
Abstract
Aim:
To present a case where the transapical and femoral accesses were used to establish a through-and-through guidewire to deliver branched arch endograft effectively.
Case:
An 86-year-old male presented with an aortic arch aneurysm rupture was treated with branched arch endograft. Due to tortuous anatomy, several attempts using femoral and axillary routes to navigate the endograft to the proximal landing zone failed. A through-and-through guidewire was established using transapical and femoral accesses to provide sufficient stability for subsequent advancement and delivery of the arch branch endograft.
Conclusion:
Transapical to femoral through-and-through approach is a feasible adjuvant for delivering aortic endografts in emergent cases, particularly in patients with trackability issues and challenging tortuous anatomy. This technique could be a valuable solution for carefully selected patients where conventional approaches are not viable.
Clinical Impact
Transapical access has been widely used in valvular and elective aortic interventions; however, its application in ruptured scenarios is seldom documented. This case report details the utilisation of transapical access in a ruptured aortic arch aneurysm with a tortuous aorta, where femoral and axillary access have proven inadequate. Establishing a transapical to transfemoral through-and-through wire has provided enhanced stability for precise endograft deployment. Procedural details and outcomes, alongside a review of the literature, underscore the use of transapical access and through-and-through wire in managing complex ruptured pathologies, addressing gaps in the literature concerning its efficacy and safety in urgent high-risk scenarios.
Introduction
According to the European Society for Vascular Surgery (ESVS) and European Association for Cardio-Thoracic Surgery (EACTS) guidelines, endovascular repair of the aortic arch is recommended in patients unfit for open surgery and with suitable anatomy. 1 Endovascular interventions have challenged open repair in recent years thanks to their improved morbidity and mortality rates, and relative feasibility in critically ill patients. 2
The through-and-through wire technique is a recent addition to the armamentarium of endovascular tools to enhance stability and accurate placement of stent grafts. This technique has proven its efficacy in the aortic endovascular treatment of challenging anatomical configurations, such as in severe tortuosity. 3
The application of the technique has extended beyond vascular surgery with remarkable success in transcatheter aortic valve replacement (TAVR) procedures. Physicians have used the transapical access to gain added precision in valve deployment, especially in emergent cases and tortuous anatomy, minimizing procedural complications and contributing to overall success. 4
We herein present a case of a ruptured aortic arch aneurysm treated using transapical to femoral through-and-through access to gain efficient stability for delivery and deployment of aortic branched endograft.
Case
We report on an 86-year-old male patient with a long history of vascular procedures in the past. Due to a ruptured infrarenal abdominal aortic aneurysm, the patient received an aorto-bi-iliac bypass 10 years ago. He then had a rapidly growing asymptomatic penetrating aortic ulcer at the proximal descending thoracic aorta that was treated using thoracic endovascular aortic repair (TEVAR) with proximal zone landing at Ishimaru zone 3. Several years later, a 4-vessel branched endovascular aneurysm repair (BEVAR) was employed for a Crawford type IV thoracoabdominal aortic aneurysm. Later during follow-up, the patient developed a type Ia endoleak regarding the TEVAR secondary to aortic enlargement. A left carotid–subclavian bypass was performed with TEVAR proximal extension to Ishimaru zone 2 and plugging the subclavian artery proximal to the takeoff of the vertebral artery.
The patient arrived at our emergency department after being transferred from another clinic, where they had been treated for pneumonia. The transfer was prompted by the new onset of recurrent paresis and an unexplained drop in hemoglobin levels. Due to a known anaphylactic reaction to iodine contrast medium, a computed tomography (CT scan had not been performed before the transfer. Upon arrival in our emergency room, the patient was administered 250 mg of cortisone and 8 mg of dimetindene before undergoing a CT angiogram. Given the patient’s history of aortic disease, an urgent computed tomography angiography (CTA) was performed. Computed tomography showed a contained rupture of a thoracic aneurysm due to a type IA endoleak.
Despite the advanced age and complex medical history, the intervention represented the only potential means of survival. The multidisciplinary team carefully considered the risks and benefits, acknowledging the ethical challenges present in treating a high-risk multimorbid patient. The decision to proceed with treatment was made in light of the patient’s life-threatening condition, with no viable alternatives to address the aortic rupture. The patient and their family were informed of the risks and consented to the procedure.
