
Abstract
Purpose:
To present a novel technique that enables safe and effective cannulation of target vessels with challenging anatomy during fenestrated/branched endovascular aortic repair (F/B-EVAR).
Technique:
Following deployment of the F/B-EVAR endograft, the target vessels (TVs) are cannulated. The bundle wire technique provides a solution to challenging TVs and uses multiple fine atraumatic guidewires that together serve as a stiff guidewire. The technique can be executed in 2 ways using: (1) one 0.018 inch and one 0.014 inch guidewire or (2) three 0.014 inch guidewires. We demonstrate the technique in a case of a complex abdominal aortic aneurysm treated using branched EVAR in which the left renal artery with severe ostial stenosis was catheterized using the bundle wire technique.
Conclusions:
The bundle wire technique offers a technically feasible and economically viable solution for facilitating catheter and bridging stent delivery in anatomically challenging TVs during F/B-EVAR. It is a useful addition to the therapeutic armamentarium available to physicians for accessing demanding TVs.
Keywords
Introduction
In recent years, fenestrated/branched endovascular aortic repair (F/B-EVAR) has emerged as the preferred treatment for complex abdominal aortic pathologies, offering better outcomes in terms of morbidity and mortality compared with open surgery. 1 A key aspect of successful F/B-EVAR is the effective revascularization of mesenteric and renal vessels. 2 However, cannulating target vessels (TVs) can often prove challenging due to the presence in them of the same pathology that affects the aortic wall, such as calcification, stenosis, thrombosis, or dissection. Anatomical variations can also jeopardize TV cannulation, including tortuous course and upward-facing ostia.
Ensuring proper guidewire cannulation of TVs is crucial. Subsequently, safe delivery and deployment of a bridging stent at the desired site becomes essential to achieve adequate vessel perfusion and sealing of the aortic pathology. 3 Hence, innovative solutions are sought to overcome this dilemma. In this context, we introduce the “bundle wire” technique as a valuable alternative approach for addressing these challenging scenarios.
Technique
In our institution, branched endovascular repair (BEVAR) procedures are usually performed using bilateral femoral accesses with percutaneous means using ultrasonography and the use of right axillary artery by open surgical exposure. The femoral accesses are used for imaging and deploying the aortic endograft, whereas the axillary access is used to cannulate and deliver bridging stents for the TVs. After the main endograft (F/B-EVAR) is deployed, subsequent TV cannulation takes place. A 7F long Flexor sheath (Cook Medical, Bloomington, Indiana) is introduced up to the level of the ostium of the TV for increased stability. Next, a 5F Berenstein II catheter (Cordis, Santa Clara, California) is introduced through the sheath and aids in directing a 0.035 inch hydrophilic guidewire (Terumo Medical Corporation, Somerset, New Jersey) into the TV. Challenges that could be encountered at this stage include severe ostial stenosis, thrombosis, dissection, and upward-facing or tortuous course of vessels. If TV cannulation using this wire is not possible, a switch to a 0.018 inch or 0.014 inch guidewire becomes necessary. Following 0.014/0.018 inch guidewire entry into the TV, tracking a catheter over it into the TV to exchange to a stiff 0.035 inch guidewire may not be possible due to lack of stability provided by the 0.014/0.018 inch guidewire. In such situations, the bundle wire technique can be usefully employed. The technique is achieved using readily available off-the-shelf guidewires. It can be implemented by 3 methods.
Method 1
After the F/B-EVAR endograft is deployed, a Berenstein catheter along with a long sheath are brought into position adjacent to the ostium of the TV. A 300 cm 0.014 inch soft-tip guidewire (Boston Scientific, Marlborough, Massachusetts) is introduced to gain access to the TV. Next, another 300 cm guidewire (Terumo Medical) of slightly larger profile (0.018 inch) is introduced in a parallel manner through the Berenstein catheter into the TV. The 2 wires now behave as one unit that has comparable stiffness as a 0.035 inch guidewire but with the added benefit of safe gentle tips. This is what we call the bundle wire. The Berenstein catheter is removed and exchanged with a 0.035 inch compatible support or crossing catheter such as NaviCross (Terumo Medical) over the bundle wire and advanced distally into the TV. The sheath could be advanced as well to provide more stability and prevent unsafe deployment of bridging stents especially balloon expandable covered stents. Ostial angioplasty could also be performed before delivering the bridging stent, although it is not routinely performed. Once the support catheter is in a secure position inside the TV, the guidewires are removed and replaced with a Rosen guidewire (Cook Medical). Now, the bridging stent can be safely advanced into the TV to be deployed. Finally, contrast angiography is performed from the long sheath to visualize the vessel anatomy and identify any potential complications.
Method 2
The same sequence of steps is followed, but this time, two 0.018 inch guidewires (Boston Scientific) are used instead of one 0.014 inch and one 0.018 inch. The bundle wire is created by cannulating the TV using the two 0.018 inch guidewires introduced through the Berenstein catheter. The 2 wires collectively behave as 1 stiff guidewire.
