
Abstract
Background:
Hybrid aortic arch repair with debranching of the supra-aortic vessels carries a high risk of cerebral infarction and fatal complications associated with side clamping of the ascending aorta. A previous study had reported the “real chimney” technique, a novel method for clamp-free total debranching thoracic endovascular aortic repair with the ascending aortic sleeve banding with dacron. In this study, we aim to build upon this foundation by presenting our experience with the early and midterm outcomes of this technique.
Methods:
We retrospectively reviewed the medical records of 61 consecutive older adult patients with aortic arch pathologies and a high risk of open repair who underwent total debranching thoracic endovascular aortic repair using the real chimney technique at our institution between January 2014 and June 2022. This technique was used to anastomose the ascending aorta with the main trunk of the triple-branched prosthetic graft.
Results:
The mean patient age was 75.1 years, and 54% of patients were transferred from medical facilities with cardiothoracic surgery departments. The comorbidities included chronic obstructive pulmonary disease (49.2%), chronic kidney disease (63.9%), coronary artery disease (27.9%), and history of stroke (31.1%). No 30-day mortality was observed. Complications included postoperative renal failure requiring permanent hemodialysis (4; 6.6%), stroke (modified Rankin scale score: ≥2 in 5; 8.2%), permanent paraplegia (1; 1.6%), and permanent paraparesis (4; 6.6%). The median follow-up period was 40.5±28.5 months. The postoperative survival rates at 5 years were 66.8%. No patients experienced complications associated with the aorta or anastomosis site; only 1 patient required an additional procedure for stenosis of the anastomosis site (midterm). An aneurysmal diameter reduction of ≥3 mm was observed in 37 cases (60.7%), and the mean aneurysmal diameter reduction was 5.3 mm.
Conclusions:
The postoperative outcome of total debranching thoracic endovascular aortic arch repair is not only acceptable but also promising, particularly in patients at high risk of open repair.
Clinical Impact
Our novel real chimney technique for total debranching thoracic endovascular aortic repair of aortic arch pathologies in patients who were at a high-risk for open repair resulted in no 30-day mortality and no complications related to the aorta or the real chimney anastomosis site.
The real chimney technique is effective for managing aortic arch pathologies and enables less invasive total debranching thoracic endovascular aortic arch repair without the need for extracorporeal circulation and clamping of the ascending aorta
Keywords
This study introduces the “real chimney” technique for clamp-free total debranching thoracic endovascular aortic repair, a promising alternative particularly for high-risk older patients, reducing the risks of cerebral infarction and fatal complications associated with traditional methods. The innovation encompasses ascending aortic sleeve banding with dacron to mitigate the risks associated with clamping. With no 30-day mortality and promising 5-year postoperative survival rates of 66.8%, this technique signifies a progressive step toward safer and more effective aortic arch repair procedures, potentially altering the clinical approach to treating aortic arch pathologies and reducing the dependency on open repair strategies.
Introduction
Total arch replacement (TAR) with extracorporeal circulation (ECC) is currently the gold standard for the management of thoracic aortic arch aneurysms.1 –3 Despite dramatic improvements in the procedure and related perioperative care, the associated mortality and morbidity remain significant.4 –6 The use of hybrid aortic arch repair with endograft exclusion and debranching of the supra-aortic vessels has become more common in patients with severe surgical risks. Despite being performed without ECC, hybrid surgeries (including thoracic endovascular aortic repair [TEVAR]) involve a greater risk of cerebral stroke7,8 and retrograde type A aortic dissection (RTAD) 9 with a more proximal landing zone.
A previous study has reported the “real chimney” technique. 10 This study is aimed at investigating the early-to-midterm outcomes of patients who underwent total debranching TEVAR employing this refined technique at our institution.
Materials and Methods
Patients
We retrospectively reviewed the medical records of consecutive patients who underwent total debranching TEVAR with the “real chimney” technique for aortic arch pathologies (aneurysms and dissections) at our hospital between January 2014 and June 2022. We performed total debranching TEVAR in patients who could not endure TAR because of severe comorbidities. All patients included in this study were either considered intolerant to conventional TAR due to associated surgical risks or were rejecting TAR in favor of alternative methods. The number of debranching arteries was determined based on ensuring a sufficiently large proximal landing zone (≥25 mm). Patients with either a cardiac disease requiring surgical repair or an ascending aorta or a Valsalva diameter of >46 mm were excluded; 61 patients were included.
Ethics Approval
This study was performed after obtaining approval from the Institutional Review Board of our institution, and informed consent was obtained.
Surgical Procedures
The “real chimney” technique enables anastomosis without clamping vessels. The term “real” is used to depict how the supra-aortic branched graft, with our technique, resembles a chimney standing on the aorta, with the entry inside and the exit outside, akin to a tangible chimney. This contrasts with conventional chimney techniques, where the procedure is endoluminal, and the endograft is not externally visible. Here, it was used for anastomosis of the ascending aorta and the main trunk of a triple-branched prosthetic bypass graft.
