
Abstract
Purpose:
This is a prospective study to investigate the clinical outcomes of using noncompliant balloons in lower limb angioplasty for chronic limb threatening ischemia (CLTI).
Materials and Methods:
This is a prospective single-center cohort study performed at a local tertiary hospital in Singapore. Consecutive patients who underwent lower limb angioplasty for CLTI using a noncompliant balloon catheter were enrolled if they were aged 40 years and above, presented with CLTI Rutherford grade 4 to 6, and had TASC C or D lesions in the lower limb vessels that were at least 100mm in length. Patient demographics, Rutherford grading, lesion characteristics, complications, and follow-up data were collected and analyzed. The primary outcomes were 30-day freedom from major adverse events, amputation-free survival (AFS) at 12 months, and freedom from clinically driven target lesion revascularization (cdTLR) at 12 months. Secondary outcomes included clinical success and target lesion primary patency (TLPP) at 12 months. Amputation-free survival, freedom from cdTLR, and TLPP were calculated by Kaplan-Meier analysis.
Results:
From May 2020 to December 2021, 50 patients (50 limbs) were enrolled. 43 (86%) patients had diabetes mellitus, while 12 patients (24%) had end-stage renal failure. 85 lesions were treated, including 59 (69.4%) below-the-knee (BTK) lesions. All the lesions were TASC C (n=45, 52.9%) or TASC D (n=40, 47.1%) lesions. Mean lesion length was 231.4±116.2mm. Technical success rate was 96.5%. No patients were lost to follow-up. Median follow-up duration was 282 days (IQR: 31-390 days). One patient died on day 26 due to an acute myocardial infarction. Two patients had groin hematomas postprocedure, both of which were treated conservatively. AFS, freedom from cdTLR, and TLPP at 12 months postprocedure was 70.0% (95% confidence interval [CI]: 58.4%-83.9%), 90.1% (95% CI: 83.4%-97.4%), and 61.1% (95% CI: 50.7%-73.6%), respectively.
Conclusion:
Early results have shown that the use of a high-pressure, noncompliant balloon is effective in lower limb angioplasty for CLTI in a highly challenging group of patients with a high prevalence of long BTK disease. Good vessel patency and limb salvage rates can be achieved, with a low complication rate. We await more long-term outcomes on vessel patency.
Clinical Impact
There are many devices in the market for use in lower limb angioplasty. However, many of them come with an increased financial cost, procedural time and procedural difficulty. We report our prospective results with the exclusive use of a high pressure, non-compliant balloon, in a challening group of patients with a high prevalence of diabetes and end stage renal failure, achieving amputation free surival at 6 and 12 months post-procedure of 84.0% and 70.0% respectively. The use of non-compliant balloon is technically easy and does not add additional steps compared to a standard POBA procedure, thus limiting costs. We believe this article can be a push factor for clinicians to consider the use of these high pressure, non-compliant balloons in their patient care.
Keywords
Introduction
Noncompliant balloons are now widely used in coronary angioplasty for vessel preparation and also for restenosis.1,2 Promising results have been noted particularly in rigid and calcified lesions. 3
To date, many studies have reported the use of semi-compliant balloons for lower limb angioplasty in chronic limb threatening ischemia (CLTI). However, results have been varying and particularly poor in below-the-knee (BTK) lesions. BTK lesions tend to be long and severely calcified, and angioplasty is often associated with significant recoil as well as poor patency.4,5 Calcifications along the vessel wall may also limit their expansion and luminal gain when semi-compliant balloons are used. The addition of paclitaxel drug eluting balloons in the BTK segment is often associated with the no-flow phenomenon on angioplasty, and has not shown promising results, likely due to impaired drug absorption. 5
In our clinical practice involving lower limb CLTI patients, we note a high proportion of patients with highly calcified vessels. In addition, our patient population with a high proportion of diabetics 6 present with mostly highly calcified BTK disease,7,8 and have small vessels similar in size to coronary vessels. On the basis of this, we set out to prospectively investigate the clinical outcomes of using noncompliant balloons in our patients undergoing lower limb angioplasty for CLTI with significant angiographic lesions.
