
Abstract
Clinical Impact
Fracture of a proximal sealing stent ring is a rare complication following fenestrated endovascular aortic repair (FEVAR). Even rarer can a proximal stent ring fracture with dislodgement and widespread retroperitoneal dissemination of nitinol fragments. This rare complication, which may manifest as transient abdominal pain, could result in severe clinical sequalae. Therefore, plain abdominal radiography should be considered in patients post-FEVAR presenting with epigastric or abdominal pain to assess stent integrity.
Fracture of a proximal sealing stent ring is a rare complication following fenestrated endovascular aortic repair (FEVAR).1–5 The literature regarding stent-graft fractures is limited to case reports, there are no cohort studies reporting on this complication. While the radial force exerted by the stent ring is believed to contribute to the fracture, the fractured stent rings typically remain within the aortic lumen. We present a rare case of proximal stent ring fracture with dislodgement and widespread retroperitoneal dissemination of nitinol fragments. Written publication consent was obtained from the patient and, following the patient’s death, from a legal representative.
A 71-year-old man with a juxtarenal abdominal aortic aneurysm (maximum diameter 86 mm) underwent FEVAR using an Anaconda device (Terumo Aortic, Inchinnan, Scotland, UK) with 2 renal fenestrations (Figure 1). Follow-up with computed tomography angiography (CTA) at 1 month and 1 year demonstrated no abnormalities and intact proximal stent rings (Figures 