Method 3
It is possible to use three 0.014 inch guidewires (Boston Scientific) instead of 2. The bundle wire is created by cannulating the TV using the three 0.014 inch guidewires introduced through the Berenstein catheter. The 3 wires collectively behave as 1 stiff guidewire. However, this way, although effective, could result in a greater amount of friction and difficulty when advancing over the catheter.
A homemade aortic model was created for a simple illustration of the technique. Supplemental Video 1 shows how unstable the use of one 0.018 guidewire for catheter cannulation and may result in the loss of TV wire cannulation. Supplemental Videos 2 and 3 demonstrate better stability for the delivery of the catheter and the following steps; using one 0.018 and one 0.014 guidewire, and using three 0.014 wires, respectively (Supplemental Videos 1, 2, and 3).
It is important to note that when the bundle technique is used, the 2 wires may or may not be in the same vessel/branch. Although having the wires in 2 different branches can hinder the advancement of the catheter or the balloon through the main TV, it may help protect against unintentional distal deployment of the bridging stent and side branch coverage.
Case Presentation
A 69-year-old male was referred for a type Ia endoleak detected on follow-up computed tomography angiography (CTA) surveillance 6 months after a standard infrarenal aortic EVAR. Pre-operative CTA images revealed type Ia endoleak with maximum dimensions of 90.7 × 60.4 mm as well as infolding of the aortic endograft at the proximal landing zone. There was associated severe stenosis and mural thrombosis of the left renal artery (LRA) ostium (Figures 1–3). A remedial BEVAR procedure was planned. A custom-made device BEVAR (Cook Medical) prepared for another patient was found compatible to the anatomy of our patient and a decision was made to use the endograft.
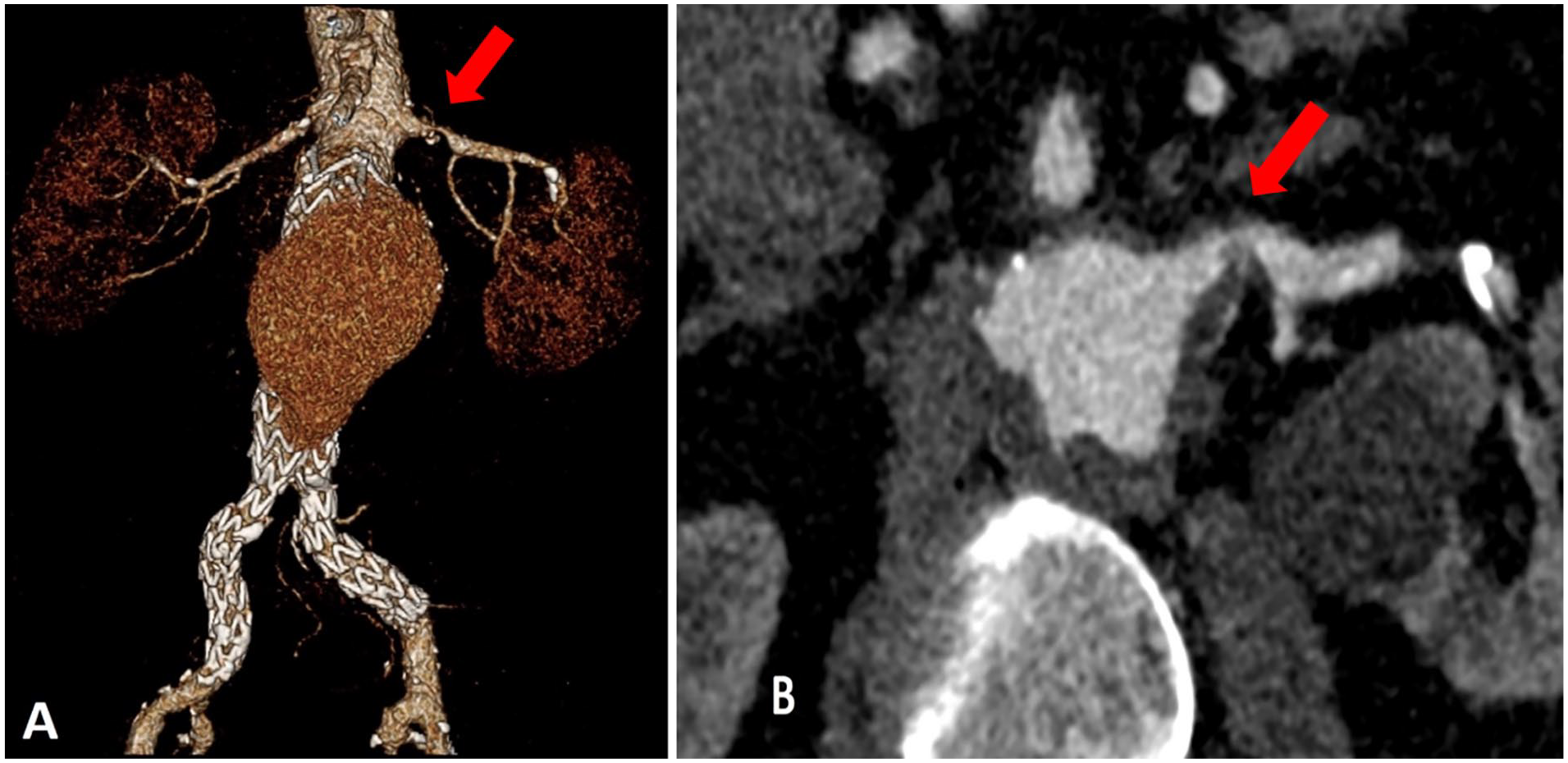
A and B: Pre-operative CT images with type I A endoleak and tight stenosis of the left renal artery ostium (denoted by the red arrow).