Materials and Methods
This is a prospective single-center cohort study performed at a local tertiary hospital in Singapore. Fifty consecutive patients who underwent lower limb angioplasty for CLTI using the JadeTM (OrbusNeich, Hong Kong) noncompliant balloon catheter were enrolled in this study. Patients were included if they were aged 40 years and above, presented with CLTI Rutherford grade 4 to 6, and had TASC C or D lesions in the superficial femoral artery, popliteal artery, or tibial arteries that were at least 100mm in length on initial angiography and suitable for endovascular intervention. Patients were excluded if they had a recent myocardial infarction in the last 30 days, had projected life expectancy of less than a year, had previous ipsilateral lower limb bypass surgery, previous stents in the target lesions, or if they required thrombectomy or atherectomy devices during the procedures.
The study was conducted in accordance with good clinical practice standards and the ethical principles of the Declaration of Helsinki and its amendments. Written informed consent both for the study and the procedure was obtained from each patient according to institutional protocol. The study was reviewed and ethics approval was given by the hospital’s institutional review board.
Data Collection
Data were collected prospectively using a template based off the Vascular Quality Initiative data 9 collection template. Preoperative data collected include patient demographics, Rutherford grading, 10 lesion severity as well as WIfI Score. 11 Intraoperative data include lesion specific details such as TASC II classification, 12 lesion length, degree of stenosis, as well as calcification scores.
Procedure
An ultrasound Duplex scan of the lower limb arteries was obtained prior to all interventions. The native vessel diameters were also measured on ultrasound. The findings of the duplex ultrasound were used to enroll these patients for our study, prior to their procedure. All patients were also assessed by the anesthetist for pre-operative optimization. Routine pre-operative investigations including a complete blood count, renal function tests, as well as an electrocardiogram was performed prior to any procedure. Further cardiology testing was done at the discretion of the anesthetists.
All lower limb angioplasty procedures were performed by senior vascular surgeons in a hybrid operating theater (Artis Zeego, Siemens) at a local tertiary hospital. The procedure was done under general, regional, or local anesthesia as per the anesthetist’s discretion in conjunction with patient preference. Intravenous antibiotics were given at induction.
In the absence of significant iliac disease on Duplex ultrasound, antegrade ultrasound guided common femoral access with a 11-cm 5Fr BRITE TIP sheath (Cordis, Santa Clara, USA) was used for initial access. A complete infra-inguinal angiogram was performed using either VisipaqueTM contrast (GE Healthcare, Chicago, USA) or Carbon dioxide, depending on the patient’s renal function. Systemic anticoagulation with intravenous heparin 3000-5000 IU was given depending on weight. Lesions were crossed using a 0.035 Glidewire (Terumo Corporation, Tokyo, Japan) or v18 wire (Boston Scientific, Marlborough, USA). Intraluminal crossing was preferred at all times, and retrograde crossing with an ultrasound guided puncture of the distal target artery used as necessary to ensure intraluminal crossing.
Balloon angioplasty was performed for both supra and infra popliteal lesions, and balloon sizes were chosen using a 1:1 diameter ratio, based on the pre-operative vessel sizing on Duplex ultrasound. The JadeTM noncompliant balloon (OrbusNeich, Hong Kong) was exclusively used for all lesions. No predilation was performed unless there was difficulty in tracking the intended balloon through the lesions. If predilation was required, this was performed using a 2 × 40-mm noncompliant balloon. Treatment balloons were inflated to the nominal pressure, or the minimum pressure required to efface all lesions, whichever was lower. Each balloon inflation was held for 120 seconds. Repeated prolonged inflation for 3 minutes was done if there was significant recoil, or vessel dissection. No drug-eluting balloons, stents, or debulking devices were used.