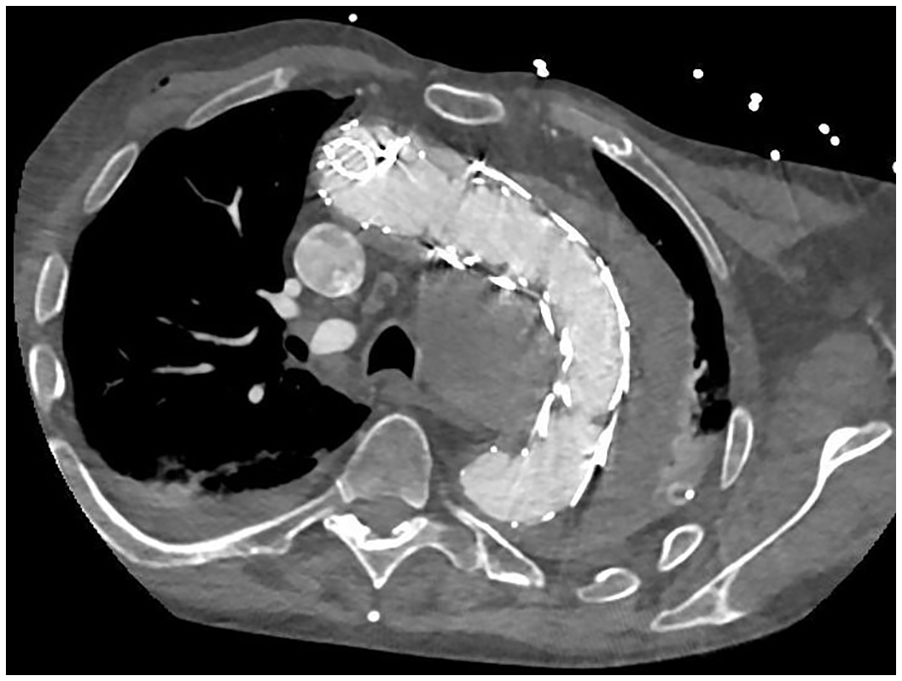
The patient’s anatomic parameters were analyzed using a dedicated 3D workstation (Tera Recon Aquarius, San Mateo, Cali). Figure 1 shows the preoperative images of the patient. A custom-made device (CMD) from Cook Medical (Bloomington, IN, USA) was utilized for endovascular repair. It was originally designed for other personnel but was found compatible with the anatomical parameters of the patient. The device design involved 2 antegrade branches and one retrograde inner branch for the innominate (IA), left common carotid (LCC), and left subclavian arteries (LSA), respectively.
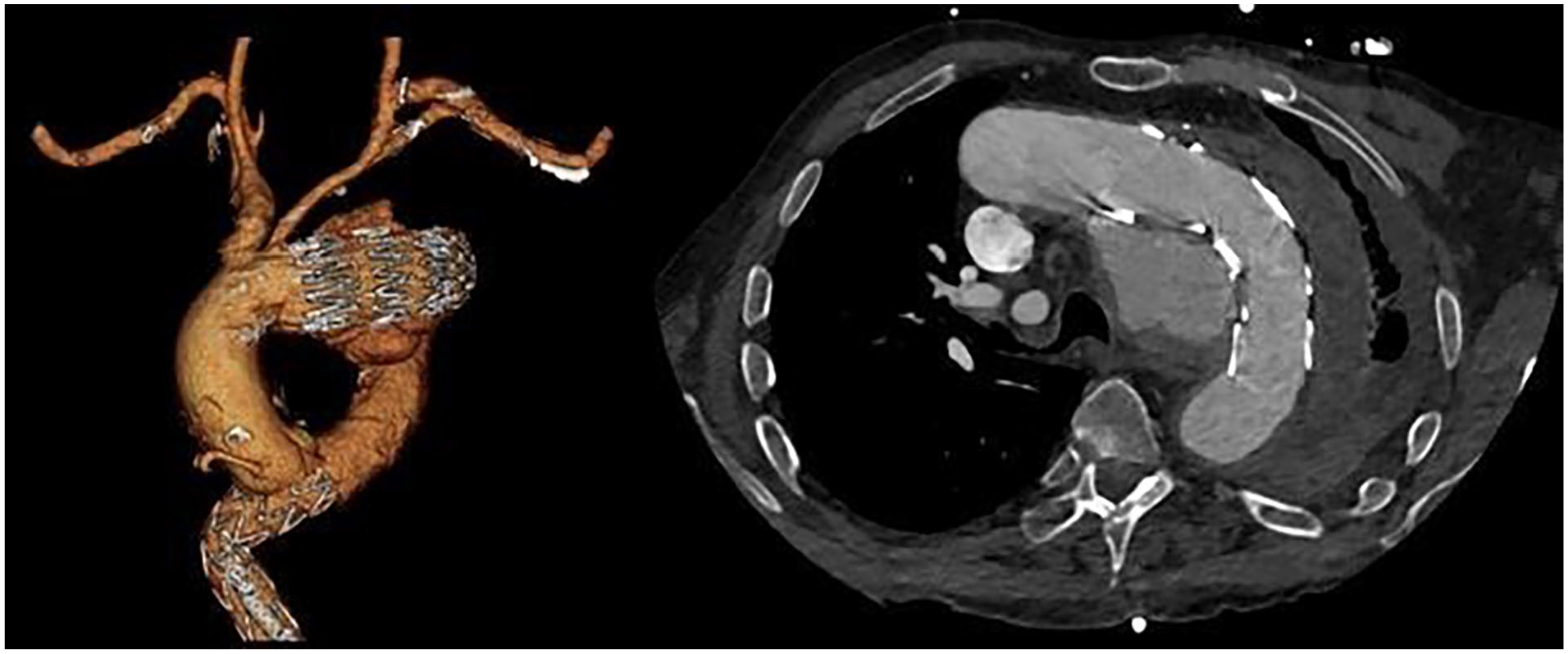
Preoperative images showing endoleak type Ia, aortic rupture, and left hemothorax.
The procedure was performed in a hybrid operating theater with a fixed imaging system under general anesthesia. Bilateral ultrasound-guided percutaneous femoral accesses were undertaken. Right axillary artery cutdown was performed to establish the through-and-through guide wire for the delivery of the aortic endograft and the IA bridging stent. Additionally, the left brachial access was percutaneously punctured using ultrasonography for delivery of the LCC bridging stent over the carotid–subclavian bypass, LSA plug inspection, and excluding type II endoleak.