The details of the procedure have been outlined in a previous report 10 (Figure 1). After median sternotomy and snaring of the ascending aorta, ascending aorta banding was performed using a woven polyester graft (J graft; Japan Lifeline, Tokyo, Japan) in almost all cases to achieve a smaller proximal landing zone diameter (≥40 mm). We measured the ascending aorta and decided the banding diameter preoperatively. The graft lengths were determined based on the presumed circumference of the ascending aorta, allowing room for the suturing bite. The anastomosis site was marked with a graft-sized oval (usually 12 mm in diameter). Six mattress sutures were inserted along the oval mark using a double-armed 4-0 polypropylene suture with a pledget and sutured to the oblique-cut main trunk of a triple-branched supra-aortic bypass graft (Hemashield Woven Double Velour Graft; Maquet Cardiovascular, Wayne, New Jersey) circumferentially and then tied above the ascending aorta (Figure 2A).
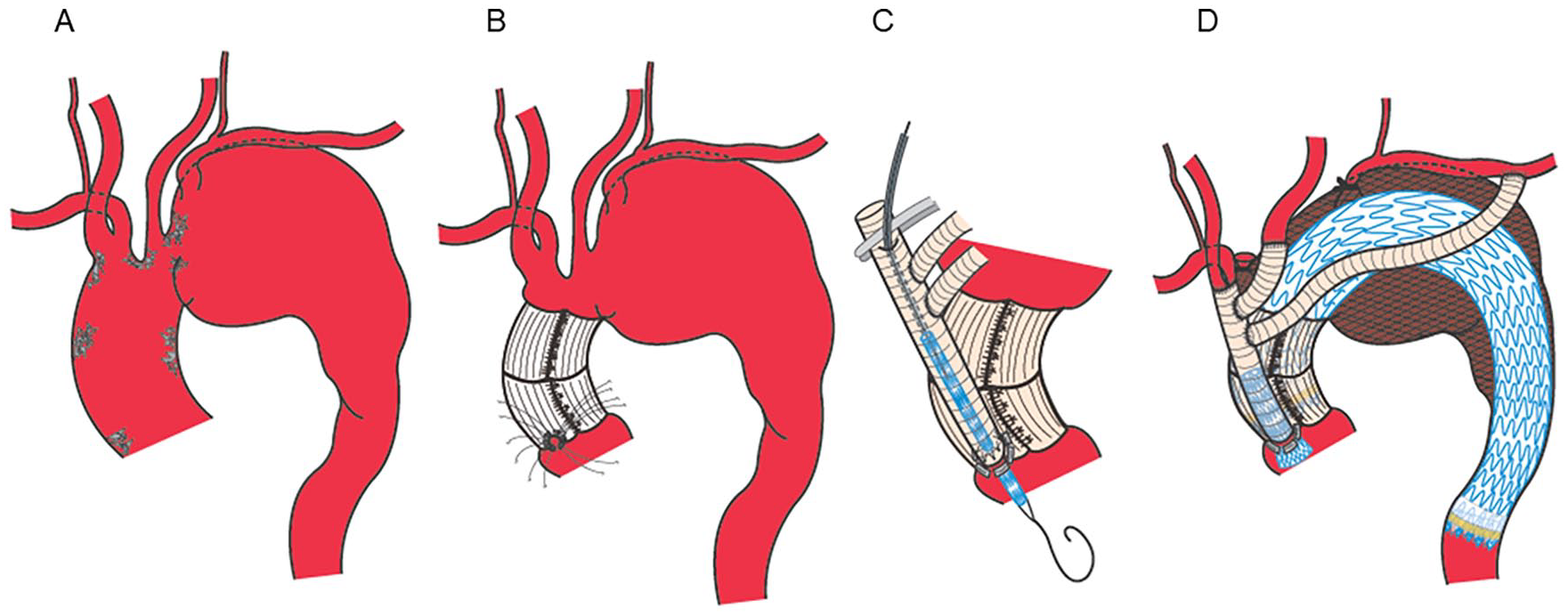
The “real chimney” technique for total debranching of supra-aortic trunks. (A) Schema of the arch aneurysm. (B) After banding of the ascending aorta, 6 mattress sutures were inserted between the ascending aorta and the main trunk of the triple-branched graft (without the use of a side clamp). The sutures pass through both the banding graft and the entire aortic wall, traversing all layers of the wall. (C) Stent graft (leg extension of the Gore Excluder; W. L. Gore and Associates, Inc, Flagstaff, Arizona) insertion from the center of the anastomosis oval through the oblique-cut triple-branched graft. (D) Complete view of the total debranching with the “real chimney” technique and thoracic endovascular aneurysm repair.