Concomitant minor below ankle or wound debridement procedures were performed in the same setting as necessary. All patients were put on single antiplatelet therapy (Aspirin 100mg daily or Clopidogrel 75mg daily) postprocedure, and concomitant anticoagulation or a second antiplatelet agent if advised by the cardiologist for their cardiac conditions.
Follow-Up Strategy
All patients were followed up at 1, 3, 6, and 12 months postprocedure. Follow-up was done in-person at our specialist outpatient clinic. Patients who did not turn up for their scheduled appointments were contacted via a phone call. At each follow-up, a clinical assessment was performed in conjunction with a wound evaluation if applicable. A Duplex Ultrasound was also performed at the 6-month and 12-month visit to evaluate the patency of the treated vessels.
Outcomes
The primary outcomes were freedom from major adverse events, amputation-free survival (AFS) at 12 months, and freedom from clinically driven target lesion revascularization (cdTLR) at 12 months. Secondary outcomes included clinical success and target lesion primary patency (TLPP) at 12 months.
Definitions
Technical success was defined as the ability to cross and dilate the lesion and achieve residual angiographic stenosis no greater than 30%. Freedom from major adverse events was defined as a composite of freedom from device- and procedure-related mortality through 30 days postprocedure. Major amputation is defined as any above ankle amputation. Freedom from cdTLR at 12-month follow-up was defined as a repeat intervention to maintain or re-establish patency within the region of the treated arterial vessel plus 5-mm proximal and distal to the treated lesion edge at the respective time points. Clinical success at follow-up was defined as an improvement of Rutherford classification at all follow- up time points of one class or more as compared with the pre-procedure Rutherford classification. TLPP at 6- and 12-month follow-up was defined as absence of a hemodynamically significant stenosis on Duplex ultrasound (systolic velocity ratio no greater than 2.5) at the target lesion and without TLR within the time of procedure and the given follow-up. Any patient where duplex ultrasound is not analyzable at index and/or at follow-up, where there is documented significant progression of disease above the target lesion, or who had undergone a major amputation prior to the time of follow-up will be excluded from the calculation of this endpoint.
Statistical Analysis
Baseline variables were summarized with the use of descriptive statistics. Continuous variables were reported as the mean and standard deviation, or median and range, as appropriate, and categorical variables as absolute number and percent. AFS, freedom from cdTLR, and TLPP were calculated by Kaplan-Meier analysis. All analyses were performed in R version 4.0.4. 13
Results
Patient Demographics
50 patients (50 limbs) were enrolled from May 2020 to December 2021. There were 36 (72%) male patients and 14 (28%) female patients, with a mean age of 66.2±11.2 years. 33 patients (66.0%) were Chinese, and 10 patients (20.0%) were Malay. 43 (86%) patients had diabetes mellitus, while 12 patients (24%) had end-stage renal failure. All patients had chronic limb threatening ischemia with the majority (78%, n=39) having Rutherford score 5 (Table 1). The mean WIfI score was 3.86±1.91. No patients were lost to follow-up. The median follow-up duration was 282 days (interquartile range: 31-390 days).
Baseline and Perioperative Details.
Abbreviations: BMI, body mass index; ESRF, end-stage renal failure.
Procedure and Lesions
40 (80%) patients had their procedures done with general anesthesia, 8 patients (16%) had regional anesthesia, while 2 patients (4%) had their procedure done under local anesthesia. A total of 50 limbs were treated, with a total of 85 lesions. 59 lesions (69.4%) were BTK lesions. All the lesions were TASC C (n=45, 52.9%) or TASC D (n=40, 47.1%) lesions. The mean lesion length was 231.4± 116.2mm. Most lesions (n=72, 84.7%) were de novo lesions. 30 lesions (37.2%) were moderately-to-severely calcified. The anterior tibial artery was the most commonly treated vessel (n=25, 29.4%). Technical success of treatment was 96.5% (82/85 lesions). All patients had successful wire crossings and balloon crossing of the intended treatment vessels. However, 1 lesion had severe residual stenosis post Plain Balloon Angioplasty (POBA) while 2 lesions had severe recoil leading to lesion re-occlusion despite prolonged angioplasty. No patients required bailout stenting. Details of the lesions are shown in Table 2.