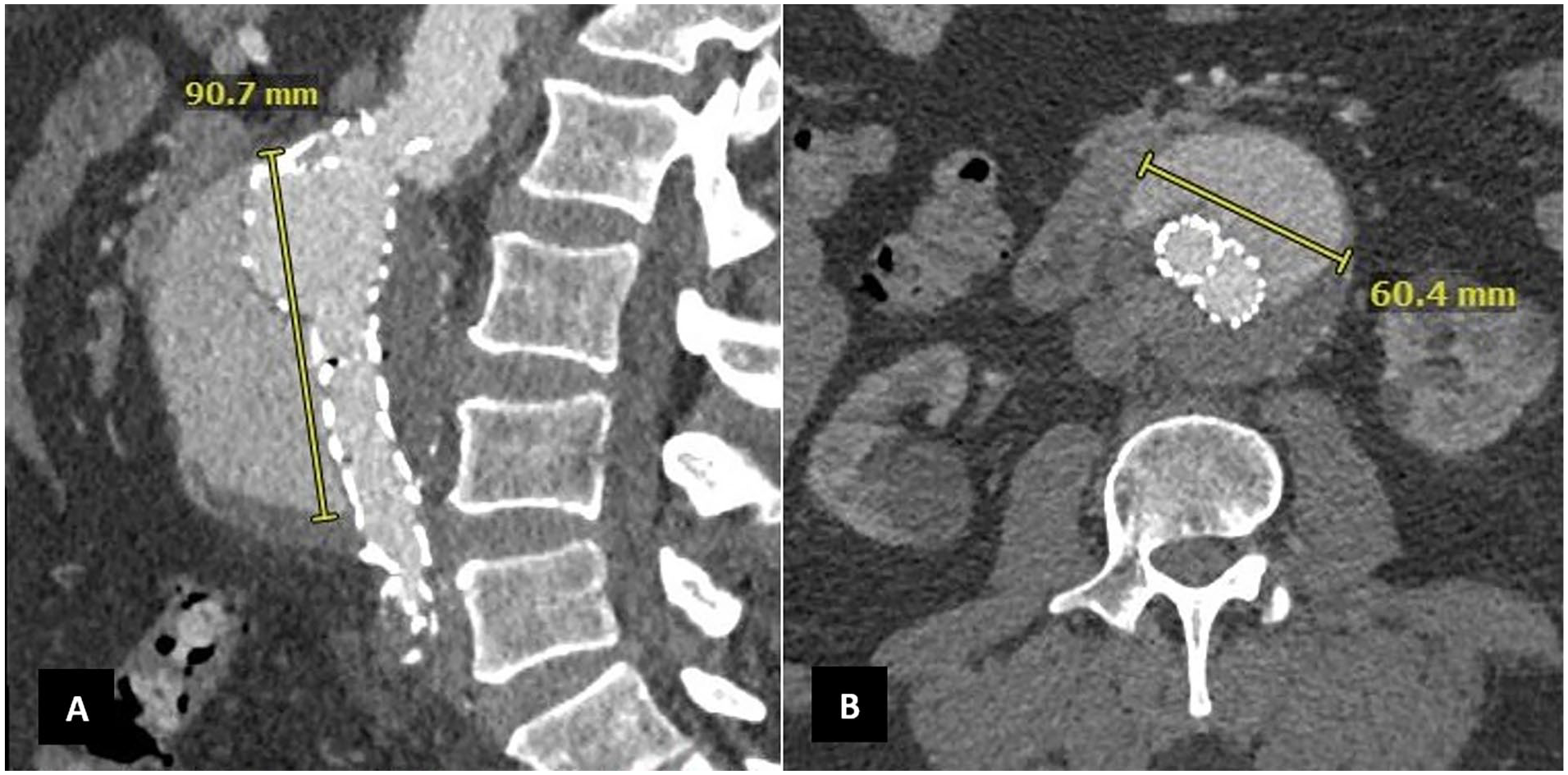
A and B: Endoleak Ia with maximum dimensions 90.7 × 60.4 mm.