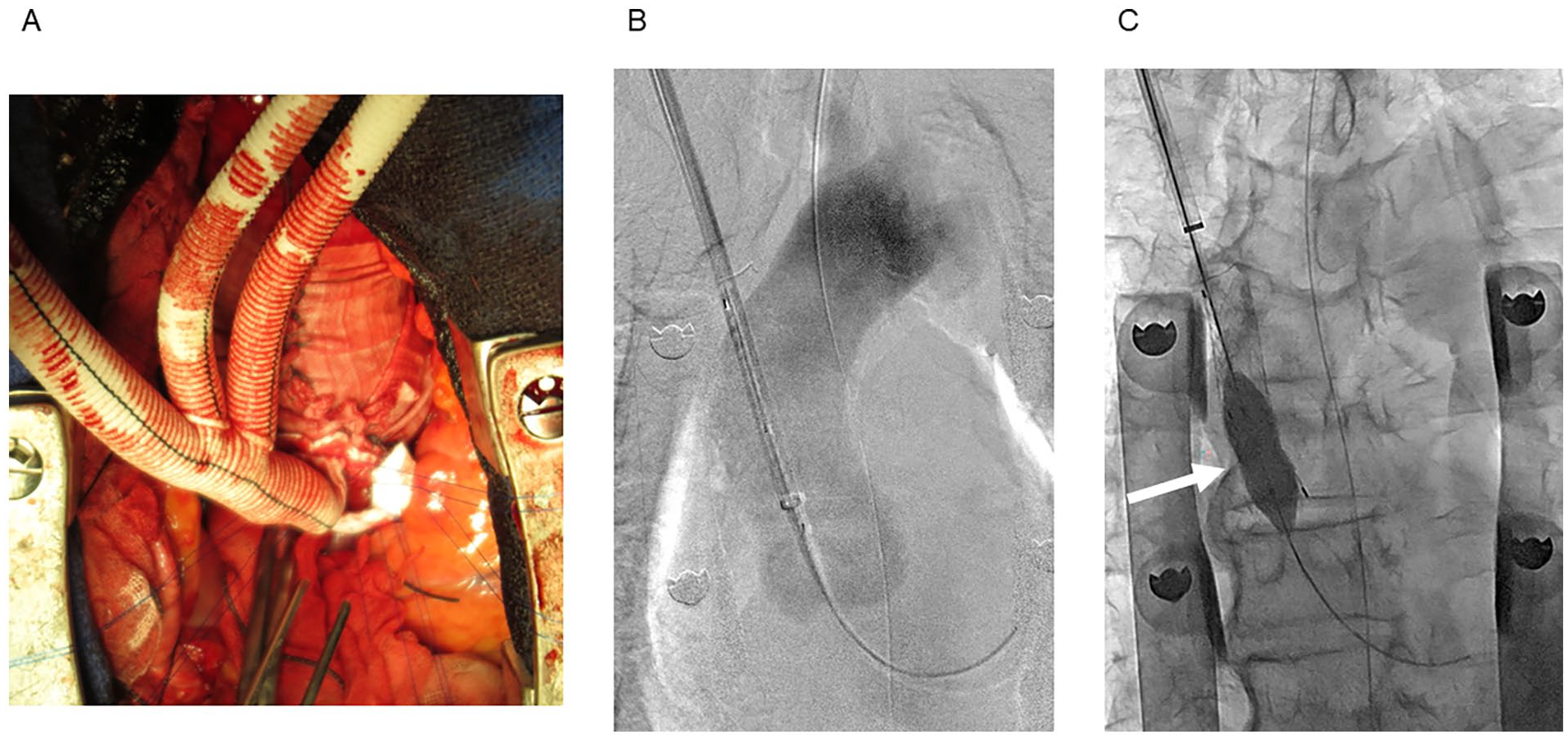
Intraoperative images of the “real chimney” technique. (A) Six mattress sutures were inserted between the ascending aorta and the triple-branched bypass graft clamplessly. (B) Stent graft (leg extension of the Gore Excluder; W. L. Gore and Associates, Inc) insertion from the center of the anastomosis oval through the oblique-cut triple-branched graft. (C) Balloon dilation was performed using a percutaneous transluminal angioplasty balloon (12 mm in diameter) to dilate the anastomotic hole in the ascending aorta as well as the area between the stent graft and the main trunk of the branched supra-aortic bypass graft. The anastomotic site of the chimney is indicated by a white arrow.
A percutaneous transhepatic cholangiography drainage needle (Medikit, Miyazaki, Japan) was used to puncture the center of the anastomosis oval through the puncture site of the branched graft, and an extra-stiff guidewire (Cook Medical, Bloomington, Indiana) was inserted against the aortic valve under fluoroscopic guidance. To ensure the needle remained centered, we punctured the middle of the oval under direct sight before tightening the 6 mattress sutures. The needle point at the ascending aorta was dilated using an 8 mm percutaneous transluminal angioplasty balloon and a 12F sheath was inserted through it. Leg extension of Gore Excluder (PXL161407 or PLC161407; W. L. Gore and Associates, Inc) was inserted 2 cm into the aorta, with the remaining 5 cm in the main trunk of the branched graft (Figure 2B).
Balloon dilation was repeatedly performed using a percutaneous transluminal angioplasty balloon (12 mm in diameter) to dilate the anastomotic hole in the ascending aorta as well as the area between the endograft and the main trunk of the branched supra-aortic bypass graft (Figure 2C). Distal anastomosis to the supra-aortic trunks (brachiocephalic, left carotid, and left subclavian arteries) was then performed using conventional techniques. After bypass grafting of the supra-aortic trunks, TEVAR was performed from the area just distal to the ascending anastomosis of the triple-branched bypass graft (the “real chimney” graft) to the descending aorta using a Gore conformable TAG (C-TAG) thoracic endoprosthesis (W. L. Gore and Associates, Inc) or Medtronic VALIANT thoracic stent graft (Medtronic, Santa Rosa, California). The procedure was performed in a hybrid operating room equipped with a C-arm. Excluder leg insertion and TEVAR were performed under fluoroscopic guidance. Intravascular ultrasound (IVUS) examinations were performed routinely to decrease contrast agent usage and determine the stent graft and proximal and distal landing zone sizes for TEVAR.