Due to the severely tortuous anatomy of the thoracic aorta with double kinks, attempts of endograft advancement using transfemoral access alone into the aortic arch failed (Figure 2). Axillary access was utilized to snare transfemoral wire to establish an axillo-femoral through-and-through guidewire to gain added stability. However, subsequent trials failed, and an alternative solution had to be sought. The decision was made to establish a through-and-through wire via transapical access for maximum possible stability. A left-sided mini-thoracotomy at the left fourth intercostal space was performed by a cardiothoracic surgeon. Two 3-0 Prolene sutures with felt pledgets were placed, and a 55 cm long 7F COOK Flexor sheath (Bloomington, IN, USA) was inserted into the left ventricle. A 400 cm hydrophilic Terumo wire (Terumo Interventional Systems, Somerset, New Jersey) with an En snare device (Merit Medical System, South Jordan, UT, USA) was then snared in the proximal descending thoracic aorta. We utilized the push-and-pull technique to position the endograft, which facilitates advancement through kinked anatomy. In this method, the through-and-through wire was alternately loosened and then pulled at the proximal end, allowing the endoprosthesis to be guided through the aorta. By doing so, the wire not only adds stability but also enables the endograft to be pulled through the aorta. (Figure 3). Cardiac output was reduced using the MuVIT technique. 5 A Supplementary video is provided to show the transapical access through the mini-thoracotomy incision.
