
Abstract
Objective:
The link between bovine aortic arch (BAA) and stroke after thoracic endovascular aortic repair (TEVAR) was investigated.
Methods:
The multicenter retrospective study included consecutive Stanford type B aortic dissection patients undergoing TEVAR from January 2019 to December 2023. A multivariable logistic regression was utilized to assess the correlation between BAA and early stroke, while a multivariable Cox regression was employed to evaluate the association between BAA and overall stroke. Kaplan-Meier curves were used to compare the freedom from overall stroke rates.
Results:
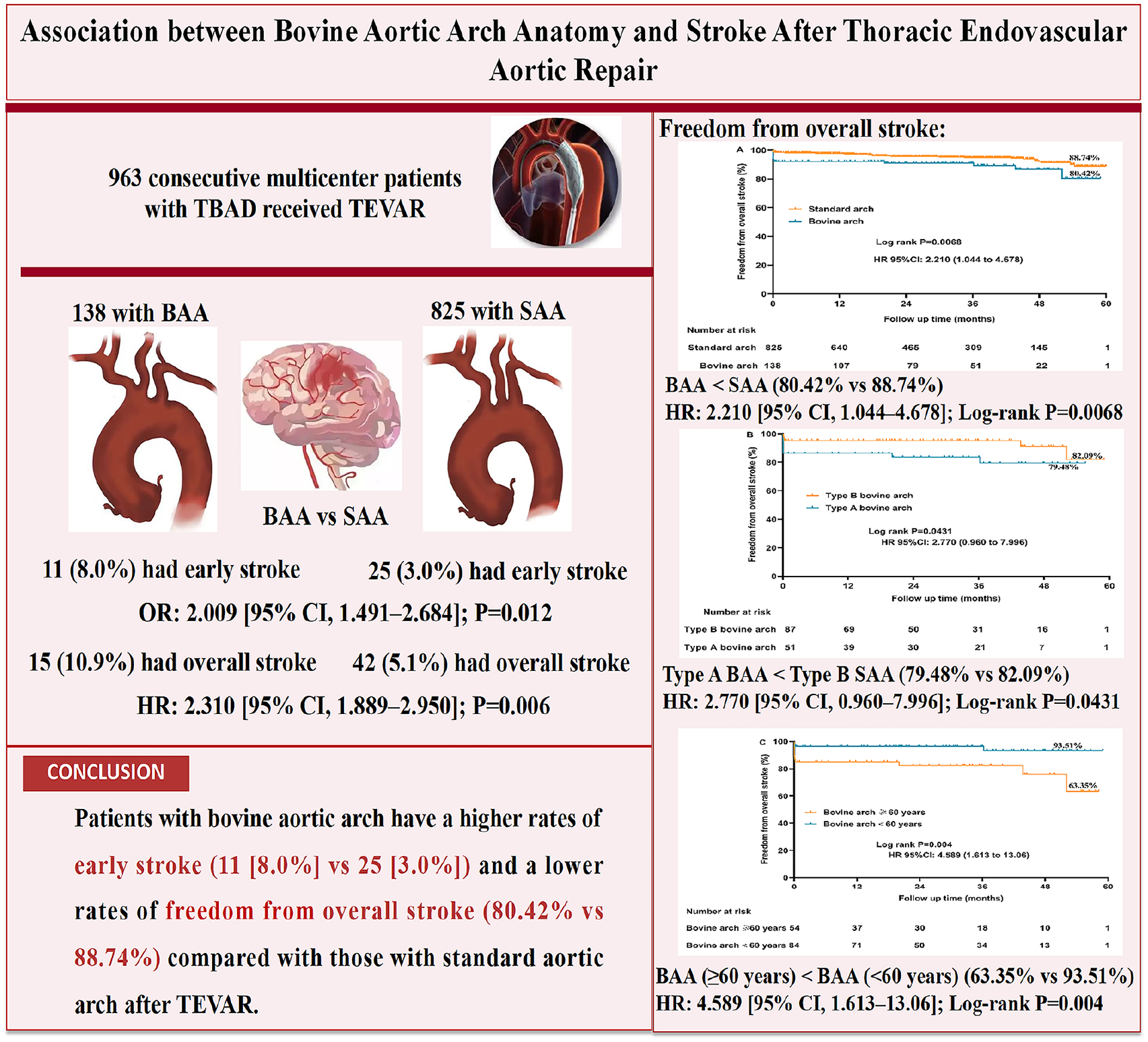
In total, 138 (14.3%) had a BAA and 825 (85.7%) had a standard aortic arch (SAA). Patients with a BAA showed a greater early stroke incidence (11 [8.0%] vs 25 [3.0%]; p=0.005). An independent association was found between BAA and early stroke (odds ratio, 2.009 [95% confidence interval (CI), 1.491-2.684]; p=0.012). During follow-up, a greater incidence of overall stroke was seen in patients with a BAA (15 [10.9%] vs 42 [5.1%]) (hazard ratio, 2.310 [95% CI, 1.889-2.950]; p=0.006). Moreover, the freedom from the overall stroke rate was notably lower in the BAA group (80.42% vs 88.74%) (log-rank p=0.0068). Furthermore, patients with type A BAA showed significantly lower freedom from overall stroke rates (79.48%) relative to those with type B BAA (82.09%) (log-rank p=0.0431), and the freedom from overall stroke rate for patients with BAA ≥60 years was markedly lower (63.35%) than that in those <60 years (93.51%) (log-rank p=0.004).
Conclusion:
BAA was correlated with an increased risk of early and overall stroke following TEVAR, particularly among older and type A BAA patients.
Clinical Impact
Individualized stroke prevention protocols and efficient neuroprotective measures should be developed for patients with BAA and adequate anticoagulation should be ensured to reduce the risk of embolism during TEVAR. This population should also ensure proper needle alignment. For instance, minimize the contact between the guide wire and the aortic arch wall. Temporal-occlusion of the carotid dynamic pulse during stent release might prevent solid fragments from entering into the craniocerebral artery. Additionally, thorough CO2 or saline flushing technique can be utilized for all the stentgrafts. Furthermore, distal cerebral embolic protection devices should be conducted in patients with a BAA during TEVAR
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.