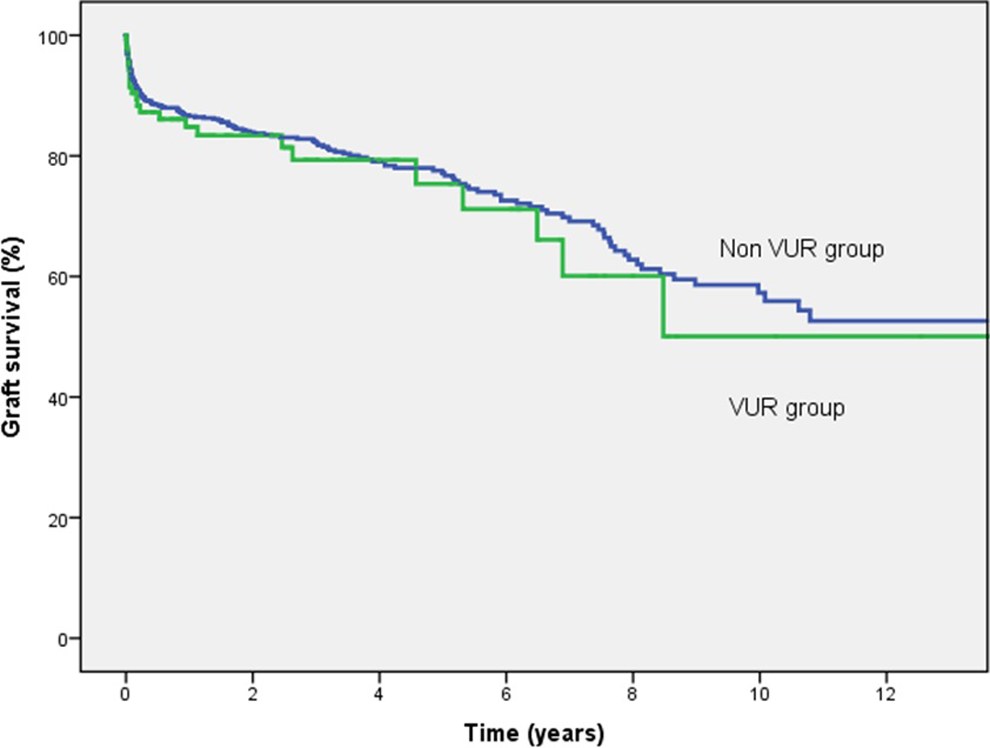
One- and 5-year graft survival rates for patients with and without vesicoureteral reflux.
Discussion
In our retrospective study of 1008 kidney transplant patients, we found a VUR rate of 10.5%. The overall incidence of bacteriuria was 17.4%, which did not differ significantly between patients with or without VUR. No effect of VUR has been observed on renal function and graft survival.
Previously published data reported a highly variable incidence of VUR, with incidences of VUR up to 86%. 4,7 Voiding cystourethrogram in these studies, however, was sometimes performed in selected patient cohorts, instead of our standardized per-protocol VCUG. Margreiter et al reported an incidence of VUR of 40.7%, which is considerably higher than our 10.5%. Our cohort showed a significantly lower incidence of VUR using intravesical ureteroneocystostomy compared to the extravesical method, which has not been used in patients of the cohort of Margreiter et al. In accordance with the findings of Margreiter et al, we found that the incidence of VUR was higher among patients receiving a deceased donor kidney compared to live donor transplants.
Bacteriuria, especially when it is recurrent, influences renal allograft outcome unfavourably. 10,12 The overall prevalence of bacteriuria was 17.4% in our patient group. Other studies have reported an incidence ranging from 6% to 86%. 10 The VUR has been discussed as being of a possible influence on the occurrence of bacteriuria, but findings have been inconclusive. Most studies did not find a relation between VUR and occurrence of bacteriuria, 4,5,7 which is in accordance with our findings.
Main objective of this study was to contribute to the debate whether VUR is of influence on graft function and survival. To evaluate graft function, we used creatinine levels at 3 months and 1 year. Several other studies report on graft function using either creatinine levels or estimated glomerular filtration rate (GFR). Coosemans et al 3 measured creatinine levels at several time points and only found a significant difference at day 1 and day 7, after which this difference disappeared. However, Coosemans et al only had a VUR population of 3.82% (n = 15). Two other studies could not find a difference as well. 4,5 Inoue et al found the existence of VUR was independently associated with a 24-hour creatinine clearance of less than 60 mL/min (odds ratio = 2.993; P = .033). 6 Margreiter et al could only find significantly lower estimated GFR (eGFR) levels at 1-year posttransplantation; the difference disappeared at 3 and 5 years posttransplantation. 7 Our results are in accordance with the current literature, which during a follow-up period of 2 to 5 years did not demonstrate significant graft survival rates in patients with or without VUR. 3,5,7
Although our population has reached a large number, our study still has its limitations. Primarily, it is a retrospective study, and of the 1358 patients who received a kidney transplant, only 1008 could be included since VCUG was lacking in 350 patients. Also, there were no follow-up VCUGs available. Unknown is whether reflux could disappear naturally after a few weeks when the surgical site is completely healed or whether reflux actually can arise later on. Earlier findings show that VUR may change with time after surgery. 13
Observation of bacteriuria only took place during initial admission to the hospital. Bacteriuria diagnosed at some other point during follow-up was not registered.
We used serum creatinine to objectify graft function. Unfortunately, we did not have enough data to calculate eGFR. Lack of data on bodyweight among others makes the use of serum creatinine as graft function less reliable.
Conclusion
Our study reported on the largest number of patients so far concerning VUR. In our data, no indications were found demonstrating that VUR has a negative influence on graft function, or graft survival rates of bacteriuria, renal function, and graft survival did not differ between patients with or without posttransplant VUR.
Footnotes
Authors’ Note
There are no other contributors to this paper. No financial support has been given.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.