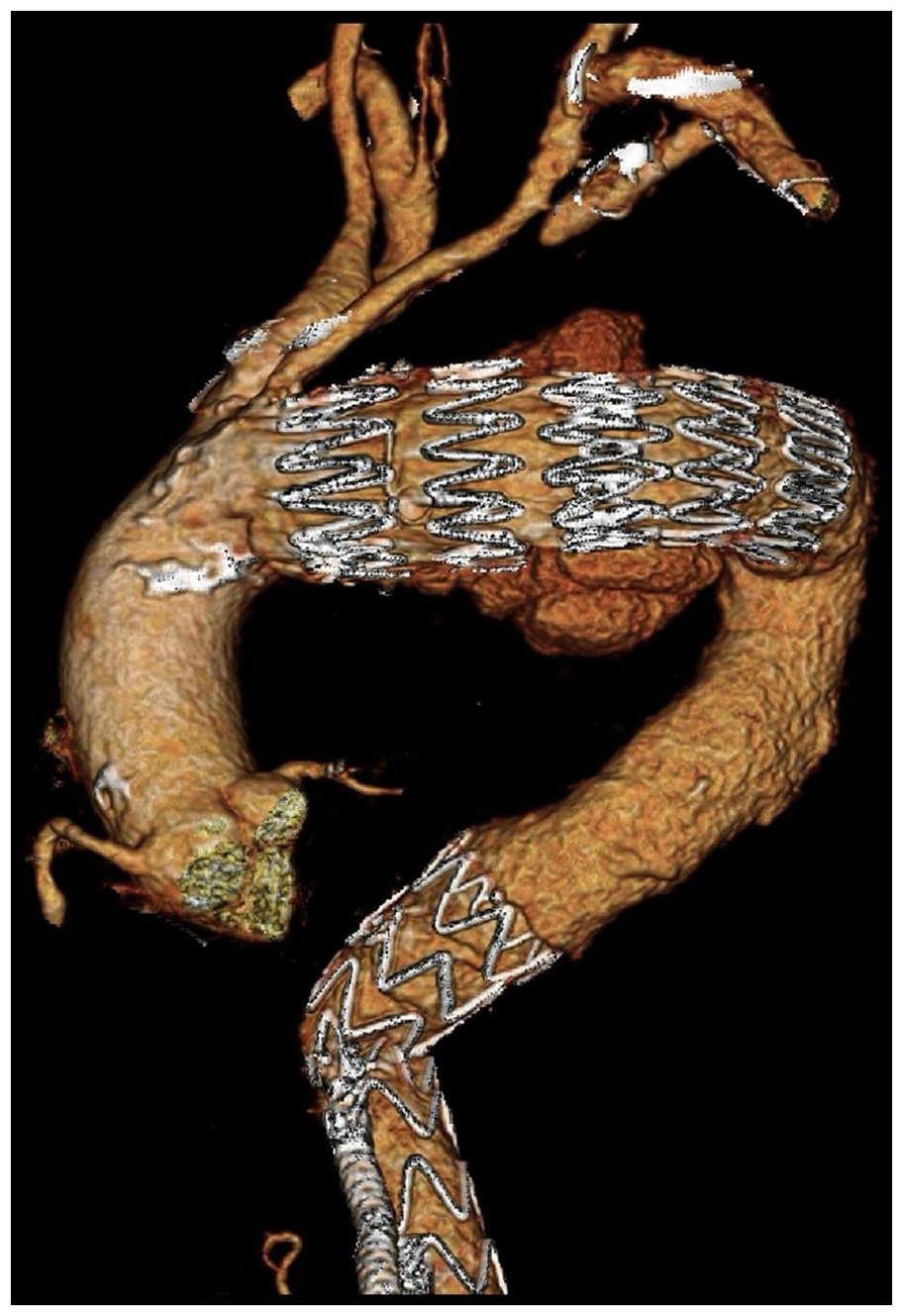
Double tortuous kinks of the thoracic aorta.