1 and 2). The patient had a right sided common iliac artery aneurysm that was untreated after the initial repair, which resulted in a reintervention after 3 months; the right internal iliac artery was embolized, and the right limb extended to the right external iliac artery. No other clinical or non-clinical events of relevance occurred. Two years post-procedure, the patient with established coronary artery disease, including 2 episodes of acute myocardial infarction requiring stenting, was admitted with severe epigastric and retrosternal pain with tightness around the chest. The patient recognized these symptoms from prior to his previous myocardial infarctions, and was subsequently admitted to the cardiology department. The patient remained in stable condition throughout the hospital admission, and laboratory testing and coronary angiography revealed no abnormalities. Upon admission the pain was already steadily improving, with complete disappearance the following day, and after 3 days the patient was discharged without a definitive diagnosis.
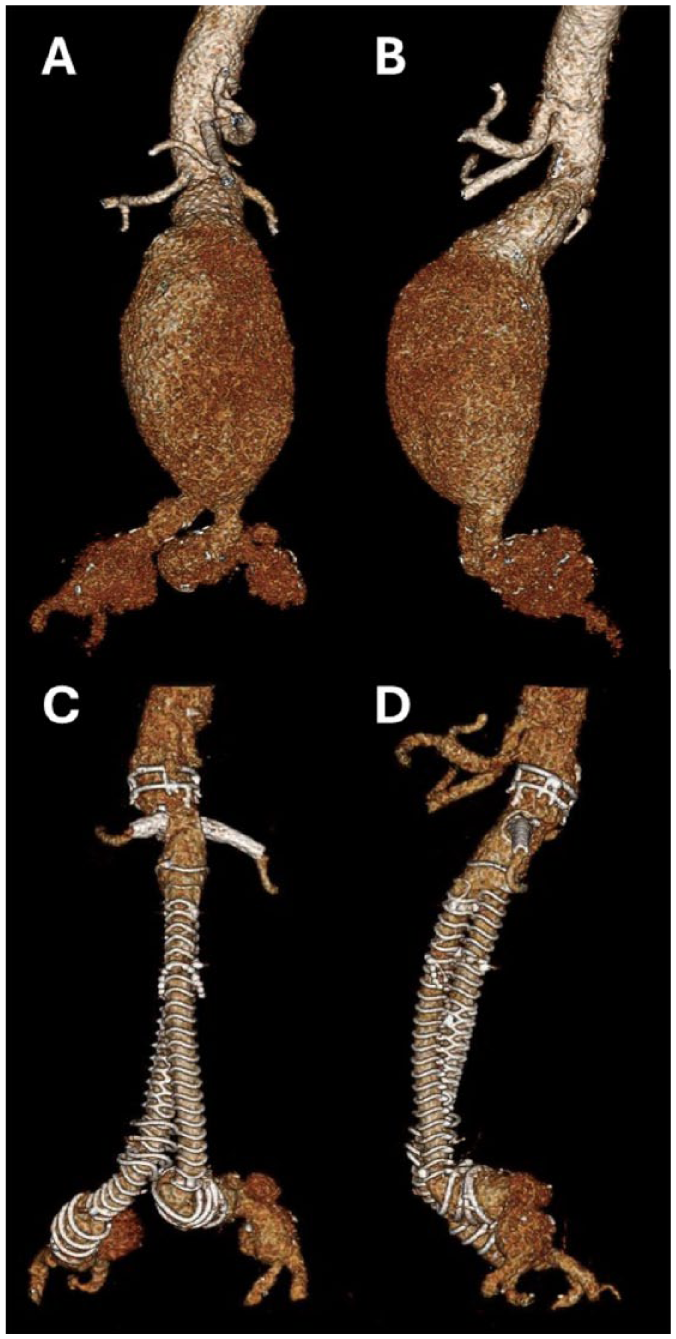
3D reconstruction of computed tomography angiography demonstrating a juxtarenal abdominal aortic aneurysm prior to treatment with a fenestrated endograft (A and B), and at 1-month follow-up post treatment (C and D).
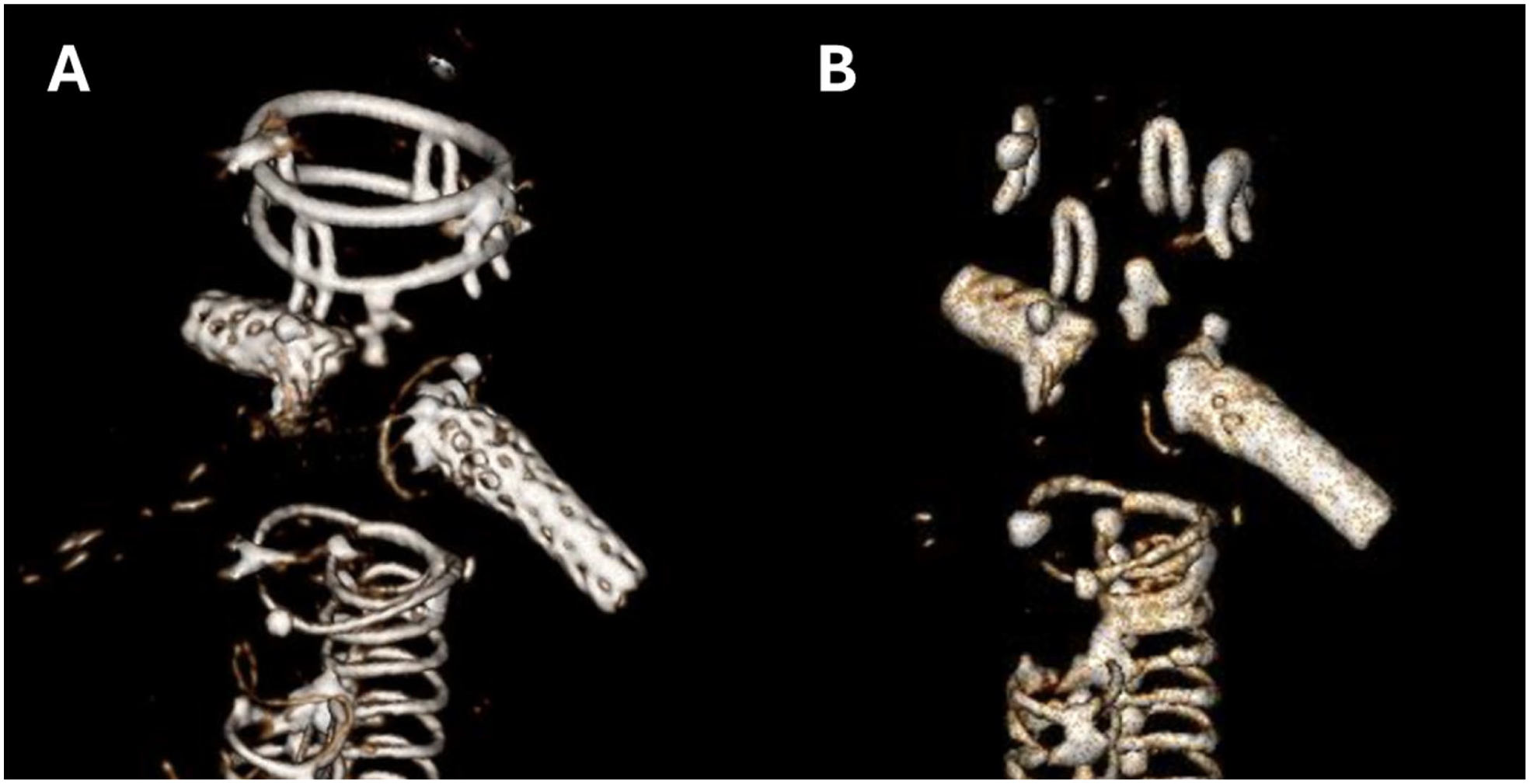
(A) Follow-up computed tomography angiography (CTA) at 1 year demonstrated no complications and intact proximal stent rings, while (B) CTA after 2-year follow-up demonstrated disappearance of both proximal stent rings.
