
Abstract
Purpose:
Triple arch branch repair has emerged as a feasible option for high-risk patients unsuitable for open surgery. In high-risk patients, severe pulmonary compromise of pulmonary function due to chronic obstructive pulmonary disease (COPD) can be found. This condition is associated with a higher risk of postoperative complications after general anesthesia and intubation.
Clinical Case:
In this clinical case, we describe the technical aspects of triple arch branch repair under sedo-analgesia, in a patient with severe COPD, unsuitable for intubation. Precise graft deployment was obtained, and no postoperative complications occurred.
Conclusion:
Triple arch branch repair under sedo-analgesia emerges as a viable option for high-risk patients with severe pulmonary compromise, obviating the need for general anesthesia and intubation. This clinical case elucidates the procedure, accentuating both its advantages and limitations, while suggesting the necessity for further validation of its safety in future studies.
Clinical Impact
The execution of complex endovascular aortic arch repair under sedo-analgesia allows for the expanded applicability of these techniques even in high-risk patients who, due to respiratory issues, cannot undergo general anesthesia and intubation.
Keywords
Introduction
Triple arch branch repair has become a viable option for high-risk patients, unfit for open surgery. Mortality and stroke rates are acceptable, with a not negligible rate of reintervention. 1
To reduce the invasiveness of this procedure in a group of high-risk patients, percutaneous access first, and a total transfemoral approach soon after, have been described.2,3 One of the most common risk factors in patients with aortic disease is smoking, which also represents the strongest risk factor associated with chronic obstructive pulmonary disease (COPD). Therefore, the association between aortic pathology and COPD is far from uncommon. COPD is a well-established predictor of complications after general anesthesia and intubation, which are normally required for arch branch repair procedures. In this clinical case, we describe technical aspects of triple branch arch repair under sedo-analgesia, to reduce complications associated with mechanical ventilation in high-risk patients with severe compromise of pulmonary function.
Clinical Case
A 69-year-old female patient was referred to our department due to a Kommerell’s Diverticulum symptomatic for dysphagia. Medical history included active smoking (60 packs/year), hypertension, mild chronic cardiac failure with diastolic dysfunction, and severe COPD requiring supplemental oxygen therapy (GOLD classification grade 3). The preoperative computed tomography (CT) scan demonstrated the presence of a 3.9 cm Kommerell’s Diverticulum and a 5.4 cm descending thoracic aneurysm (Figure 1). During the preoperative evaluation, pulmonary function tests (PFTs) demonstrated a severe obstructive pattern with persistent airflow obstruction after bronchodilator administration: forced expiratory volume at 1 second (FEV1) 47% of predict, Tiffeneau index 61%, vital capacity 65%, carbon monoxide diffusing capacity 33%. Due to the anatomy and patient’s general condition, a 2 stages procedure was planned: right carotid-subclavian bypass first and triple branch repair after.
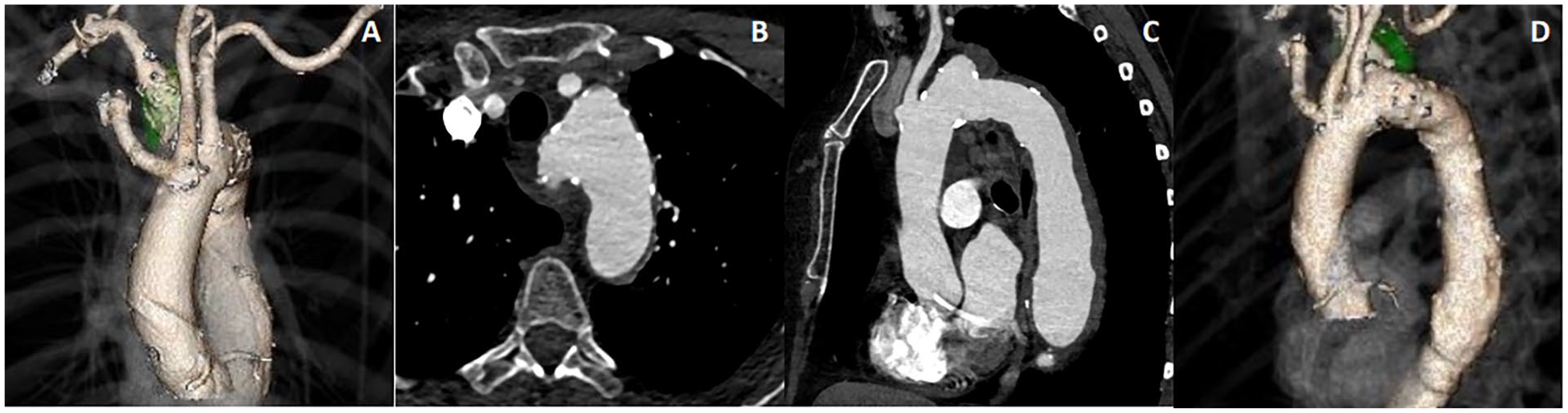
Preoperative CT scan. (A) Anterior view of 3-D reconstruction, (B) axial view, (C) sagittal view, and (D) lateral view of 3-D reconstruction. CT, computed tomography.