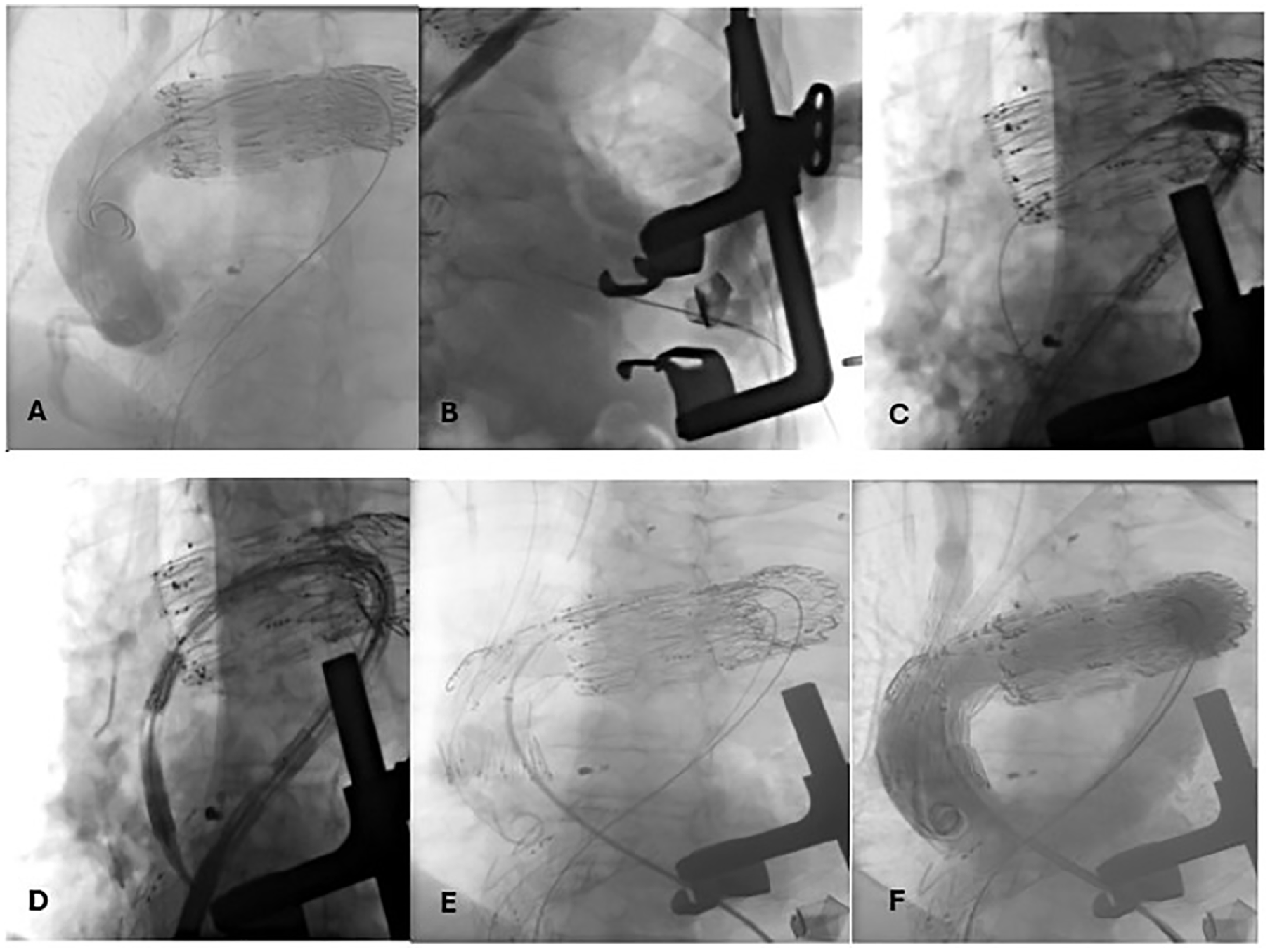
Intraoperative images. (A) Transfemoral guidewire, (B) Mini-thoracotomy of the left side of the chest and LV puncture with guidewire advancement, (C) Establishment of through-and-through guidewire, (D) Introduction of the CMD into Ishimaru zone 0, (E) Deployment of the 3 branched CMD, (F) Completion angiography at the end of the procedure denoting sealing of the pathology, perfusion of supra-aortic vessels, and absence of endoleak.
Connection of supra-aortic vessels via bridging stents was then performed. The right axillary access was used to bridge stent the IA to the first inner branch. The LCCA was cannulated using the left brachial access, and consequently, 2 Begraft plus stents (Bentley InnoMed, Hechingen, Germany) were used as bridging stents for the second inner branch. The retrograde branch designated for the left subclavian artery (LSA) was extended using a 10x57 mm Begraft stent (Bentley InnoMed, Hechingen, Germany) to gain additional length. Subsequently, the branch was occluded using a 12 mm Amplatzer Plug (Abbott Vascular, CA, USA), delivered via the transfemoral route. The branched endograft was extended with a COOK ZTA P 34/161(Bloomington, IN, USA) to achieve distal sealing. Control angiography showed a sealed aneurysm, adequate perfusion of supra-aortic vessels, and no sign of endoleak. (Figure 4).
