
Abstract
Background:
Thrombotic material in the non-aneurysmatic and non-atherosclerotic aorta is a rare entity without any recommended standard treatment so far. We present a successful treatment strategy for patients who do not fit into any of the common approaches.
Case report:
A free-floating thrombus in the descending aorta was found as source of embolism in an 82-year-old female patient with lower limb ischemia. After initial heparinization of the patient without relevant reduction of the thrombotic mass, the thrombus was removed using an interdisciplinary approach. Under echocardiographic guidance to locate the thrombus, the AngioVac device, usually licensed to remove floating thrombi from the venous system, was used off-label to remove the thrombus by a transfemoral approach. To avoid rebuilding of a new thrombus, the attachment point with an exulcerated plaque in the descending aorta was covered by a stent graft via the same femoral access. The patient did not experience any further embolic events, and the postoperative course was uncomplicated.
Conclusion:
Patients with uncommon aortic diseases, such as the reported free-floating thrombus, should be treated by an individualized, interdisciplinary approach. Besides the recommended treatment options, there are other uncommon approaches that might offer an alternative in complex cases.
Clinical Impact
Evidence is rare for the treatment of a free-floating thrombus in the descending aorta and the treatment strategy remains discussed controversially. We present a rather uncommon approach of successful off-label treatment for patients who do not fit into any of the common approaches (operative, endovascular, or conservative treatment based on patient’s comorbidities). The AngioVac System has already been successfully used off-label in the arterial system but not in the above presented way of treating a free-floating thrombus in a patient with high embolization risk and treatment-limiting comorbidities.
Introduction
A free-floating thrombus within non-aneurysmatic and non-atherosclerotic aortic segments especially in the absence of thrombophilia or malignancy is a rare entity, without an available standard treatment strategy.1,2 Current clinical guidelines recommend an individualized treatment decision based on the patients’ co-factors and condition to decide whether to use an operative, endovascular, or a conservative strategy. 3 Conservative management involves administration of unfractionated heparin to dissolve the thrombus usually as initial and less invasive treatment and especially for patients who are unfit for surgery or endovascular treatment. More invasive strategies like surgery or endovascular repair depend strongly on the centers’ range of expertise. We discuss a case, which combines more than 1 strategy in a multidisciplinary team of vascular surgeons, cardiac surgeons, and anesthesiologists using the AngioVac System (AngioDynamics, New York) in an off-label use within the arterial system.
Case Report
An 82-year-old female patient presented with left lower limb ischemia at a peripheral hospital. Revascularization of the affected limb was successfully done by transfemoral thrombectomy. As a source of embolism, a free-floating thrombus attached to the proximal descending aorta was detected in computed tomography (CT) scan (Figure 1.1). First, a conservative treatment strategy was performed using intravenous administration of unfractionated heparin. Another CT scan revealed no relevant reduction of aortic thrombus mass. In a multidisciplinary board, further treatment options were discussed. Due to age and pre-existing comorbidities (status post left pancreas resection and splenectomy for pancreatic tumor and right hemicolectomy and ileo-descendostomy with short bowel syndrome for colon carcinoma), open surgical removal of the thrombus was considered to be associated with a high perioperative risk. Endovascular treatment by placement of a thoracic endograft was considered to be at high risk for fatal embolization. The idea of using the AngioVac (AngioDynamics, New York) in the arterial system had already been successfully conducted in the ascending aorta. It was the first time using this system “off-label” for a thrombectomy in the descending aorta in a hybrid setting with endovascular stenting of the attachment point.
In preparation for the AngioVac System, a conduit (12 mm Gelsoft Plus, Vascuthek, Inchinnan, UK) was anastomosed to the left femoral artery. A venous cannula was percutaneously inserted to the right femoral vein to return the retrieved and filtered blood to the patient. After insertion of the AngioVac System via the conduit, the tip of the system was placed under echocardiographic control between the distal end of the thrombus and the origin of the celiac trunk, to prevent visceral embolism.
At a flow volume of 2 L/min, the floating thrombus could be removed in toto (Figure 1.2). To avoid rebuilding of a new thrombus, the attachment point with a persistent exulcerated plaque in the descending aorta was covered by a thoracic endograft (Medtronic-Valiant-Navion VNMC2828C90TE), inserted via the same femoral access.