Definitions
Patients were defined as current smokers if they had smoked within 1 month before surgery. The operation was considered emergent if performed immediately after admission and urgent if performed within 24 hours after admission.
Imaging evaluation for postoperative stroke was performed if the patient was at high risk due to the presence of severe atherosclerotic arch lesions or any suspicious postoperative symptoms. Prolonged ventilation was defined as the inability to extubate within 48 hours after surgery. Wound delay was defined as any tissue loss that occurred within 2 weeks after surgery. Outcomes were defined as “early” (during admission or within 30 days after surgery); otherwise, they were defined as “midterm.” Postoperative renal failure was defined as a 50% decrease or a >2.0 increase in serum creatinine compared with the patient’s baseline levels.
Follow-up
Patients were followed-up in our outpatient clinic every 3 months within the first year after surgery and every 6 months thereafter. Imaging surveillance was performed using plain computed tomography (CT) and ultrasonography. Contrast-enhanced CT was performed during admission when possible.
Statistical Analysis
Continuous variables were presented as mean±standard deviation, whereas categorical variables were presented as frequencies or percentages. Statistical analyses were performed using JMP Pro 16 software (SAS Institute Japan, Tokyo, Japan).
Results
Baseline Characteristics
Sixty-one patients were treated between January 2014 and June 2022. The patient characteristics are shown in Table 1. The mean age was 75.1±6.5 years, and there were 51 men (83.6%). Nine non-smokers (18.0%), 34 ex-smokers (68.0%), and 7 current smokers (14.0%); the smoking status of 11 patients was unknown. Seventeen (27.9%) and 19 (31.1%) patients had histories of coronary artery disease and stroke, respectively. Eighteen patients (29.5%) had undergone previous aortic surgery. Thirty patients (49.2%) had chronic obstructive pulmonary disease (COPD). The mean eGFR was 51.6±24.4 mL/min/1.73 m2; 28 patients (45.9%) had mild-to-moderate chronic kidney disease (CKD; 30 mL/min/1.73 m2≤ eGFR<60 mL/min/1.73 m2), and 11 patients (18.0%) had severe CKD (eGFR<30 mL/min/1.73 m2). Three patients (4.9%) were undergoing regular dialysis. Thirty-three patients (54%) were transferred to facilities with cardiothoracic surgery departments.
Patient Characteristics.
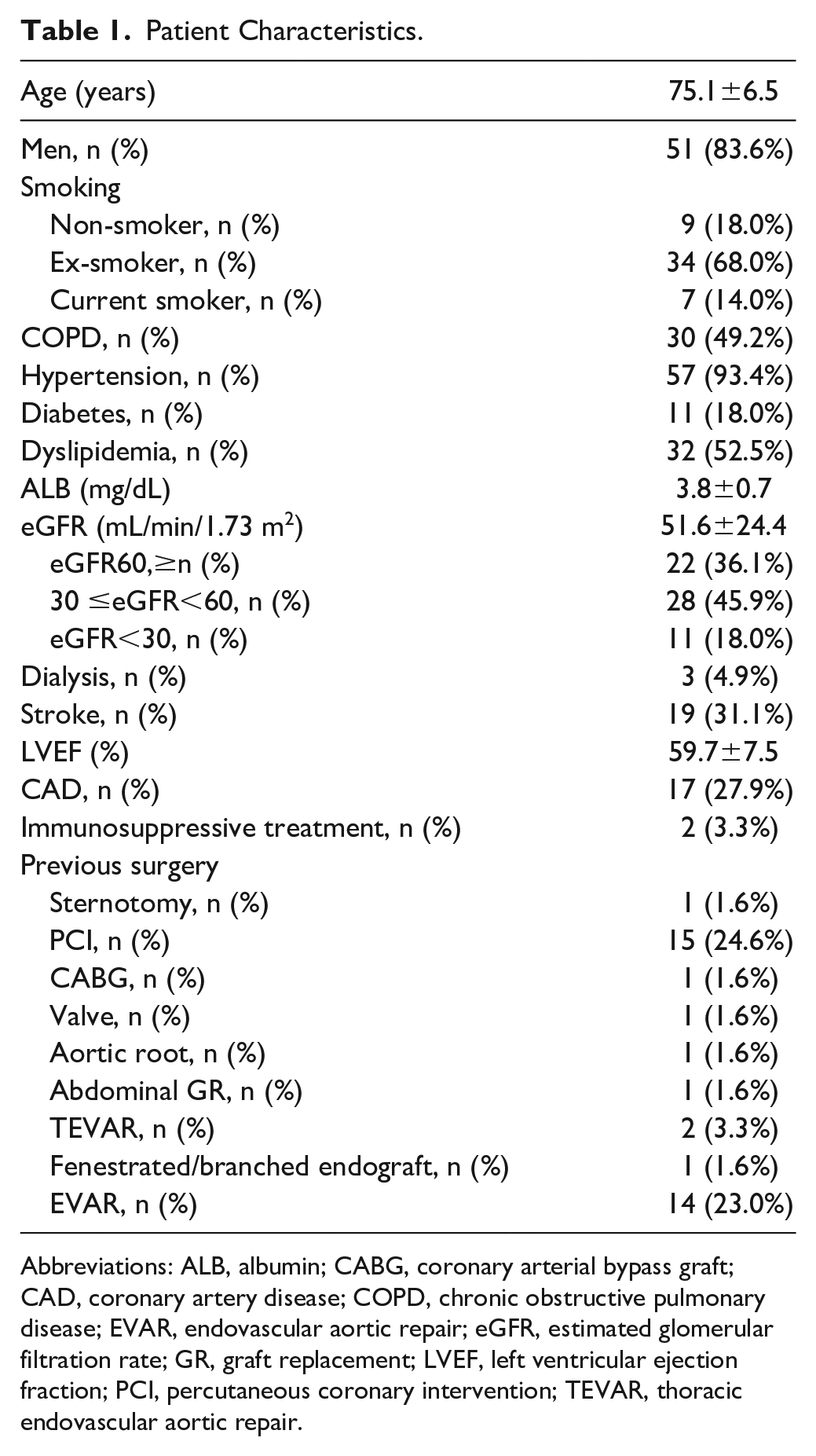
Abbreviations: ALB, albumin; CABG, coronary arterial bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; EVAR, endovascular aortic repair; eGFR, estimated glomerular filtration rate; GR, graft replacement; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary intervention; TEVAR, thoracic endovascular aortic repair.