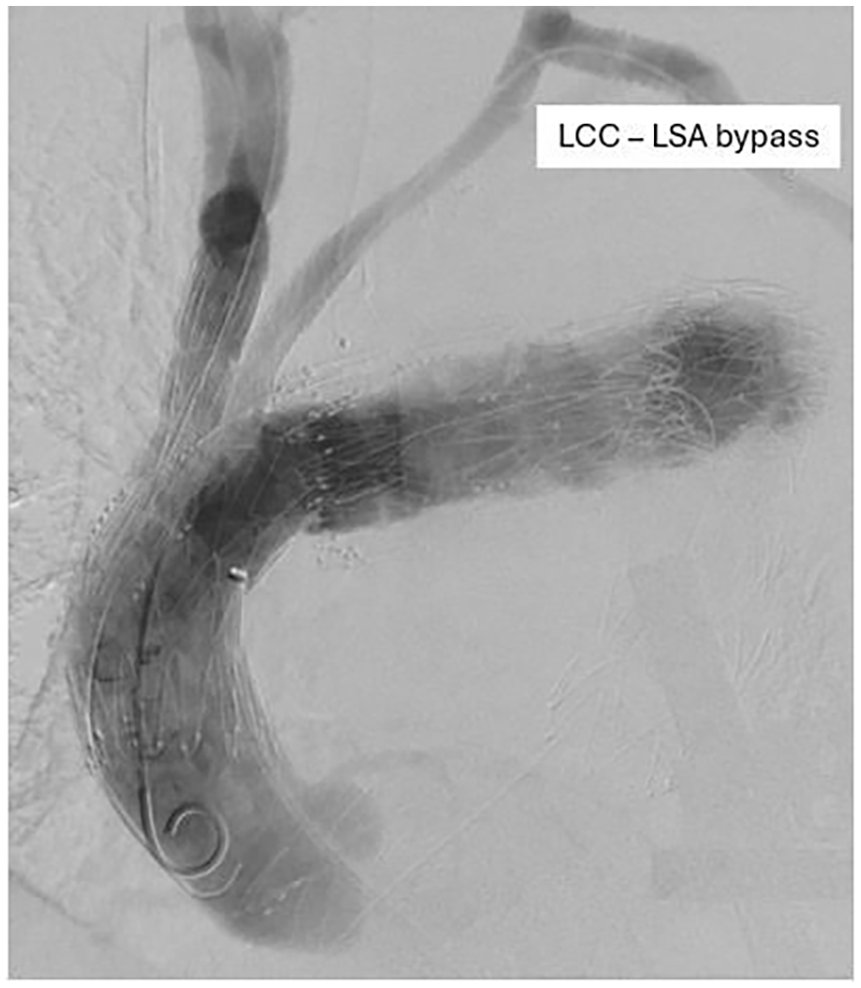
Intraoperative angiography. Aortic rupture sealed, no endoleaks, and adequate supra-aortic vessels’ perfusion.
The left-sided hemothorax was drained by a chest tube. The left brachial artery was surgically exposed and closed with interrupted prolene sutures. The right axillary artery had focal dissection and required localized endarterectomy with bovine pericardial patch closure. Both femoral accesses were sealed using the suture-mediated closure device Perclose ProGlide system (Abbott Vascular, CA, USA).
The patient stayed in the intensive care unit for 5 days before being transferred to the ward under uneventful stable conditions. Postoperative CTA demonstrated the absence of endoleak, complete sealing of the pathology, and maintained patency of the supra-aortic bridging stents (Figure 5). The patient then had a complicated course where the hemothorax eventually required surgical thoracoscopic evacuation. Due to secondary empyema, open surgery was required. Following that, the patient went into respiratory insufficiency and required tracheotomy and prolonged ventilation. The family decided to withdraw care due to the patient’s age and respecting his preoperative wishes.
Postoperative CTA shows the absence of endoleak, sealing of pathology, and patency of supra-aortic bridging stents.
Discussion
Nearly a third of patients with ruptured aortic arch aneurysms can make it safely to the hospital where only half of them may eventually survive. The main contributing factor is the absence of symptoms and the incidental discovery of pathology.1,6–11 Mortality rates have reached nearly 50 and 75% for those who have arrived at the hospital after aortic rupture within 6 and 24 hours, respectively.8,9
According to the ESVS and EACTS guidelines, endovascular aortic arch repair is advised only for patients who are unsuitable for open surgery and possess appropriate anatomical characteristics. In recent years, open surgical repair has faced challenges from endovascular interventions due to their enhanced rates of morbidity and mortality, as well as their relative feasibility for critically ill patients.1,2,10,11
The use of femoral access has been the standard way of deploying an aortic endograft. In the current case, the tortuous course of the thoracic aorta rendered all transfemoral attempts to fail. Given the anatomical challenges, a through-and-through wire was employed to enhance procedural stability and facilitate the advancement of the endograft. 3 This was employed using the right axillary artery for ergonomic reasons by open surgical means. However, further trials of endograft advancement were not successful.
