
Abstract
Introduction:
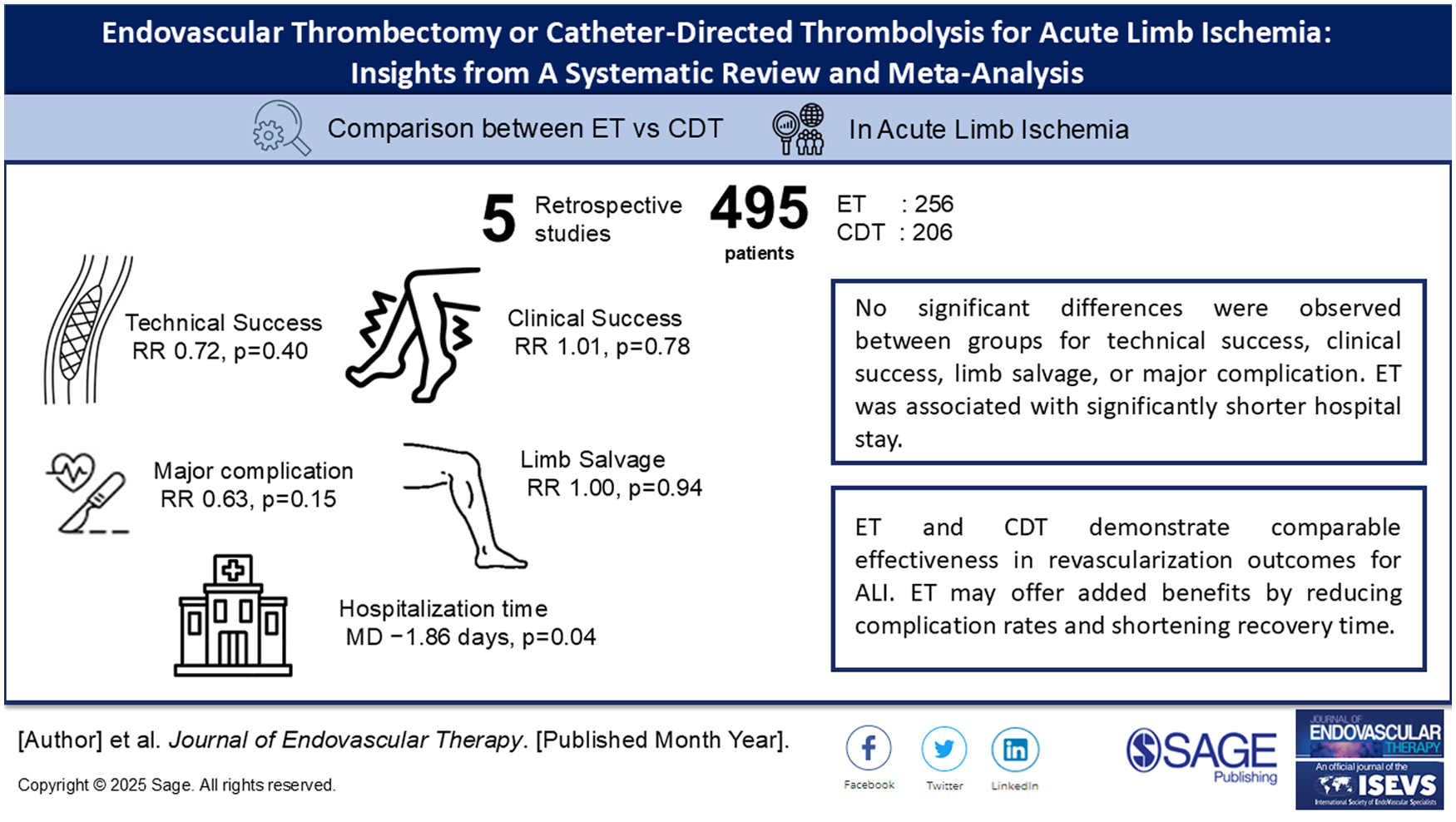
Acute limb ischemia (ALI) is a vascular emergency requiring prompt revascularization to prevent limb loss and death. Endovascular thrombectomy (ET) and catheter-directed thrombolysis (CDT) are the most commonly used strategies. Despite their increasing use, comparative effectiveness and safety remain unclear. This study aims to compare the clinical outcomes between ET and CDT in patients with ALI.
Methods:
This systematic review and meta-analysis followed PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) 2020 guidelines and was registered in PROSPERO (CRD42024590036). A comprehensive literature search in scientific databases was conducted up to December 2024. Studies comparing ET and CDT in adult patients with ALI were included. Data were pooled using random- or fixed-effects models depending on heterogeneity. Sensitivity and publication bias analyses were performed.
Results:
Five retrospective studies with 495 patients (ET: 256; CDT: 206) were analyzed. No significant differences were observed between groups in terms of technical success (risk ratio [RR]=0.72, p=0.40), clinical success (RR=1.01, p=0.78), or limb salvage (RR=1.00, p=0.94). ET was associated with a longer procedure duration (mean difference [MD]=57.80 minutes, p=0.03) but shorter hospital stays (MD=−1.86 days, p=0.04). Major complications were lower in the ET group, the difference was not statistically significant (RR=0.63, p=0.15). Cost reporting was heterogeneous, suggesting a potential trade-off in which ET has higher upfront costs but shorter hospitalization.
Conclusion:
ET and CDT demonstrated comparable effectiveness in revascularization outcomes for ALI. ET may offer added benefits by reducing complication rates and shortening recovery time. The choice between interventions should take patient-specific factors into account.
Clinical Impact
This study supports the use of endovascular thrombectomy (ET) as an effective alternative to catheter-directed thrombolysis (CDT) due to its favorable safety profile, demonstrated by lower rates of major complications and shorter hospital stays. ET may be particularly suitable in patients with a high bleeding risk. However, individual patient anatomy and comorbidities remain critical determinants in treatment selection. Institutional factors and cost-effectiveness considerations also play important roles in determining the choice of intervention. Overall, both techniques ET and CDT are effective revascularization strategies for restoring arterial perfusion in acute limb ischemia.
Keywords
Get full access to this article
View all access options for this article.