Lesion Characteristics.
Abbreviations: SFA, Superficial Femoral Artery; ATA, anterior tibial artery; PTA, posterior tibial artery; TP, Tibio-Peroneal.
Primary Outcomes
30 day Major Adverse Events: One patient died on day 26 due to an acute myocardial infarction. Two patients had groin hematomas postprocedure, both of which were treated conservatively. There were no vessel ruptures, perforations, large flow-limiting dissections, or distal embolization peri-procedurally.
AFS: AFS at 6 and 12 months postprocedure was 84.0% (95% confidence interval [CI]: 74.4%-94.8%) and 70.0% (95% CI: 58.4%-83.9%), respectively (Figure 1A). In total, 7 patients underwent a major amputation within 12 months postprocedure, and the average time to major amputation was 161.7±112.5 days. 8 patients died within 12 months postprocedure from unrelated causes.
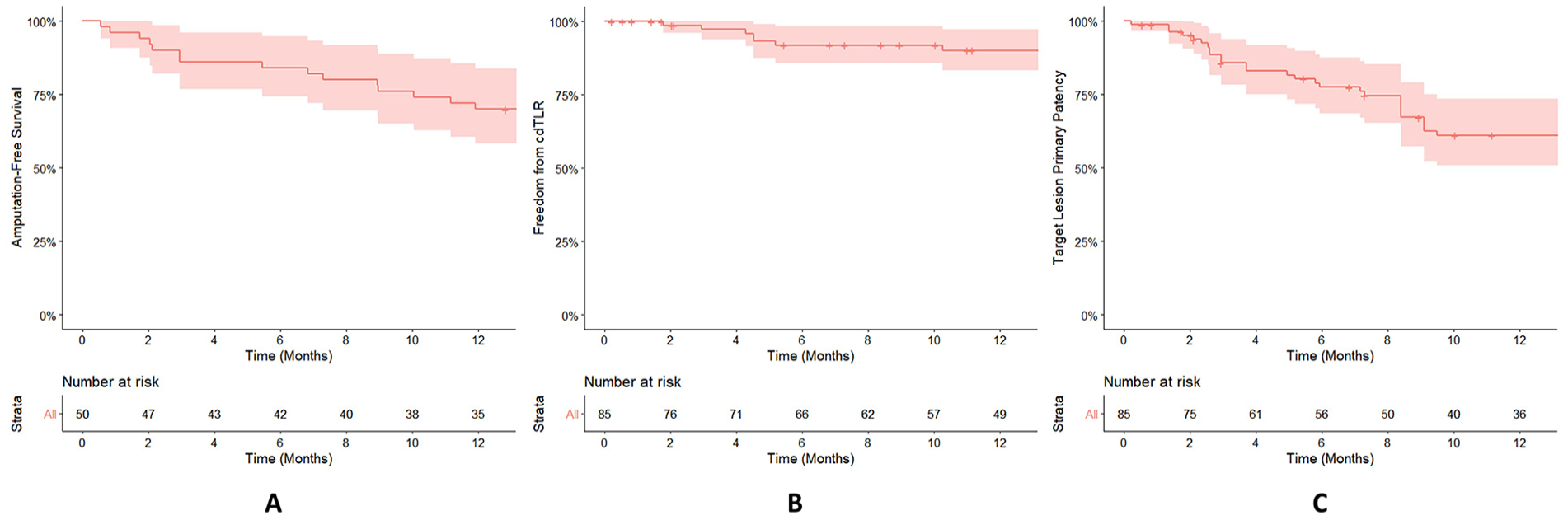
Amputation -Free Survival rate (A), Freedom from Clinically Driven Targent Lesion Revascularization rate (B) and Target Lesion Primary Patency rate (C) at 12 months calculated by Kaplan-Meier analysis were 70% (95% CI, 58.4 – 83.9%), 90.1% (95% CI, 83.4 – 97.4%) and 61.1% (95% CI, 50.7 – 73.6%) respectively.