Right carotid-subclavian bypass was performed under regional anesthesia with plexus anesthesia and right cervical block. Postoperative course was uneventful, and the patient was discharged at home. After 1 month, the patient was newly admitted to our department for a second-stage procedure, but a worsening of pulmonary function with orthopnea was recognized. COVID-19 test was performed with a positive result. After starting COVID-19 medical therapy (antiviral medications), the patient was discharged. With a negative COVID-19 test, a new PFT was carried out with an FEV1 of 43% of prediction. At this point, after a multidisciplinary evaluation with the anesthesiologist and pneumologist, the decision of performing the triple branch arch repair without general anesthesia and mechanical ventilation was made.
The operation was performed in a hybrid room (Artis Zeego; Siemens Healthcare, Erlangen, Germany). Monitoring included electrocardiography, arterial oxygen saturation (pulse oximetry), near-infrared spectroscopy, and continuous pressure measurement in the left radial arterial right jugular vein access as well as respiratory rate (capnography). Sedo-analgesia was performed with Remifentanil (0.01–0.02 mg/kg/min) and Propofol (0.01–0.02 µg/kg/min) associated with local anesthesia lidocaine 1% (10 ml) and ropivacaine 0.5% (10 ml).
Bilateral femoral percutaneous access and right axillary cutdown were obtained. A custom-made graft (Cook Medical, Bloomington, IN, USA) was implanted with 1 antegrade branch for the right common carotid artery and 2 retrograde branches for the left common carotid artery (LCCA) and left subclavian artery (LSA) (Figure 2). Graft deployment was performed under rapid right ventricle pacing until 180 bpm obtaining 90 mmHg systolic blood pressure. The operation was completed with the right common carotid bridging stent from the right axillary cutdown and LCCA and LSA bridging stent from the right femoral access. Lusoria artery was plugged just proximally to the origin of the right vertebral artery (Figure 3).
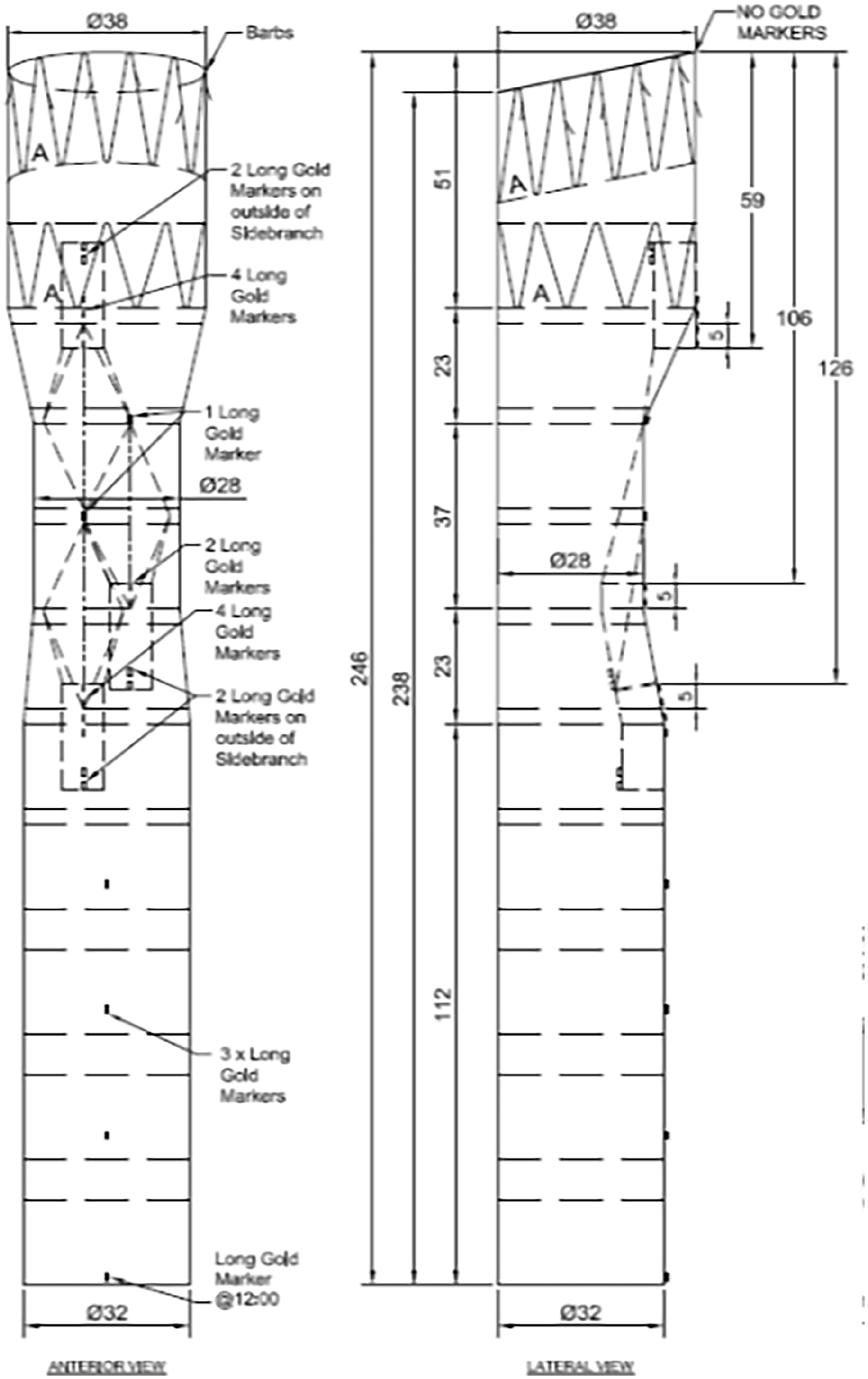
Custom-made graft plan with 1 antegrade branch for the right common carotid artery and 2 retrograde branches for the left common carotid artery and left subclavian artery (Cook Medical, Bloomington, IN, USA).
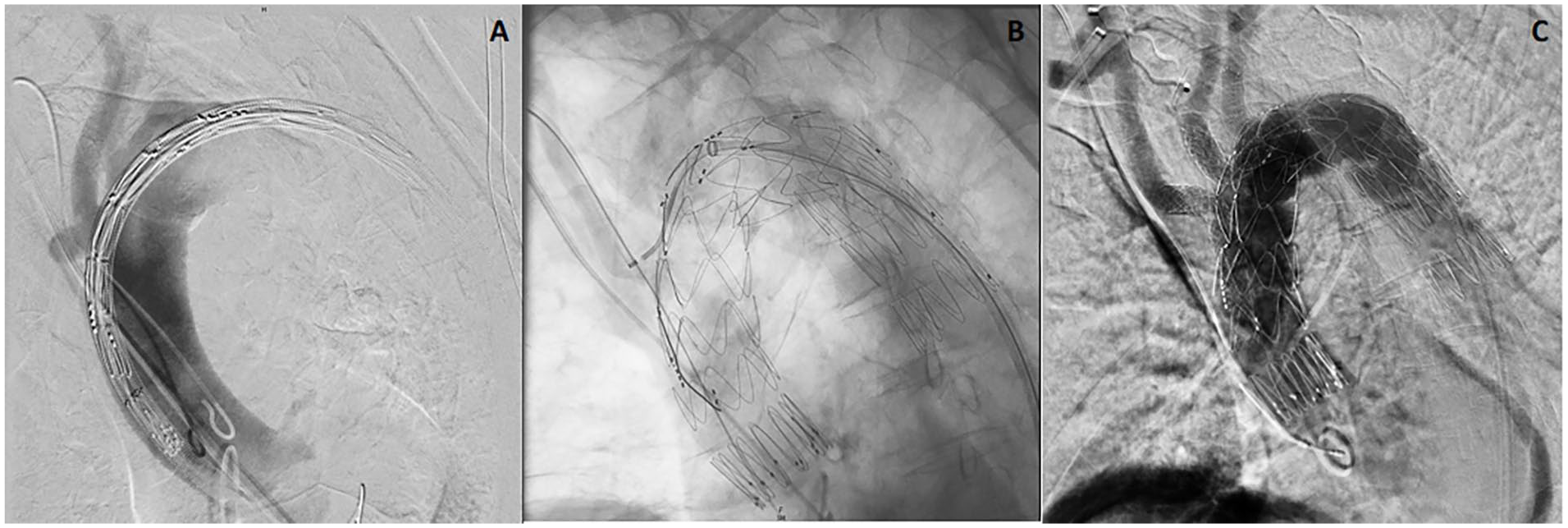
Intraoperative details. (A) Preoperative angiography, (B) full deployment of the triple branch endograft, and (C) completion angiography.
