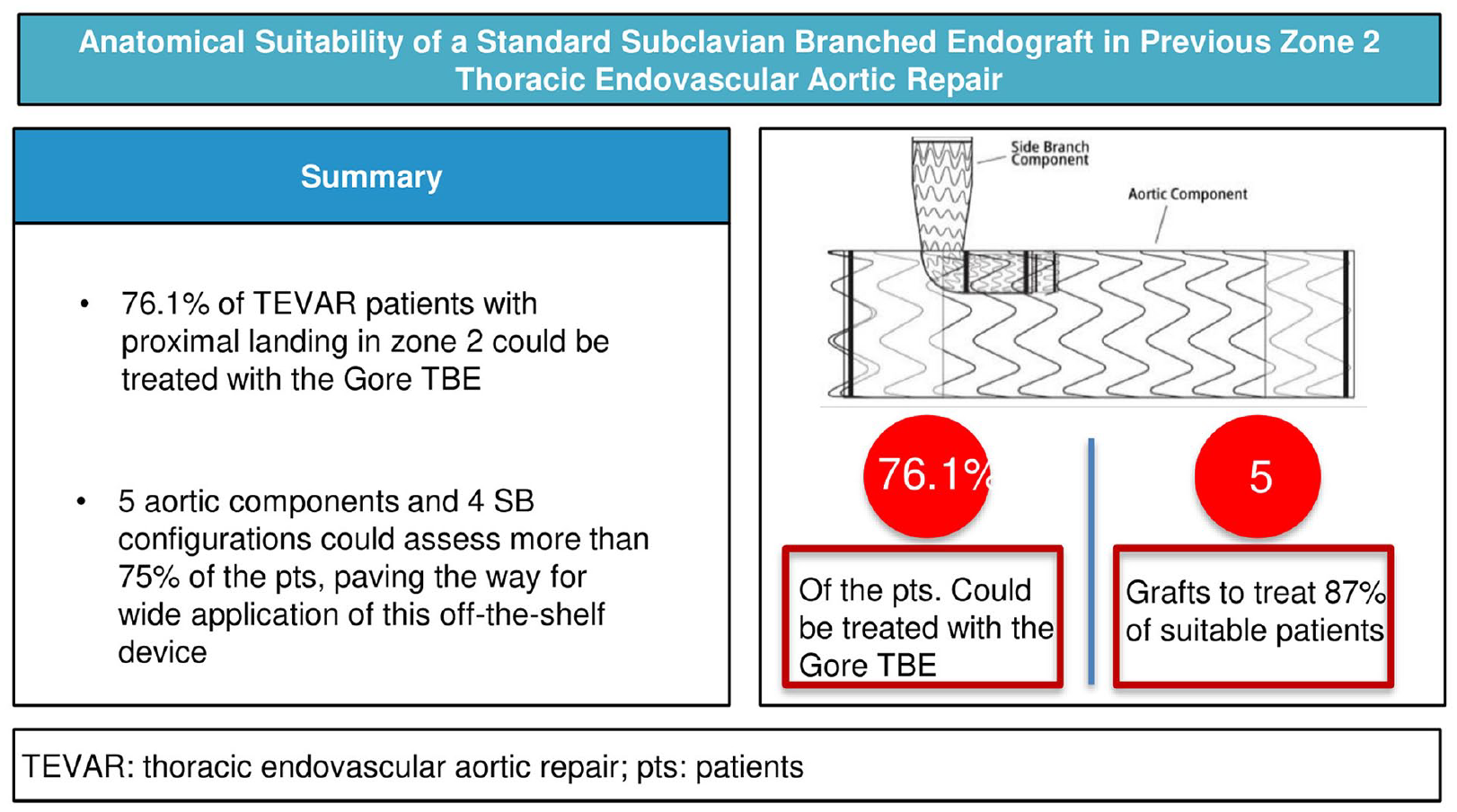
Purpose: To evaluate the anatomical suitability of the Gore Thoracic Branch Endoprosthesis in patients treated with thoracic endovascular aortic repair in landing zone 2. Materials and methods: A total of 517 cases were consecutively treated between 1999 and 2023, of which 102 were deployed in landing zone 2. A total of 92 patients were included in a single-center, retrospective, preclinical suitability study. The suitability for the investigational device was defined according to the manufacturer’s instructions for use. Extended suitability was also evaluated, including patients initially excluded for left subclavian artery measurements. Secondary outcomes were suitable and non-suitable patient comparisons, analysis of exclusion causes, and anatomical characteristics associated with suitability. A logistic regression model evaluated associations between baseline anatomical characteristics and non-suitability. Results: Seventy patients (76.1%) were suitable for implantation, which increased to 77 (83.6%) when analyzing extended suitability. Eighty-seven percent of suitable patients could have been treated with 5 aortic components, and 4 side branch configurations fitted 89.2% of suitable cases. A short prevertebral left subclavian artery length and a short proximal aortic landing zone were the most common causes of anatomical exclusion. The aortic landing zone diameter (odds ratio [OR]=0.83, 95% confidence interval [CI]=0.75–0.93, p=0.001) and length (OR=1.32, 95% CI=1.14–1.53, p<0.001) along with subclavian length (OR=1.18, 95% CI=1.07–1.31, p=0.001) were significantly associated with the odds of suitability. Conclusions: The Gore Thoracic Branch Endoprosthesis was anatomically suitable for more than 3 quarters of cases. A limited number of stent-graft configurations could fit the cohort in a remarkable number of patients, paving the way for wide application of this off-the-shelf device.