Anatomical and Procedural Details
Anatomical and procedural details are presented in Table 2. The mean operative time and bleeding volume were 379±75 minutes and 627±639 mL, respectively. The mean amount of contrast agent used was 32.2±26.2 mL. The observed aortic pathologies were thoracic aortic aneurysm (TAA; n=55 [90.2%]), type B aortic dissection (n=3 [4.9%]), and post-dissection aneurysm (n=3 [4.9%]). Ruptured and infectious TAA were observed in 4 patients (6.6%) and 1 patient (1.6%), respectively. The mean aneurysmal diameter was 63.7±12.9 mm. The distribution of aneurysmal proximal zones is shown in Table 2. The mean diameter of the proximal landing zone was 36.2±4.4 mm. Banding of the ascending aorta was performed in 60 cases (98.3%); the mean banding diameter was 34.1±2.4 mm. Reconstruction of the left subclavian artery was performed by the simultaneous bypass to the supra-aortic arteries in all cases, with preoperative occlusion, surgical closure, and coil embolization performed in 1 (1.6%), 55 (90.2%), and 5 (8.2%) cases, respectively. The implanted devices were Alpha, C-TAG, and VALIANT in 1 (1.6%), 58 (95.1%), and 2 (3.3%) cases, respectively. In all cases, surgery was performed using an open approach to the access artery (mostly the femoral arteries [98.4%]).
Anatomical and Operative Details.
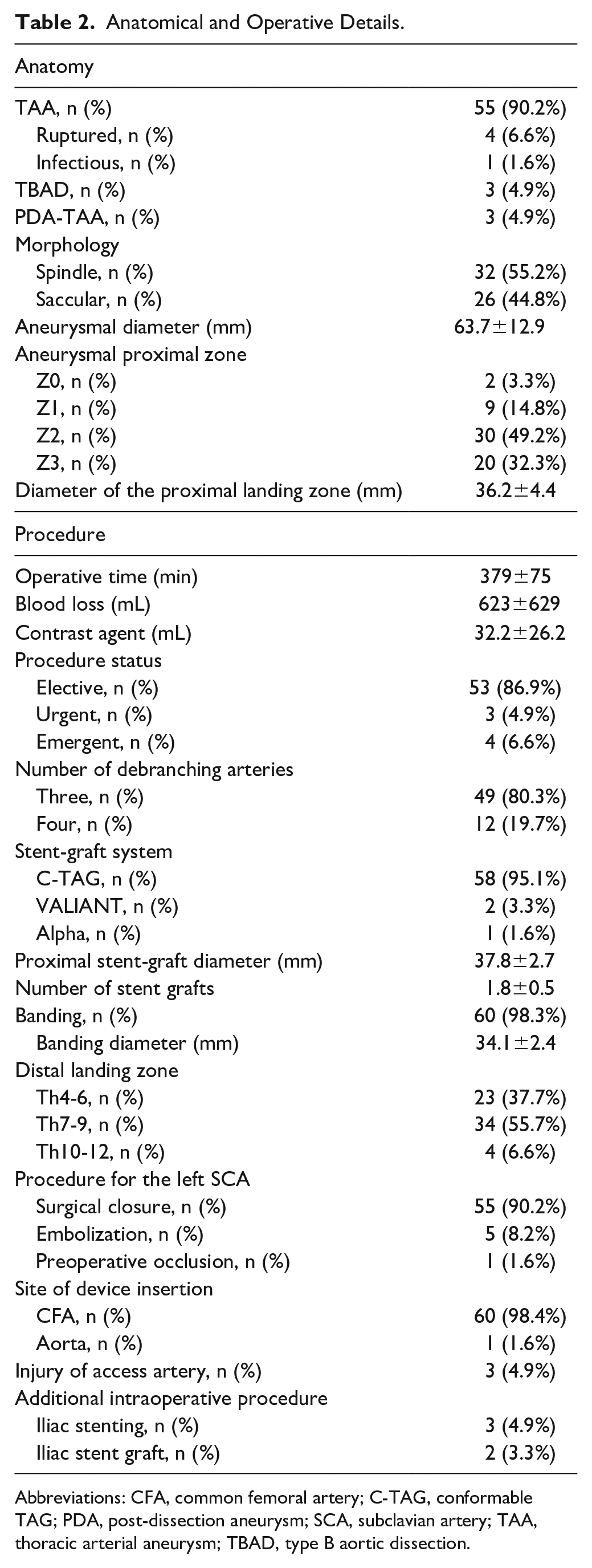
Abbreviations: CFA, common femoral artery; C-TAG, conformable TAG; PDA, post-dissection aneurysm; SCA, subclavian artery; TAA, thoracic arterial aneurysm; TBAD, type B aortic dissection.