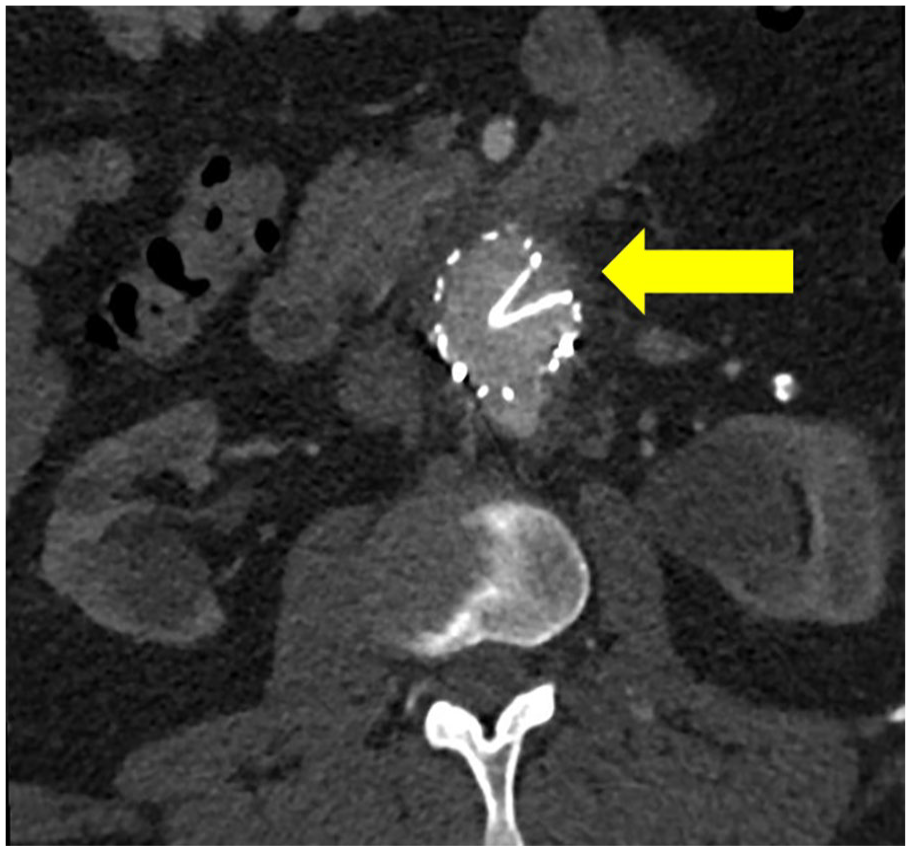
Infolding of the previous EVAR endograft (yellow arrow).
The procedure was performed in a hybrid operating theater with an incorporated fixed imaging system. Transfemoral arterial access was obtained using ultrasound guidance. Full heparinization was initiated. Target activated clotting time (ACT) of 250 to 300 seconds was maintained by measuring the ACT level every 30 minutes. Intraoperative digital subtraction angiography confirmed the presence of endograft infolding and LRA ostial stenosis (Figure 4).
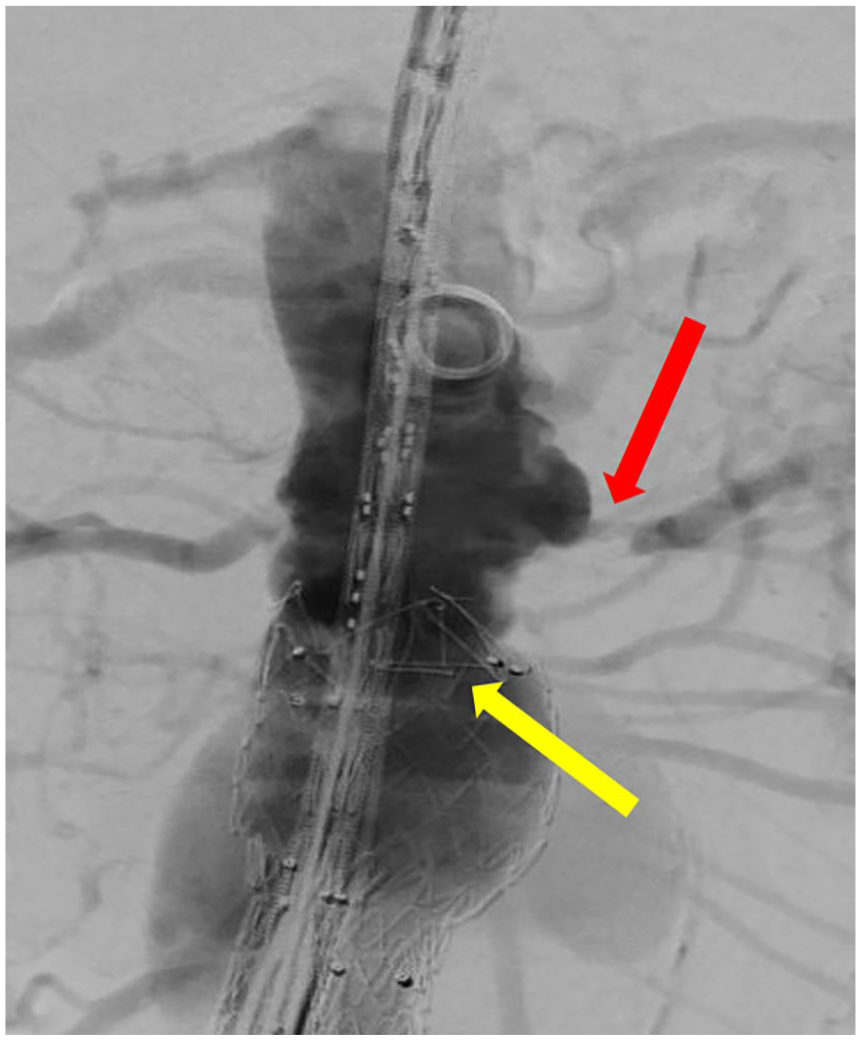
Intraoperative angiography images of the tight stenosis of the LRA (blue arrow) and the previous existing infolding (yellow arrow).