The patient was able to stay in apnea during angiography and graft deployment; after that, the level of sedation was increased to keep the patient still until the end of the procedure.
No significant changes in the patient’s general condition occurred during the entire procedure.
Technical success was obtained with precise graft deployment and successful bridging stenting.
Completion angiography confirmed the complete exclusion of the aneurysm, with patency of the aortic graft and of all the bridging stents in the absence of endoleak. To reduce the time of the procedure and the risk of spinal cord ischemia, a third procedure was planned with distal thoracic endograft positioning.
Total procedure time was 3 hours, fluoroscopy time was 35 minutes, with 221 ml of iodine contrast medium used.
The patient was admitted to the Intensive Care Unit for 2 days for postoperative monitoring. No postoperative complications occurred, especially no neurological complications and no worsening of pulmonary function. The patient was discharged home on the seventh postoperative day. CT scan at discharge confirmed the good result of the procedure (Figure 4).
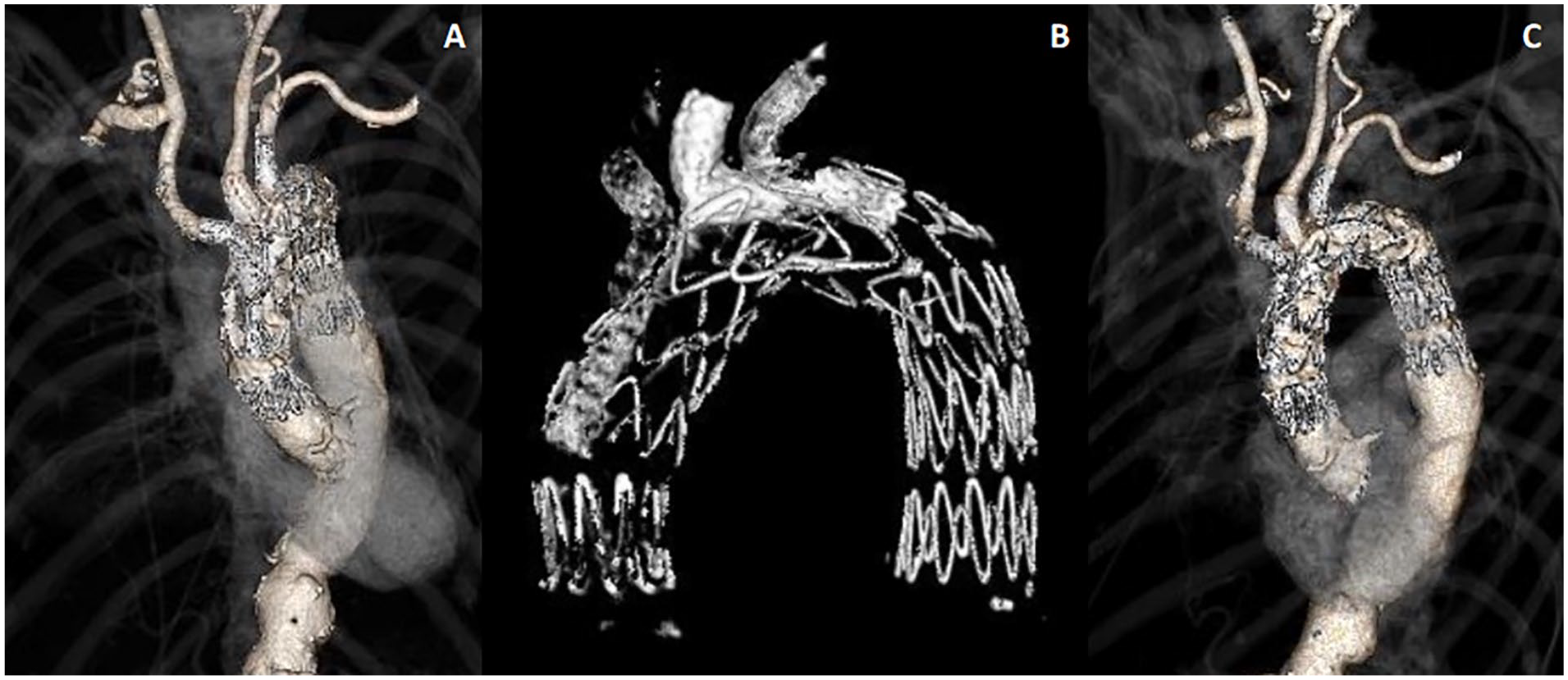
Postoperative CT scan. (A) Anterior view of 3D reconstruction, (B) 3D endograft reconstruction, and (C) lateral view of 3D reconstruction. CT, computed tomography.
Discussion
In this clinical case, we presented the adoption of sedo-analgesia to allow triple arch branch repair in high-risk patients, with contraindication to intubation due to severe compromise of pulmonary function. Since this first case, we have already treated 3 patients, 2 aortic rupture, and 1 elective procedure.
COPD represents a major risk factor for perioperative complications after general anesthesia and mechanical ventilation. 4 It has been demonstrated that patients affected by COPD who undergo general anesthesia frequently face complications during extubation, such as bronchospasm, wheezing, irritating cough, and depression of blood oxygen saturation. 5
These patients are also more prone to prolonged postoperative ventilation, re-intubation, and postoperative pulmonary infections, leading to an increased length of hospital stay and higher mortality. To overcome these problems local anesthesia and sedation have been proposed. Date showed a lower incidence of composite morbidity, pneumonia, prolonged ventilation, and re-intubation. 6