The transapical access was utilized to establish a through-and-through wire, providing the necessary stability to overcome severe aortic tortuosity. This approach, though well-established in valve implantation, 4 is less commonly reported in managing ruptured aortic arch aneurysms, particularly in emergent scenarios. The potential risks of inducing ventricular tachycardia and dropping blood pressure have been discussed and studied. Some physicians have used the phenomenon as a means of cardiac output reduction for secure deployment of the valves. Nevertheless, the majority of these tachycardic episodes are temporary and usually resolve in a few minutes.12,13 Ahmad et al, 14 have reported on the use of transapical access to deploy an aortic endograft for an ascending aortic saccular aneurysm in a heart transplant patient. The postoperative period was uneventful, and the patient showed satisfactory remodeling during follow-up that reached 12 months. Similarly, another group has treated an ascending aortic pseudoaneurysm with the use of transapical and transfemoral accesses to establish a through-and-through wire. The graft was introduced through the femoral artery and rapid ventricular pacing was used to reduce the cardiac output for safe deployment of the endograft. The patient had no adverse events during the follow-up of 6 months. 15 In our case, the use of transapical access helped us achieve a through-and-through wire that enabled us to achieve more stability. We had not experienced any ventricular tachycardia.
The use of transapical access for treating ruptured aortic pathologies is relatively under-reported in the literature. The following Table 1 summarizes the existing reports, detailing indications and complications for such emergent procedures. While most studies have established transapical access as a feasible technique with high technical success, the emergent application of transapical access in a ruptured aortic arch aneurysm, as presented in this case, is rarely documented.
Summary of Literature on the Use of Transapical Access in Treating Ruptured and Contained Ruptured Aortic Pathologies, Including Indications and Complications.
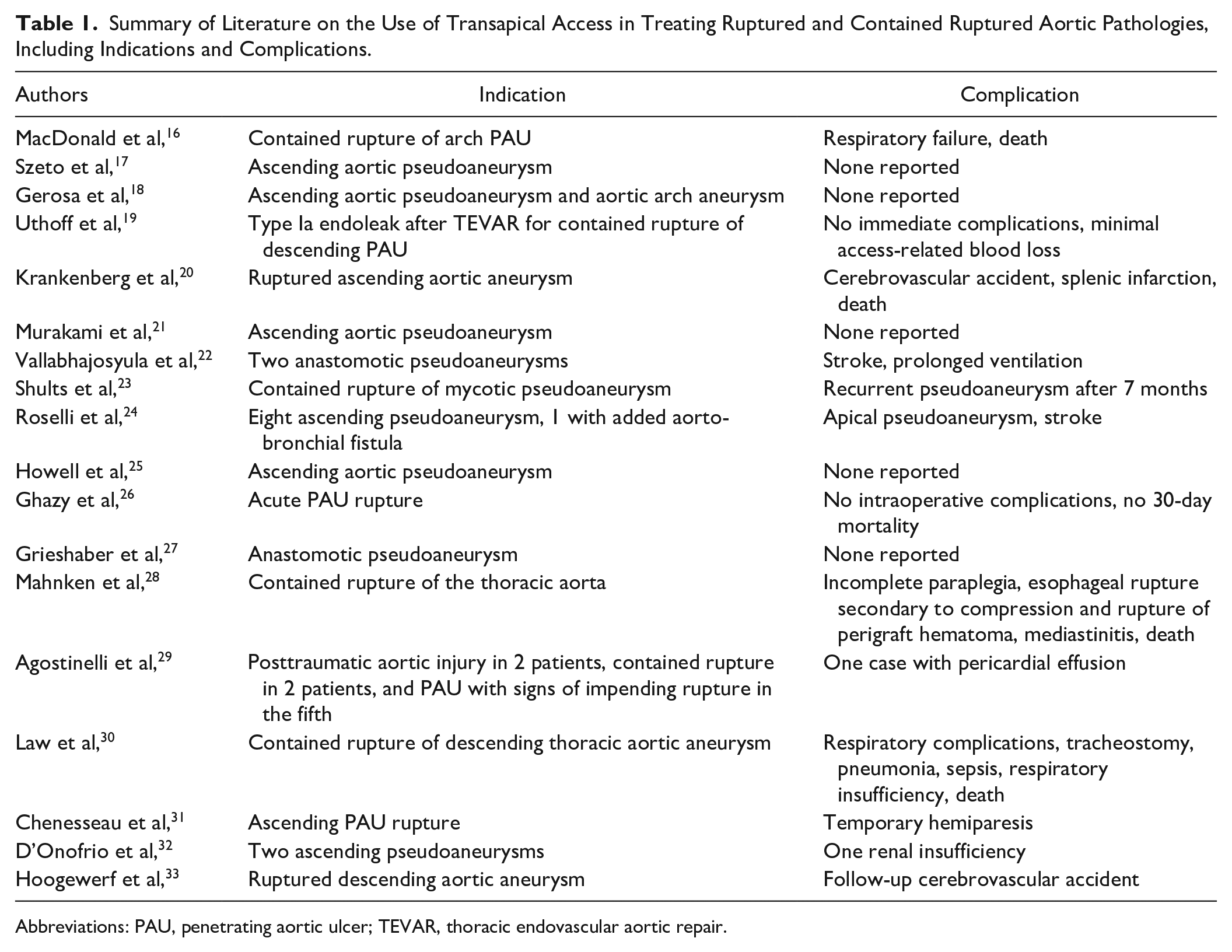
Abbreviations: PAU, penetrating aortic ulcer; TEVAR, thoracic endovascular aortic repair.
The transapical technique in endovascular aortic repair provides precise positioning of stent grafts, improved access to complex anatomies, and reduced complications arch as in chimney repairs. Employing a transapical through-and-through (TT) wire allows the main graft body to pass centrally within the aorta, lowering the risk of embolization and damage to arch plaques. Additionally, it helps prevent delivery system conflicts and avoids kinking or occlusion of bridging stents. Nevertheless, the approach is invasive and presents challenges with cerebral protection. 34