The BEVAR endograft was deployed at its planned position. Then, a 7F-long Flexor sheath was positioned near the ostium of the LRA to provide stability for subsequent maneuvers. A 5F Berenstein II catheter and a 0.035 inch guidewire were introduced through the Flexor sheath and directed toward the LRA ostium. Attempts to safely cannulate the LRA were unsuccessful. Hence, cannulation was reattempted using a 0.014 inch guidewire and 0.035 inch compatible support catheter (Figure 5). Following successful guidewire cannulation, attempts to advance the support catheter into the LRA proved ineffective. Consequently, we opted to use our innovative bundle wire technique. The support catheter was carefully withdrawn and replaced with the 5F Berenstein catheter. A parallel 0.018 inch guidewire was introduced through the catheter and directed toward the LRA ostium (Figures 6A and B and 7).
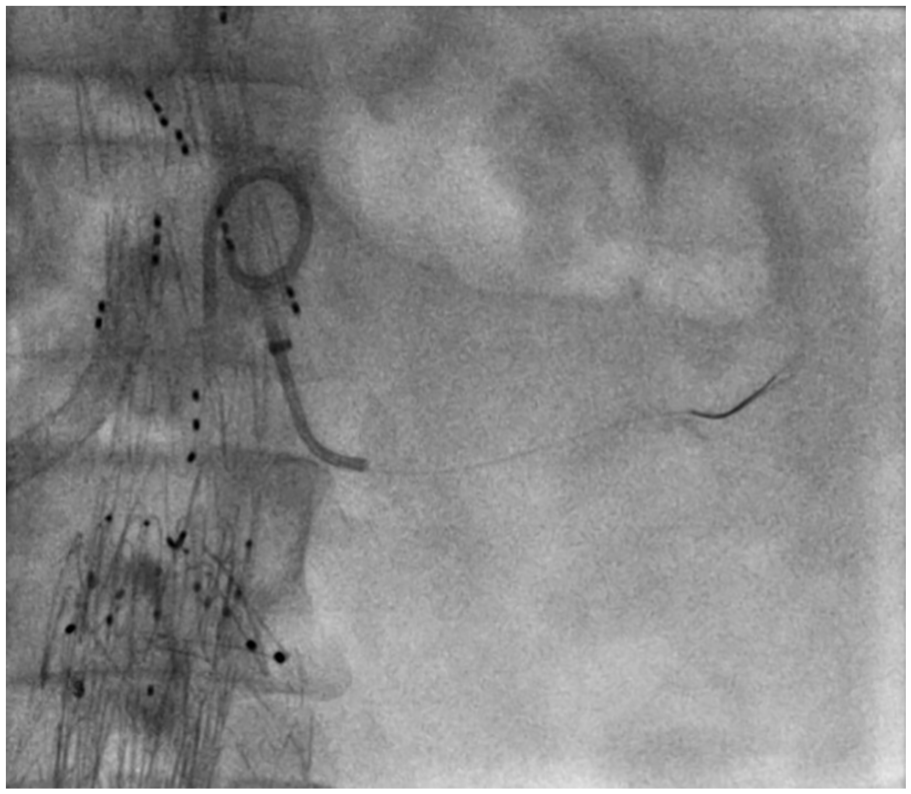
Passage of 0.014 inch guidewire.