To the best of our knowledge, only single-branch arch repairs for the LSA under monitored anesthesia care have been previously reported, with successful results. 7
Traditionally, endovascular arch repair has been limited to high-risk patients, unfit for open surgery. Progressively, this procedure has become even more mini-invasive due to the adoption of percutaneous access, transaxillary branch-to-branch-to-branch carotid catheterization technique, 8 and total transfemoral approach.
The critical aspect of triple arch branch repair is represented by the need for precise deployment of the graft at the level of the ascending aorta, with a risk of migration due to high blood pressure generated by the heart. For this reason, it is crucial to be able to obtain respiratory arrest during angiography to precisely identify the proximal landing zone, distal to the coronary arteries ostia, and during graft deployment to prevent malpositioning.
To successfully perform a triple arch branch procedure under sedo-analgesia, it is mandatory teamwork between surgeons and anesthesiologists to keep the patient at a level of consciousness during graft deployment to be able to obtain respiratory arrest and to increase the sedation during the remaining part of the intervention to keep the patient still. The main challenge of sedo-analgesia is the careful control of the level of sedation to minimize the risk of respiratory depression and aspiration.
Choosing sedo-analgesia with spontaneous ventilation also has an impact on cardiac output reduction technique that can be applied. Of course, during sedation, not having control of ventilation, the Munich Valsalva Implantation Technique (MuVIT) cannot be implemented.9,10 Despite MuVIT being our standard choice, during the sedo-analgesia procedure, rapid right ventricle pacing was adopted.
Demonstrating the feasibility of triple arch branch repair under sedation represents the next step in minimizing the invasiveness of endovascular arch repair.
Conclusion
Triple arch branch repair under sedo-analgesia can be considered an effective technique in high-risk patients with severe compromise of pulmonary function, without the need for general anesthesia and intubation. In this clinical case, we illustrated the technique to further reduce the invasiveness of endovascular arch repair, underlining advantages, and limitations. The safety of the technique should be confirmed in future larger sample cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.