Freedom from cdTLR: The freedom from cdTLR at 6 months and 12 months were 91.8% (95% CI: 85.8%-98.3%) and 90.1% (95% CI: 83.4%-97.4%), respectively (Figure 1B). The mean time to reintervention was 155.8±99.5 days.
Secondary Outcomes
In the 12-month study period, 29 patients (82.9%) showed an improvement in Rutherford score postprocedure. 22 (50.0%) patients had complete wound healing with absence of claudication or rest pain (Rutherford 0) at 12 months postprocedure. TLPP was 77.6% (95% CI: 68.7%-87.6%) and 61.1% (95% CI: 50.7%-73.6%) at 6 and 12 months, respectively (Figure 1C).
Subgroup Analysis of Diabetic Patients
43 (86%) patients had diabetes mellitus. In this particular group, AFS at 12 months postprocedure was 67.4% (95% CI: 54.8%-83.0%); the freedom from cdTLR at 12 months was 89.9% (95% CI: 82.3%-97.9%); the TLPP at 12 months was 64.9% (95% CI: 53.7%-78.4%).
Discussion
In patients with chronic limb threatening ischemia and lower limb tissue loss, it is often crucial to get inline straight line blood flow to the foot to aid wound healing. While it was previously thought that patency is only essential for the period of wound healing, this tide-over concept is now being challenged. Studies have reported that loss of arterial patency is associated with poorer outcomes such as delayed wound healing and increase in major amputations.14,15
Maintaining vessel patency is often challenging, especially in patients with diabetes and end-stage renal failure, as these patients have predominantly BTK disease, with long segment TASC C and D lesions, consistent with the patients in our study group. These highly calcified lesions also makes recoil more common and faster to occur.
BTK angioplasty is traditionally done using semi-compliant balloons, and this is often associated with poor results, due to high rates of recoil and restenosis.4,5 A recent meta-analysis reported a 71.6% freedom from clinically driven target lesion revascularization after BTK angioplasty. 16 Unfortunately, the use of adjunctive devices has not been shown to improve BTK angioplasty results significantly. Oh et al 16 showed that stenting did not improve limb salvage or AFS in patients with BTK disease and chronic limb threatening ischemia. Benfor et al 5 also concluded that there was no significant difference in limb salvage, restenosis rates, target lesion revascularization and AFS in patients who had drug-eluting balloons versus plain old balloon angioplasty for BTK disease. The use of atherectomy devices have also not shown to be superior in the BTK arteries. Possible reasons for the lack of improved results is likely due to much smaller diameters and more calcifications in the BTK arteries as compared with the larger, more proximal arteries, limiting space for scaffolding or absorption of drug therapy.
Balloon compliance is defined by the diameter increase that results from a predetermined increase in inflation pressure. 17 Semi compliant balloons are typically made of Pebax or higher-durometer polyurethanes, and increase in diameter in response to an increased inflation pressure. In contrast, noncompliant balloons are usually made of nylon or polyester, expand uniformly when inflated and typically do not increase in diameter past a predetermined limit. When a balloon is inflated, a semi-compliant balloon will respond to an increase in pressure by initially increasing balloon diameter in the areas proximally and distal to the lesion. 18 This results in radial force being unevenly distributed along the treated segment and the classic waisting and “dumbbell shape” noted during balloon inflation. This resultant deformation of vessel on either side of lesion potentially increases the risk of vascular damage of the vessel proximal and distal to the lesion. 19
To our knowledge, there are limited studies reporting the use of noncompliant balloons in the peripheral vasculature. An initial study by Tang et al 20 reported a 67% AFS at 1 year. However, this was retrospective, single-operator study involving a mixed cohort of patients some of whom had semi-compliant and paclitaxel coated balloons used in the same procedure. Another study by Huizing et al 21 also used noncompliant balloons selectively and concluded that noncompliant balloons were safe and feasible for use in the lower limb arteries.