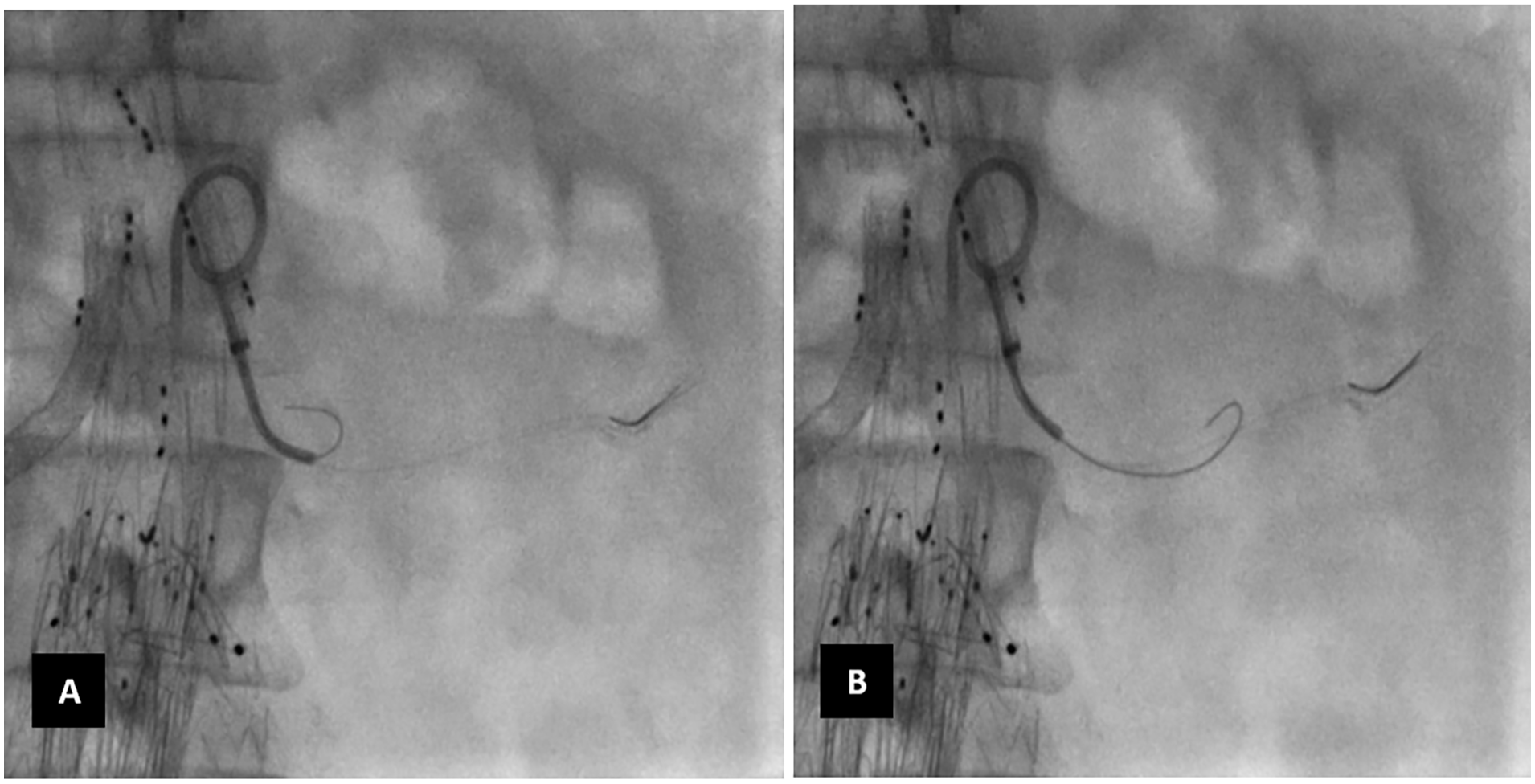
A and B: Passage of 2nd 0.018 guidewire into the left renal artery.