Clinical Impact
The present paper highlighted a significant feasibility rate for the Gore Thoracic Branch Endoprothesis among patients previously treated with TEVAR and proximal landing in zone. The limited number of stent-graft configurations that could have been implanted in a considerable portion of our cohort could help clinicians to develop a proper endovascular inventory related to this device, paving the way for its wide application.
DakeMDMillerDCSembaCP, et alTransluminal placement of endovascular stent-grafts for the treatment of descending thoracic aortic aneurysms. N Engl J Med. 1994;331(26):1729–1734.
2.
ErbelRAboyansVBoileauC, et al2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The task force for the diagnosis and treatment of aortic diseases of the European society of cardiology (ESC). Eur Heart J. 2014;35(41):2873–2926.
3.
RiambauVBöcklerDBrunkwallJ, et alEditor’s choice—management of descending thoracic aorta diseases: clinical practice guidelines of the European society for vascular surgery (ESVS). Eur J Vasc Endovasc Surg. 2017;53(1):4–52.
4.
MatsumuraJSLeeWAMitchellRS, et alThe society for vascular surgery practice guidelines: management of the left subclavian artery with thoracic endovascular aortic repair. J Vasc Surg. 2009;50(5):1155–1158.
5.
BradshawRJAhanchiSSPowellO, et alLeft subclavian artery revascularization in zone 2 thoracic endovascular aortic repair is associated with lower stroke risk across all aortic diseases. J Vasc Surg. 2017;65(5):1270–1279.
6.
BosiersMJDonasKPMangialardiN, et alEuropean multicenter registry for the performance of the chimney/snorkel technique in the treatment of aortic arch pathologic conditions. Ann Thorac Surg. 2016;101(6):2224–2230.
7.
TishSChaseJAScovilleC, et alA systematic review of contemporary outcomes from aortic arch in situ laser fenestration during thoracic endovascular aortic repair. Ann Vasc Surg. 2023;91:266–274.
8.
GennaiSCovicTLeoneN, et alChimney stenting versus surgical debranching for the treatment of aortic arch pathologies—a propensity-matched analysis. Ann Vasc Surg. 2023;89:200–209.
9.
TenorioEROderichGSKölbelT, et alMulticenter global early feasibility study to evaluate total endovascular arch repair using three-vessel inner branch stent-grafts for aneurysms and dissections. J Vasc Surg. 2021;74(4):1055–1065.e4.
10.
GeisbüschPKotelisDMüller-EschnerM, et alComplications after aortic arch hybrid repair. J Vasc Surg. 2011;53(4):935–941.
11.
VoigtSLBishawiMRanneyD, et alOutcomes of carotid-subclavian bypass performed in the setting of thoracic endovascular aortic repair. J Vasc Surg. 2019;69(3):701–709.
12.
PatelHJDakeMDBavariaJE, et alBranched endovascular therapy of the distal aortic arch: preliminary results of the feasibility multicenter trial of the gore thoracic branch endoprosthesis. Ann Thorac Surg. 2016;102(4):1190–1198.
13.
RoselliEEArkoFRThompsonMM, et alResults of the valiant Mona LSA early feasibility study for descending thoracic aneurysms. J Vasc Surg. 2015;62(6):1465–1471.e3.
14.
WangZGLiC.Single-branch endograft for treating Stanford type B aortic dissections with entry tears in proximity to the left subclavian artery. J Endovasc Ther. 2005;12(5):588–593.
15.
DakeMDFischbeinMPBavariaJE, et alEvaluation of the Gore TAG thoracic branch endoprosthesis in the treatment of proximal descending thoracic aortic aneurysms. J Vasc Surg. 2021;74(5):1483–1490.e2.
16.
DakeMDBrinkmanWTHanSM, et alOutcomes of endovascular repair of aortic aneurysms with the GORE thoracic branch endoprosthesis for left subclavian artery preservation. J Vasc Surg. 2022;76(5):1141–1149.e3.
17.
KooTKLiMY.A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163.
18.
CarkeetA.Exact parametric confidence intervals for Bland-Altman limits of agreement. Optom Vis Sci. 2015;92(3):e71–e80.
19.
LeoneNAndreoliFBartolottiLAM, et alAnatomical feasibility of a “semi-custom” unibody single-branch endograft in previous zone 2 thoracic endovascular aortic repair. Eur J Cardiothorac Surg. 2023;64(4):ezad290.
20.
BellamkondaKSYousefSNassiriN, et alTrends and outcomes of thoracic endovascular aortic repair with open concomitant cervical debranching. J Vasc Surg. 2021;73(4):1205–1212.e3.
21.
IserniaGSimonteGOrricoM, et alPreliminary results from an Italian national registry on the outcomes of the Najuta fenestrated aortic arch endograft. J Vasc Surg. 2023;77(5):1330–1338.e2.
22.
DeanAWanhainenAManiK, et alIn situ laser fenestrations of aortic endografts for emergent aortic disease. Ann Vasc Surg. 2023;93:329–337.
23.
GrimaMJWanhainenALindströmD.In situ laser fenestration technique: bench-testing of aortic endograft to guide clinical practice. J Endovasc Ther. 2024;31(1):126–131.
24.
LeoneNBartolottiLAMBaresiGF, et alAnatomical suitability for branched endovascular aortic arch repair and balloon-expandable bridging stent grafts in a cohort of patients previously treated with a hybrid approach. J Vasc Surg. 2024;79(2):198–206.e15.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.