Postoperative Outcomes
Postoperative outcomes are presented in Table 3. Regarding early outcomes, 30-day mortality and anastomosis-related problems affecting the ascending aorta or supra-aortic trunks were not observed. Cerebral magnetic resonance imaging was performed if cerebral symptoms were noted. Five (8.5%), 1 (1.6%), and 4 (6.6%) patients presented with permanent stroke (modified Rankin scale score≥ 2), permanent paraplegia, and permanent paraparesis, respectively. Four patients (6.6%) developed postoperative renal failure and required permanent hemodialysis. Respiratory complications were observed in 4 cases of prolonged mechanical ventilation (6.6%) and 5 cases of tracheostomy (8.2%).
Postoperative Outcomes.
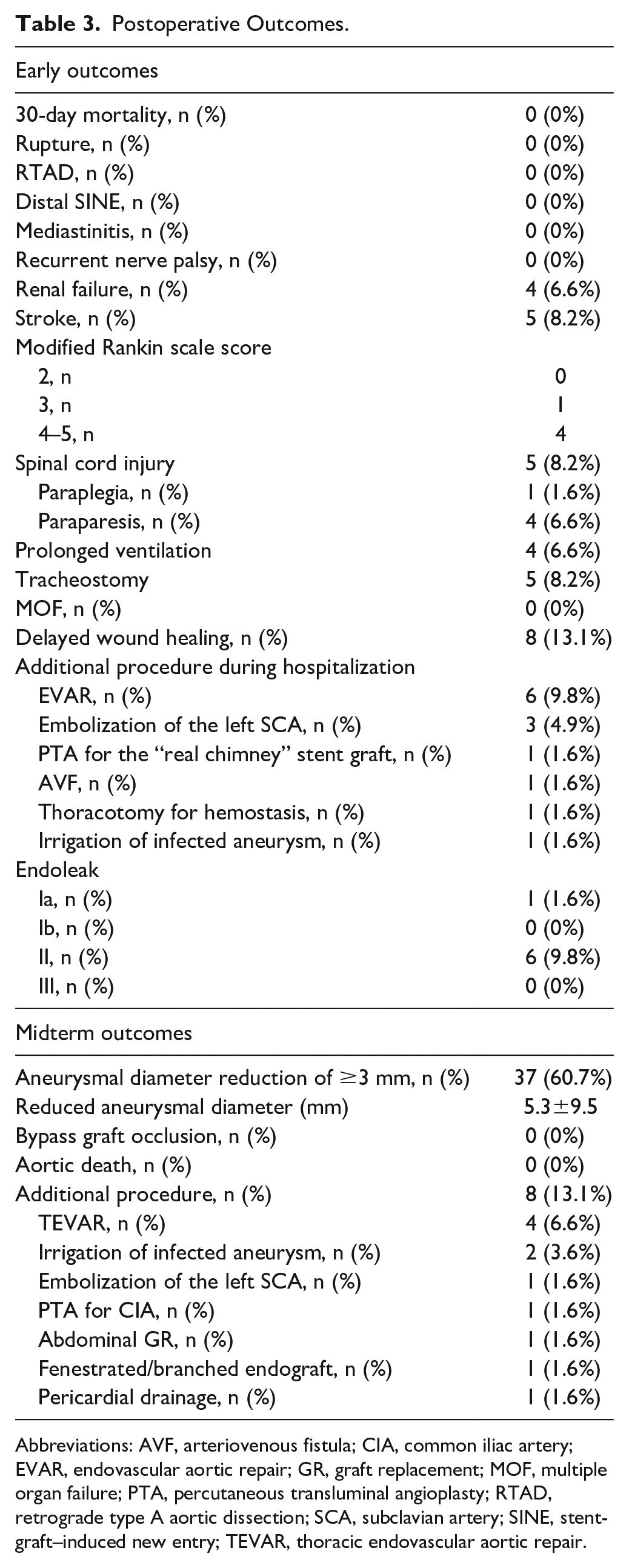
Abbreviations: AVF, arteriovenous fistula; CIA, common iliac artery; EVAR, endovascular aortic repair; GR, graft replacement; MOF, multiple organ failure; PTA, percutaneous transluminal angioplasty; RTAD, retrograde type A aortic dissection; SCA, subclavian artery; SINE, stent-graft–induced new entry; TEVAR, thoracic endovascular aortic repair.
Bypass graft occlusion and aortic death were not observed as midterm outcomes. An additional procedure for managing stenosis of the anastomosis site was required in only 1 case. One case of type Ia postoperative endoleak (EL; 1.6%) was noted, and the patient was managed with proximal endograft insertion. There was 1 case of type Ib EL as well, which was managed with distal endograft insertion. Furthermore, 6 cases of type II EL (9.8%) were noted; 2 patients were managed with embolization of the subclavian artery.