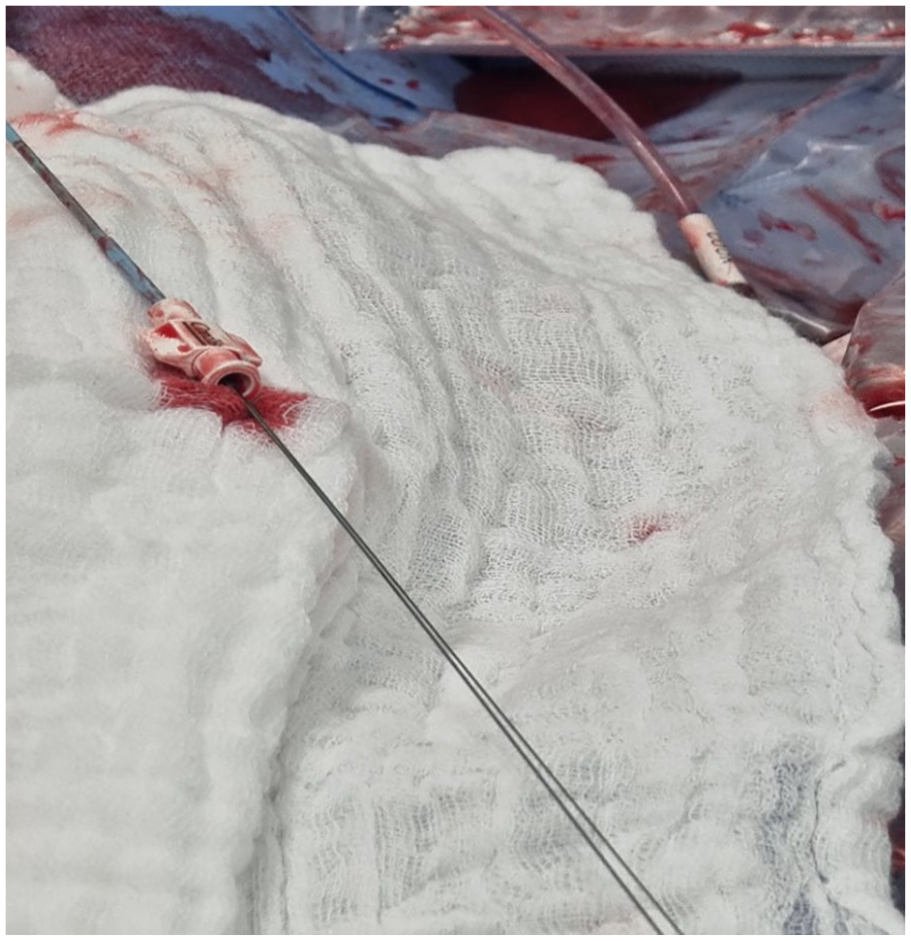
The external parts of the 2 guidewires used.
Following the successful placement of the 2 guidewires in the LRA, the Berenstein catheter was removed and a 0.035 inch compatible support catheter (NaviCross, Terumo Medical) was introduced distally into the LRA over the bundle wire.
The bundle wire was then replaced with a Rosen guidewire (Cook Medical) for the upcoming stent delivery. The stent of choice was brought into place and deployed. The outcome of this procedure showcases the safe and successful revascularization and bridge-stenting of the LRA, with no apparent complications (Figure 8).
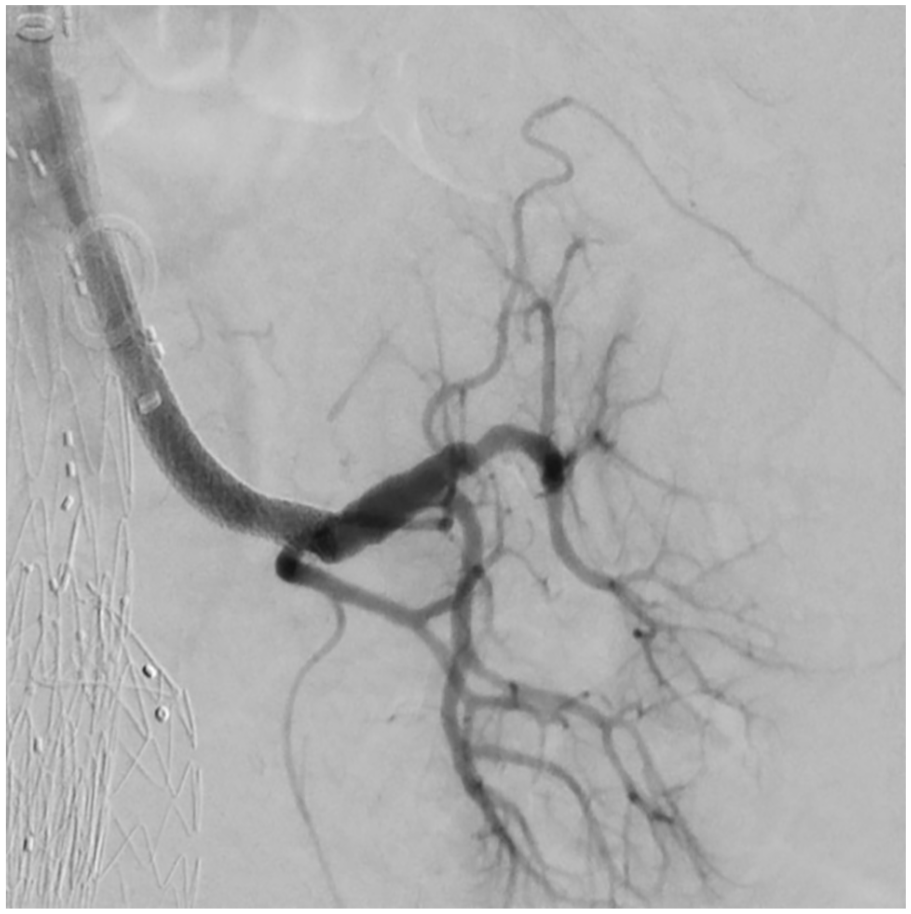
Successful stenting of the left renal artery.