Routine post-FEVAR follow-up revealed disappearance of the proximal 2 stent rings on plain abdominal radiographs and CTA (Figure 2). Inspection of the CTA identified multiple fragmented nitinol wires scattered throughout the upper abdomen, particularly adjacent to and perforating the left kidney and liver (Figures 3–5). These findings were first identified 1 month after the episode of acute pain. No abdominal imaging had been obtained during hospitalization.
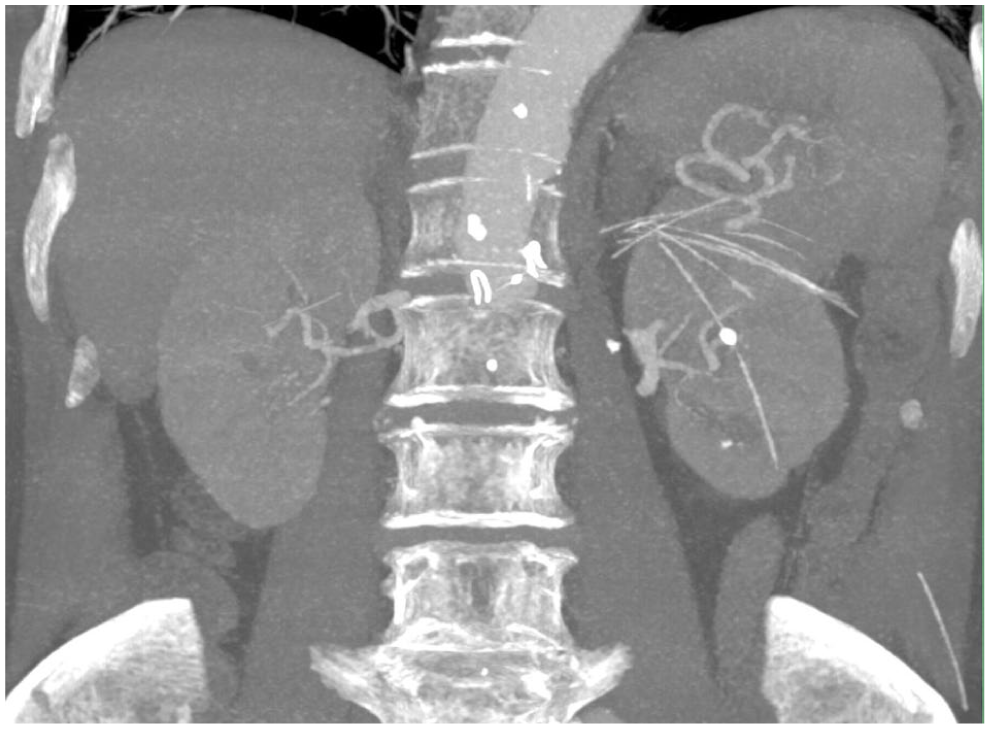
Frontal computed tomography angiography demonstrating multiple fragmented nitinol wires scattered throughout the upper abdomen, particularly adjacent to and perforating the left kidney. The fragments originate from a fractured proximal sealing stent ring of a fenestrated endograft.