During follow-up, aneurysm shrinkage of >3 mm occurred in 37 patients (60.7%). The mean reduction in the aneurysmal diameter was 5.3±9.5 mm.
Survival Analysis
Kaplan-Meier curves were drawn for overall survival (OS), aneurysm-related survival (ARS; Figure 3), and aortic event-free survival (AEFS; Figure 4). The standard errors at 9 years were 0.0936, 0.0435, and 0.901 for OS, ARS, and AEFS, respectively.
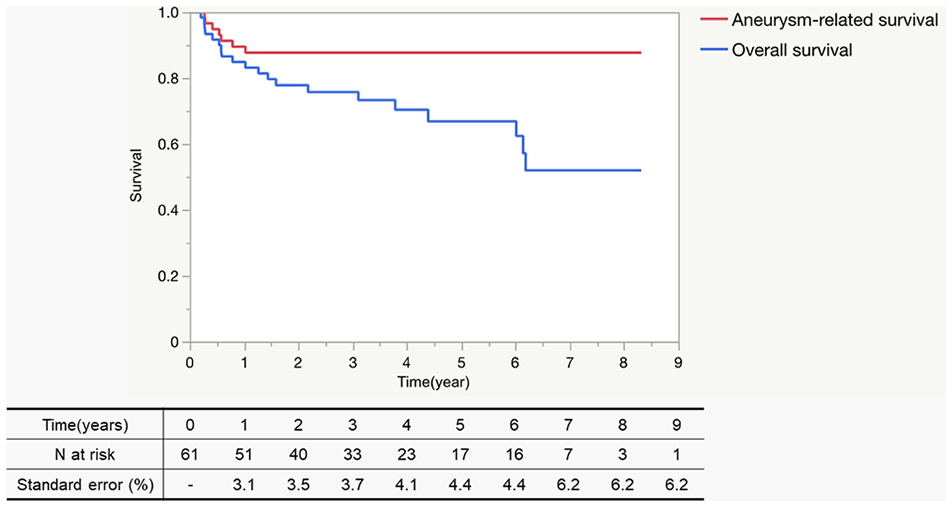
Overall and aneurysm-related survival. The 9-year overall and aneurysm-related survival after total debranching thoracic endovascular aneurysm repair with the “real chimney” technique. The standard errors at 5 years were 0.0936 and 0.0435 for overall survival and aneurysm-related survival, respectively.
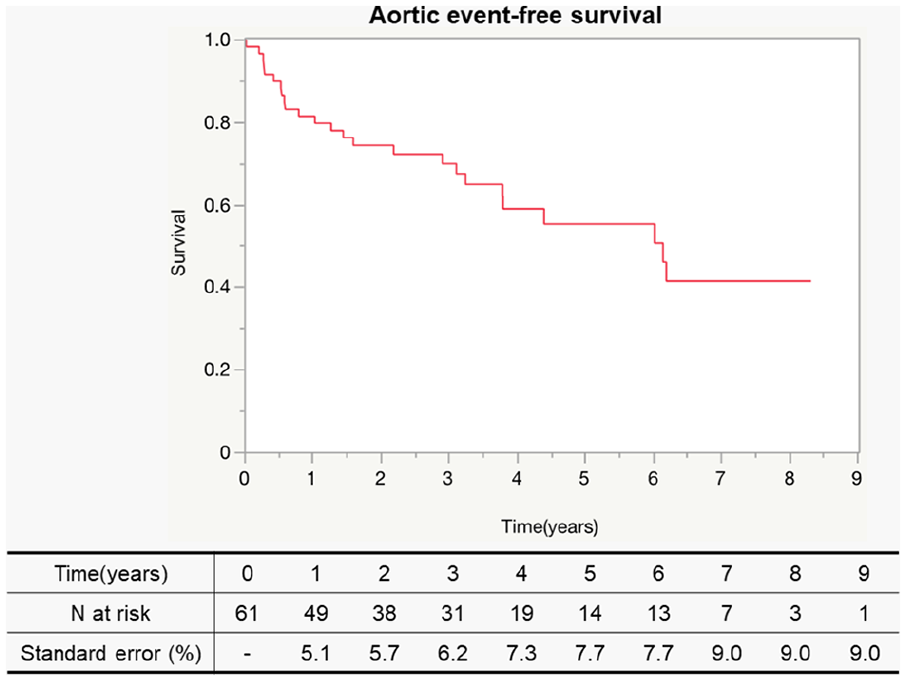
Aortic event-free survival. The diagram shows the 9-year aortic event-free survival after total debranching TEVAR with the “real chimney” technique. The standard error at 5 years was 0.0901. TEVAR, thoracic endovascular aortic repair.
The median follow-up period was 40.5±28.5 months. The postoperative survival rates at 1, 3, and 5 years were 84.9%, 75.7%, and 66.8%, respectively. Aortic death occurred in 2 cases, attributed to thoracic endograft infection in 1 case (1.6%) and aortoesophageal fistula in the other (1.6%).