In our study, noncompliant balloons were exclusively used without any adjuncts, as we wanted to remove any technical procedure related confounding factors in our study. None of our patients had intra-procedure vessel ruptures despite the high inflation pressures of noncompliant balloons. This is likely due to the even pressure distribution across the lesion with no dog-boning effect at the edge of the lesions. It is also our institution’s practice to do Duplex arterial ultrasound scans for diagnosis and pre-procedure planning. Compared with traditional CT angiography, the use of duplex ultrasound reduces a patient’s exposure to contrast media as well as radiation. At the same time, this allows for accurate measurement of the vessel size and appropriate balloon selection to prevent unnecessary vessel trauma from an oversized balloon.
In our patient population, there is a very high proportion of patients (90%) with Rutherford 5 and 6 disease, with more than half the patients deemed to be at moderate to high risk of major amputation based on the clinical stage of their WIfI score. 22 To compound the problem, our patients also have a high incidence of diabetes mellitus and end-stage renal failure, with associated infrapopliteal long lesion lengths of >20cm (Figure 2), much longer than typical sub-10cm tibial lesions that have been reported in other studies involving in BTK angioplasties.9,10 Despite having these poor prognostic factors, we managed to achieve an AFS of 70% at 12 months, and a 1-year freedom from cdTLR of 90.1%. This appears to be promising compared with previously published results5,13,16 that featured patients who have less co-morbidities and less complex lesions. On follow-up Duplex ultrasound, we also noted a 12-month TLPP of 61.1%, which suggests that long lasting patency can be achieved with the use of noncompliant balloons alone, without further adjuncts. We postulate that the high pressures could have an effect in causing microfractures in the calcified arterial walls, thus changing the compliance of the vessel wall and limiting rapid restenosis. The use of a single modality in treatment also helps to limit the costs of treatment in this group of patients, which is important in places where patients have to bear most of the costs of their treatments.
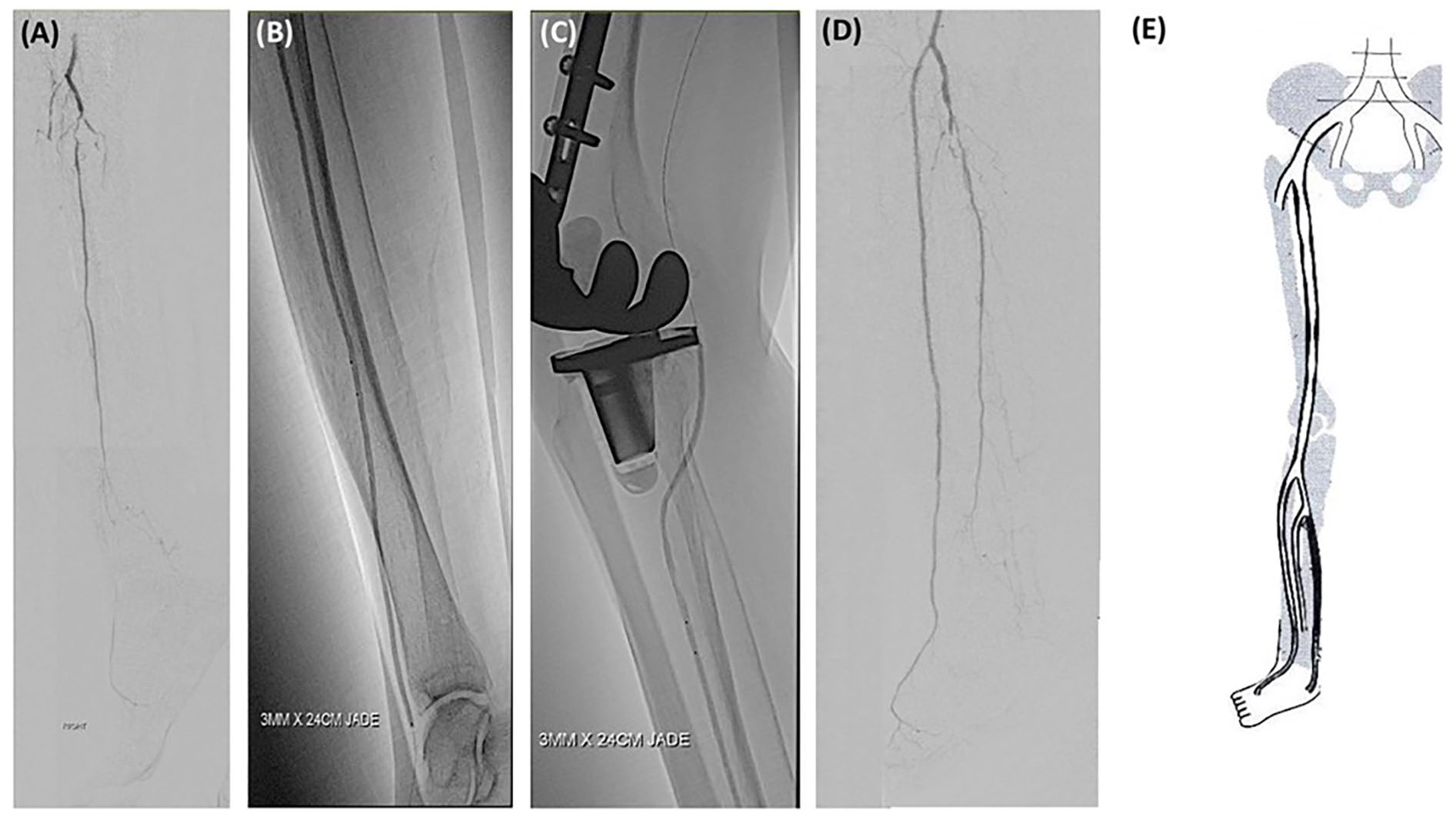