Transverse computed tomography angiography demonstrating multiple fragmented nitinol wires scattered throughout the upper abdomen, particularly adjacent to and perforating the left kidney and liver. The fragments originate from a fractured proximal sealing stent ring of a fenestrated endograft.
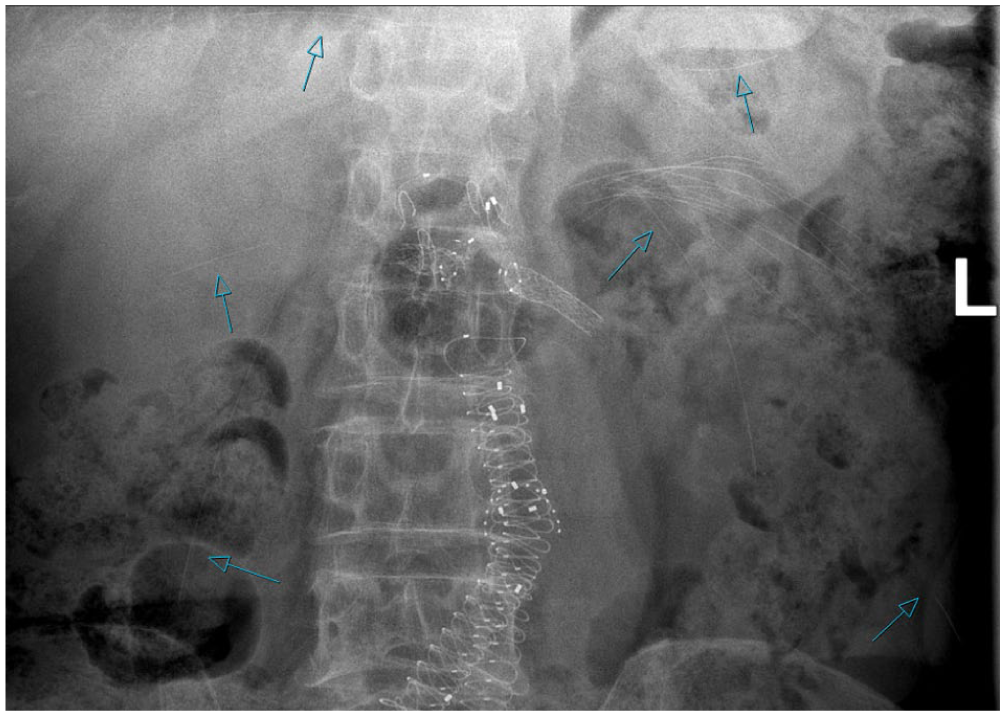
Plain abdominal radiography after 2-year follow-up demonstrating the disappearance of both proximal stent rings and nitinol fracture remnants (arrows) in different locations across the retroperitoneum, left and right kidney, spleen, liver, and left thigh.
Retrospectively, the scattered nitinol fragments are presumed to have caused the transient symptoms. The positioning of the nitinol wires outside the aortic lumen after the sent-fracture requires that the wires perforated the aortic wall. In this case no clinical sequels were noted specifically due to the puncturing of the aortic wall, possibly due to sealing of the puncture site by the endograft. Moreover, there were no clinical sequelae such as hemorrhage, organ injury, or bowel perforation, apart from an episode of microscopic hematuria. During the following 3 years, the fragments remained stable in position, the target vessels remained patent, and a small type 3c endoleak from the right renal artery was observed but did not require reintervention. The patient died 5 years after the FEVAR due to chronic obstructive pulmonary disease.
This case highlights that proximal stent ring fracture after FEVAR can result in extensive retroperitoneal dissemination of wire fragments, which may manifest as transient abdominal pain, but could result in severe clinical sequalae. Plain abdominal radiography should be considered in patients with an Anaconda endograft presenting with epigastric or abdominal pain to assess stent integrity.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.J.Z. is consultant for Terumo Aortic. E.W.M.H., M.J.v.d.L., and I.F.J.T. have no conflicts of interest.