Discussion
The outcomes of total debranching TEVAR using the “real chimney” technique are encouraging for patients with aortic arch pathologies who are at high risk for open repair. Most studies on TAR or conventional total debranching TEVAR included patients with a median age of <70 years5,6,11 –16; this study included comparatively older patients. Older patients with lower cardiac and/or respiratory function are potential candidates for this procedure. In addition, this study included more smokers and patients with COPD. This study was presumed to have included more frail patients, which had to be considered when interpreting the findings. According to previous studies, the incidence of early mortality after TAR or conventional total debranching TEVAR is 3.4% to 8.2%16 –19 and 0% to 29.6%,20 –23 respectively. Although 1 study revealed extremely high mortality after total debranching TEVAR, a recent systematic review revealed that the 30-day mortality rate after zone 0 TEVAR was 7.49%. 24 Conventional arch TEVAR with a more proximal landing zone reportedly involves greater risks of cerebral stroke7,8 and RTAD, 9 and total debranching zone 0 TEVAR supposedly bears the greatest risk for both. The reported risk of RTAD after zone 0 TEVAR is yet to be determined and ranges from 0% 25 to 17.9%; 26 however, a recent systematic review estimated it to be 5.72%. 24 With such high mortality and morbidity rates, conventional hybrid arch repair techniques require further improvement.
Despite our patients’ high-risk status, this study demonstrated that total debranching TEVAR with the “real chimney” technique is safer than TAR and conventional total debranching TEVAR (based on the absence of early mortality). Furthermore, this novel approach is favorable as no cases of RTAD were noted. There was only 1 case where a C-TAG insertion was required for the Type Ib EL secondary to a perigraft infection. Despite the interventions, the patient was transferred to another general hospital but died soon after transfer.
This study also revealed that all the included patients had high-risk morbidities, such as a history of stroke, coronary artery disease, or aortic surgery, and that more than half of the study patients (54%) were referred to our institution from other facilities with departments of cardiovascular surgery, suggesting that a considerable number of patients with aortic arch pathologies may be at extremely high risk for conventional open surgery. Considering the fragility of these patients and the presence of severe atherosclerotic disease, outcomes such as stroke or spinal cord injury (SCI) are likely.
Although many techniques have been developed for performing aortic repair, conventional TAR still requires ECC, which is very invasive in patients at a high risk for open repair. Hybrid arch repair is less invasive than TAR.13 –15,27,28 It is classified into 3 types; 29 all cases of type II and III hybrid arch repairs require ECC, 30 although some facilities also use ECC for type I procedures. Even in cases where a type I arch hybrid repair is performed without ECC, virtually all cases involve partial clamping of the ascending aorta, which carries a greater risk for brain complications due to emboli originating from the plaque-rich aortic wall 14 and aortic wall injury and dissection. 13 Clamping of the ascending aorta has been suggested to be the leading cause of RTAD.15,21,31,32 Side clamping involves a wide area, including the distal ascending plaque-rich aorta, and does not result in sufficiently large proximal landing zones. To reduce complications arising from side clamping of the ascending aorta and to achieve a longer proximal landing zone, the presented novel “real chimney” technique for the repair of aortic arch pathologies was developed. This breakthrough technique requires neither ECC nor partial aortic clamping. The manipulated area was limited to a small plaque-free area of the ascending aorta; endovascular devices were inserted into the proximal ascending aorta (which contained less plaque) instead of the distal ascending aorta. Longer proximal landing zones can be guaranteed without clamping sites.
No complications related to the “real chimney” technique were noted, except for 1 case of anastomotic stenosis that was successfully treated with the addition of an endograft. This case occurred because the real chimney endograft was inserted more than 2 cm into the aorta. The inner orifice of the endograft got too close to the aortic wall, resulting in pressure loss. An additional endograft was inserted toward the distal. It is crucial not to insert the real chimney stent graft more than 2 cm into the aortic lumen. Stitching of the ascending aorta from the outer surface is speculated to cause dissection of the arterial 3-layer structure; however, no aortic complications were observed in our study. This indicates that total debranching with the “real chimney” technique is safe for anastomosis.
The proximal landing zone diameter is always a cause for concern because of the risk of future dilation and type Ia endoleak. Although we did not always perform banding of the ascending aorta before 2015, almost all the patients in this study underwent banding. We now consider banding even in cases with an ascending aorta diameter <37 mm to ensure that the diameter is as small as possible. Banding of the ascending aorta, which is extensively secured by the “real chimney” technique, provides a firmer and more durable proximal connection for the stent graft. Accordingly, only 1 case of a type Ia endoleak was observed in this study. A failed arch TEVAR due to an insufficient proximal landing zone is difficult to treat postoperatively; therefore, these 2 innovations at the proximal landing site are valuable. The postoperative reduction in the aneurysmal diameter observed in most cases indicates the efficacy of this procedure.
In addition, because many patients in this series had renal dysfunction, the use of contrast media was limited to a minimum by the extensive use of IVUS. Intravascular ultrasound has the added benefit of allowing the diameter of the banded proximal landing zone to be remeasured before stent-graft implantation. We chose the device size following the instructions for use.
Limitations
Due to the single-center retrospective cohort design of this study, our decision-making process may not be generalized, and selection bias cannot be ruled out. Further studies are required to establish additional clinical evidence for this procedure.
Conclusions
Our novel “real chimney” technique for total debranching TEVAR proved effective in patients at high risk of open repair for aortic arch pathologies. Further technique refinements will be made to reduce serious complications such as stroke or SCI, as well as further evidence of the safety and effectiveness of this technique.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval/Informed Consent
This study was performed after obtaining approval from the Morinomiya Hospital Institutional Review Board and individual informed consent from the participants.