A 30cm long occlusion of the anterior tibial artery treated with non-compliant Jade™ balloon catheter. (A) The pretreatment angiogram. (B,C) Anterior Tibial Artery angioplasty with a 3.0mm x 240mm Jade™ balloon catheter. (D) Post-treatment angiogram showing good luminal gain in the anterior tibial artery. (E) Duplex ultrasound performed at 1-year post-op shows patency of the treated anterior tibial artery.
Limitations
Some limitations of our study were that this is a single-center single-arm small cohort prospective study, which could have resulted in some selection bias. There was also more than one procedurist involved and the varying skill level of each procedurist could have impacted the outcomes. In addition, we evaluated TLPP with the use of duplex ultrasound instead of angiography, and there was no adjudication of an independent core lab. Despite these limitations, this study demonstrates encouraging preliminary outcomes in our population and will serve as a pilot for a larger scale comparative study in future.
It was also unfortunate that during our study period, 8 patients passed on and 7 underwent major amputations, which could have added a bias to the TLPP results. However, this reflects the real-world situation of these patients who have many co-morbidities and cardiovascular risk factors, and often die of unrelated causes despite our best efforts at managing their CLTI.
Conclusion
Our study has shown that the use of a high pressure, noncompliant balloon is effective in lower limb angioplasty for CLTI in a highly challenging group of patients with a high prevalence of diabetes and end-stage renal failure. Good vessel patency and limb salvage can be achieved with a low rate of intraprocedural complications. This is a useful and relatively easy-to-use addition to the existing armamentarium that we have for treating patients with lower limb CLTI and we await more long-term outcomes.
Footnotes
Author Contributions
TYT, CTT, YHY, and CY was involved in gaining ethical approval, patient recruitment and data collection. CSL was involved in data analysis and interpretation. YHY drafted the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Investigator-Initiated funding from OrbusNeich.
Ethical Statement
The study was reviewed and approved by SingHealth Centralized Institutional Review Board (CIRB Ref 2020/2425). Written informed consent was sought from patients in accordance with Good Clinical Practice standards and ethical principles of Declaration of Helsinki.
Clinical Trials Registration
NCT04534192.