The procedure took around 54 minutes regarding fluoroscopy time, radiation dose of 2347 cGy/cm2, and contrast volume of 246 mL.
Discussion
Safe and efficient cannulation and perfusion of reno-visceral vessels are essential for successful endovascular treatment of complex abdominal aortic pathologies. 2 However, this can become challenging in some patients due to extensive pathologies, such as severe stenosis, calcification, thrombosis, and vessel tortuosity. These factors can hinder standard guidewire cannulation and stent delivery, jeopardizing organ perfusion and overall treatment success. 3
Initial cannulation of TVs in F/B-EVAR is usually with a 0.035 inch standard (soft) guidewire. However, standard (soft) guidewires cannot be used to deliver a balloon or a bridging stent into TVs, especially severely diseased TVs, and could lead to loss of vessel access. Safe delivery of bridging stents into the TV requires a stiff guidewire which is introduced into the TV through a 0.035 inch compatible support catheter in exchange for the standard guidewire. Commonly used stiff guidewires are the Amplatz Super-stiff guidewire (Boston Scientific) and the Rosen wires (Cook Medical), which both have a 0.035 inch caliber. The initial cannulation of the TV using standard 0.035 inch guidewires may not always be successful, especially in anatomically challenging mesenteric or renal vessels. In this situation, a smaller caliber and more steerable guidewire (0.014 or 0.018 inch) may be successful in cannulating the TV, but this may not provide enough support to allow safe passage of a 0.035 inch compatible catheter into the TV, especially when TVs have an upward course or have severely diseased ostia. The NaviCross crossing catheters have been an effective tool in crossing severely stenosed and occluded vessels especially with the telescope technique which provides seamless transition and better pushability.4,5 However, in the case presented, when the catheter was advanced into the LRA, exchange with a stiff wire resulted in loss of the cannulation. This could be explained by the directional changes where a transition from the aorta to the TV possesses a real challenge. If catheters face difficulty during TV cannulation, then increased introduction forces should not be used as the safety and integrity of the TVs remain uncertain after such passage.
Target vessel cannulation in the presence of anatomical challenges poses a real threat to the technical and clinical success of BEVAR procedures. Factors such as long procedure and fluoroscopy times, increased contrast dose, and physician mental stress have a negative impact that can compromise the outcome of such interventions. To address these challenges, we propose our novel bundle wire technique wherein 2 (one 0.014 inch and one 0.018 inch) or 3 (0.014 inch) soft-tip guidewires together provide as much support as a stiff guidewire. Thus, the safety and crossing efficacy of soft low-profile guidewires are used while achieving support equivalent to that of stiff large-profile guidewires.
Several techniques were reported previously to address challenging TVs. Oikonomou et al 6 reported on the feasibility of retrograde TV access as a bailout technique using open surgical means, which revealed high technical success yet the procedure has been associated with incremental morbidity risk and longer hospital stay. Endovascular solutions have been also proposed. Heidemann et al 7 published the “Balloon-Anchoring Technique” where an antegrade through-the-branch guidewire was anchored using a balloon. This approach needed cannulating the TV via the femoral access, then exchanged for a stiff guidewire by which a balloon was introduced and inflated to support the through-the-branch guidewire that was used from upper access. This could be challenging in cases with narrow aortic diameters at the level of the renal arteries. In addition, the cannulation has to take place outside the main aortic device deployed. Another technique (snare-ride technique) was reported by Ferreira and colleagues where they used an Indy snare through the transfemoral route to direct the guidewire deployed from the antegrade side into the TV. 8 Once again, the technique depends crucially on the femoral access for TV cannulation, presenting the same challenges that could be faced with the “Balloon-Anchoring Technique.” The “Stabilizing Technique” presented by Zander et al 9 has used the femoral access to snare the antegrade sheath and provide reasonable stability for antegrade access into the outer branch of the BEVAR device. However, it still failed to present enough evidence to support the cannulation of TV with challenging ostia.
The bundle wire technique is entirely endovascular and can be used through the upper access without the need of additional accesses or from the lower access alone via a steerable sheath. Moreover, it does not need cannulating the TV outside the F/B-EVAR device, thereby reducing the possible threats to the device’s integrity and adverse aortic sealing outcomes. It is applicable not only in complex abdominal aortic pathologies but could also be used in peripheral interventions for chronic threatening limb ischemia where catheters may encounter difficulties passing through tight lesions after guidewire passage.
Conclusions
The bundle wire technique is a technically viable and cost-effective approach to facilitate catheter introduction, exchange, and subsequent delivery and deployment of bridging stents into visceral TVs. By overcoming the limitations of standard guidewire approaches, the technique enhances procedural safety and efficiency without imposing any economic burden. The bundle wire technique is a useful addition to the therapeutic armamentarium available to physicians for accessing challenging TVs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All the authors have no conflict of interest. N.T. is a proctor for and receives an institutional grant from Cook Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from the patient presented.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.