The postoperative CT scan showed a proper position of the endograft with a short juxtarenal dissection flap, without hemodynamic compromises, distal to the endograft. The patient did not experience any further embolic events or other complications. The patient was transferred to her home hospital on the seventh postoperative day with a single antiplatelet therapy. In the 1-year follow-up including CT scan, the patient was symptom free regarding any embolic events.
Discussion
Current clinical guidelines describe a free-floating thrombus within a healthy aortic segment, especially in the absence of thrombophilia or malignancy as an uncommon clinical entity. Mostly, the floating thrombus is related to a prior aortic injury (dissection, atherosclerotic plaque, or trauma). 1 Either way, the treatment strategy for a free-floating thrombus remains discussed controversially.1,4 According to clinical guidelines, the best strategy depends on the pre-existing comorbidities, extension of the thrombus, embolic complications, and the physician’s preferences. 3
Evidence is rare as most of the recommendations are based on case reports or experts’ opinion. Every case should be discussed in multidisciplinary teams. Within the presented case, embolism of the floating thrombus, especially to the visceral segment with fatal consequences, was a likely scenario. Therefore, a sole endovascular treatment was not favorable. Open surgery was discussed, but due to the age and the pre-existing comorbidities of the patient, open thoracic aortic repair was considered with high perioperative risk. As the considered strategies did not seem to fit for our patient, we were looking for a safe alternative method. After the AngioVac procedure to remove the thrombus, an exulcerated plaque was left. As therapeutic anticoagulation failed to dissolve or at least reduce the thrombus mass before, the decision to insert a stent graft in a hybrid setting to secure the attachment point was made.
The AngioVac System is licensed by the United States Food and Drug Administration (FDA) since 2009 for vacuum-assisted thrombectomy of intracardiac masses and intravenous thrombi in the right atrium, the right ventricle, and the vena cava. In a safety report of the RAPID registry (Registry of AngioVac Procedures in Detail), a total of 234 patients were prospectively registered from March 2016 to August 2019. Authors reported about the removal of 70% to 100% of thrombus mass in 73.6% of patients with caval thrombus, 58.5% with right heart thrombus, 60% with catheter-related thrombus, and 57.1% of patients with pulmonary embolism. Complications included blood loss with need for transfusion (25.2%) and 36 procedure-related complications, including one periprocedural death. 5 Regarding these registry data and other studies, the safe and successful use of the AngioVac System was confirmed.5,6 There is also literature of the safe use of the AngioVac System in the aorta. The device was used in the ascending aorta to remove a free-floating thrombus similar to our case in the University Hospital of Hamburg/Germany. 7
During the COVID-19 pandemic, an accumulation of thromboembolic events has been reported being associated with the hypercoagulable state related to an infection with COVID-19. The pathophysiology behind the increased hypercoagulability and increased thromboembolic events in COVID-19 patients is not well understood but likely includes vascular endothelial cell injury, inflammation, activation of the coagulation cascade, and shutdown of fibrinolysis. 8 There is a report about cases of COVID-19-related aortic thrombosis, with two of them presenting with a floating thrombus despite an antithrombotic prophylaxis. Both of them were treated successfully by intravenous administration of unfractionated heparin. 9 The conservative approach is the most common initial and less invasive treatment. 2 It is also the best approach for patients who are unfit for surgery or endovascular treatment. In case of residual thrombus or recurring embolic events, more invasive treatment strategies like surgical and endovascular repair are often conducted.4,10 There is also a case report about the successful use of the AngioVac System in the aortic arch and the descending aorta to remove a thrombus. Source of this thrombus was likely a hypercoaguable state during a current COVID-19 infection. 11 Since COVID-19 has the potential to establish seasonality, 12 associated arterial thrombotic complications might occur more often. Alternative treatment strategies compared with conservative, surgical, or sole endovascular strategies should become more present and should be taken into account depending on the patient’s condition, localization of the thrombus, and previous embolic events.