The treatment of this 86-year-old patient with significant comorbidities and a ruptured aortic arch aneurysm presented profound ethical challenges. The decision to proceed with the intervention was guided by the principles of beneficence and non-maleficence, which necessitate a careful balance between the potential benefits and risks of treatment. Given the patient’s life-threatening condition and the absence of alternative treatment options, a multidisciplinary team of vascular surgeons, cardiothoracic surgeons, and anesthesiologists deliberated extensively on the case. Ultimately, the intervention was considered the only viable option to address the ruptured aneurysm, which posed an imminent threat to the patient’s survival. The patient and their family were thoroughly informed about the risks, including the high likelihood of complications and the limited probability of long-term survival. With this understanding, they provided consent for the procedure, aligning the decision-making process with the ethical principle of respect for autonomy.
While the emergent nature of the condition justified the intervention, this case also underscores broader ethical dilemmas in vascular surgery, particularly concerning resource utilization and quality-of-life considerations in high-risk, elderly patients. These decisions require a nuanced and case-specific approach, balancing the urgency of life-saving interventions against the anticipated outcomes and patient preferences.
Transapical access offers an alternative method to enhance stability for the delivery of aortic endografts, particularly in emergent cases where conventional approaches are inadequate. It is a feasible and readily available technique that expands the armamentarium of endovascular options for treating complex aortic pathologies. In this case, the transapical-to-femoral through-and-through wire technique demonstrated remarkable efficiency in addressing severe aortic tortuosity during emergent aortic arch repair. Furthermore, the use of a custom-made device originally designed for another patient highlights the adaptability required in high-risk vascular emergencies. By detailing procedural nuances and outcomes, this report provides valuable insights for managing similar cases and bridges gaps in the literature regarding the emergent application of transapical access and establishment of through-and-through wire in ruptured aortic pathologies.
Conclusion
Transapical to femoral through-and-through approach is a feasible adjuvant for delivering aortic endografts in emergent cases, particularly in patients with trackability issues and challenging tortuous anatomy. This technique could be a valuable solution for carefully selected patients where conventional approaches are not viable.
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors have no conflict of interest. NT is a proctor for and receives an institutional grant from Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Consent was obtained from the patient and family members for the use of data for publication.
Ethical Committee Approval
Ethical committee approval was not required as this is a single case report.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.