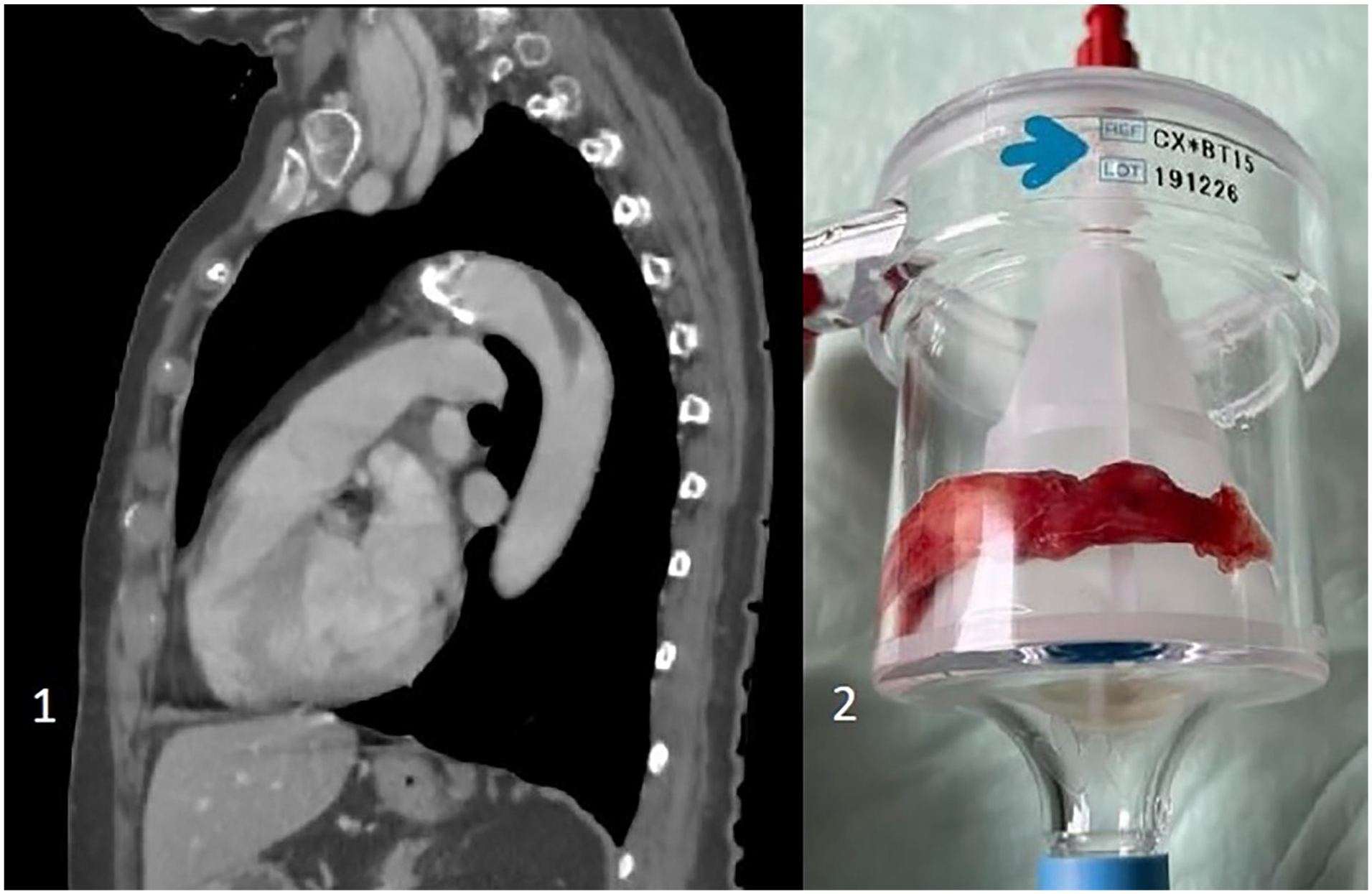
The free-floating thrombus in the descending aorta in the preoperative CT-scan (1) and after removal in the AngioVac System (2).
Conclusion
In this case report, a free-floating thrombus was removed from the descending aorta in a patient who was not suitable for one of the common treatment strategies. This case report should provide another approach for special selected patients, which should be discussed in a multidisciplinary team. It underlines that the AngioVac system can be used safely in selected patients within the arterial system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.