
Abstract
Objectives:
This study sought to establish the cost-effectiveness of endovascular thrombectomy (EVT) in M2 occlusions compared with patients who did not have EVT using both real-world and clinical trial evidence.
Methods:
The effectiveness of EVT in M2 occlusions was informed by the International Stroke Perfusion Imaging Registry (INSPIRE, real-world data for a wide range of strokes) and HERMES collaboration, trial data. Patients who received EVT and non-EVT treatment from INSPIRE were matched according to baseline characteristics. A Markov model with 7 health states defined by the 3-month modified Rankin scale (mRS) was constructed. Endovascular thrombectomy and non-EVT-treated patients in real-world, and clinical trials were run through the Markov model separately to generate the results from a limited societal perspective. National statistics and published literature informed the long-term probability of recurrent stroke, mortality, costs of management post-stroke, non-medical care, and nursing home care.
Results:
A total of 83 (42 EVT and 41 non-EVT) patients were matched of 278 (45 EVT and 233 non-EVT) patients in INSPIRE who had M2 occlusion stroke at presentation. The long-term simulation estimated that offering EVT to M2 occlusion stroke patients was associated with greater benefits (5.48 EVT vs 5.24 non-EVT quality-adjusted life year [QALY]) and higher costs (A$133 457 EVT vs A$126 127 non-EVT) compared with non-EVT treatment in real-world from a limited societal perspective. The incremental cost-effectiveness ratio (ICER) of EVT in real-world was A$29 981 (€19 488)/QALY. The analysis using the data from HERMES collaboration yielded consistent results for the EVT patients. Comparison with real-world cost-effectiveness analyses of EVT in internal carotid artery/middle cerebral artery-M1 (ICA/MCA-M1) occlusion suggested a potential reduced QALY gains and increased ICER in M2 occlusions.
Conclusions:
Our study suggested that the benefits gained from EVT in M2 occlusion stroke in the real-world were similar to that derived from the clinical trials. The clinical and cost benefits from EVT appeared to be reduced in M2 compared with that from the ICA/MCA-M1 occlusions.
Clinical Impact
Our study has provided valuable insights into the clinical significance of endovascular therapy (EVT) in the context of M2 occlusion stroke within a real-world setting. It is noteworthy that our findings indicate that the benefits obtained from EVT in M2 occlusion stroke closely align with those observed in controlled clinical trials. However, it is essential to recognize that there is a reduction in the clinical and cost-related advantages when comparing M2 occlusions to more proximal ICA/MCA-M1 occlusions.
Introduction
While the most recent American Heart Association (AHA) guidelines recommend endovascular thrombectomy (EVT) for patients with causative occlusion of the internal carotid artery (ICA) or proximal middle cerebral artery (MCA) M1 segment (class 1; level of evidence A), the benefits of EVT remain incompletely defined for MCA M2 segment occlusions (class 2b; level of evidence B-R). 1 The limited evidence for M2 occlusions may be due to the exclusion of these patients in the majority (5 of the 7) of the pivotal randomized controlled trials (RCTs) except for MR CLEAN and EXTEND-IA. However, meta-analysis of patient-level data from the Highly Effective Reperfusion Using Multiple Endovascular Devices (HERMES) collaboration comprising 7 RCTs has reported favorable treatment effects of mechanical thrombectomy over standard of care in patients with M2 occlusions, adjusted odds ratio, aOR=2.39, 95% CI=1.08 to 5.28, p=0.03 for 90-day modified Rankin scale (mRS) outcome of 0 to 2. 2 The result was consistent with a previous meta-analysis of 12 non-randomized studies, which indicated that compared with M1 occlusions, EVT was associated with similar recanalization rates, better 90-day mRS outcome of 0 to 2 and potentially reduced mortality in patients with isolated M2 occlusions. 3 Nevertheless, compared with M1 and ICA occlusions, patients with an M2 occlusion have substantially higher rates of good and excellent functional outcomes with thrombolysis alone. Therefore, it is reasonable to expect that the cost-effectiveness of EVT in M2 occlusion may be less favorable than more proximal large vessel occlusions (LVOs).
Though EVT for stroke patients with M2 occlusions may be beneficial and may be currently practiced in clinical care, its cost-effectiveness has not been corroborated with real-world evidence. To our knowledge, there was only one economic evaluation specific to M2 occlusions using clinical trials’ data. The economic analysis was based in the US setting, comparing EVT with standard care using data from the HERMES collaboration. 4 In this analysis, EVT was found to be not cost-effective over the short term (90 days) with an incremental cost-effectiveness ratio (ICER) of US dollar (USD) 678 003/quality-adjusted life year (QALY) (valued in 2020 USD), but was dominant (lower cost and more effective) over the long term (lifetime). Another economic evaluation based in the United States that reported on a subgroup of patients with M2 occlusions found that this subgroup was the least cost-effective (out of ICA, M1, and M2 occlusion subgroups) with an ICER of USD28 812/QALY (valued in 2015 USD) over a time horizon of 30 years. 5 While this may be considered an acceptable ICER (under the willingness-to-pay of USD 50 000/QALY), probabilistic sensitivity analysis (PSA) results indicated a suboptimal acceptability rate of 59.4%, rendering its cost-effectiveness uncertain. 5
While previous economic evaluations have been performed for the United States, differences in costs and structure of the health system mean that the results may not apply to the Australian setting. Taking advantage of data from the International Stroke Perfusion Imaging Registry (INSPIRE), our study aimed to (1) determine the interim cost-effectiveness of EVT in patients with M2 segment occlusions in Australia using both real-world and clinical trial evidence and (2) compare the benefits of EVT in M2 occlusions using trial and real-world populations.
Methods
Study Population
Real-world population
Data from the INSPIRE (over 20 centers from 4 countries with >4000 patients) were used to source baseline, imaging data, and 90-day clinical outcome over a 6-year period (2015–2019) 6 (Supplementary Material). A proximal vessel occlusion was defined as an occlusion located in the first half of a M2 branch, while a distal occlusion was defined as an occlusion in the second half of the M2 branch based on the computed tomography/magnetic resonance imaging (CT/MRI). The location of the vessel occlusion was also confirmed by a study radiologist independent from the site. However, INSPIRE registry did not sufficiently document the location of the M2 occlusion. Eligibility for EVT in routine clinical practice included the presence of a vessel occlusion, ICA, proximal posterior cerebral artery, middle cerebral artery, and anterior cerebral artery (PCA, MCA, and ACA, respectively), intracranial vertebral artery (VA), and/or basilar artery (BA) with a significant clinical deficit7–10 that the interventionalist could potentially retrieve. Patients were treated according to the local clinician’s discretion and protocols.
Patients were split into 2 groups: those who received EVT and those who did not. Patients in the 2 groups were then matched on a one-to-one ratio based on age, sex, baseline National Institutes of Health Stroke Scale (NIHSS) and computed tomography perfusion (CTP) ischemic core and penumbra volume using the “psmatch2” command from Stata (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC) (Stata codes provided in Supplementary Material). In consultation with the clinician (MP), NIHSS was selected as the key indicator to determine the appropriateness of the matched cohorts. Premorbid mRS was insufficiently recorded in the INSPIRE thus was not incorporated in the matching process. The sociodemographic and clinical characteristics of the simulated cohort were defined by matched participants from the INSPIRE (summarized in Table 1).
Baseline Characteristics of the Matched Cohorts From INSPIRE and HERMES.
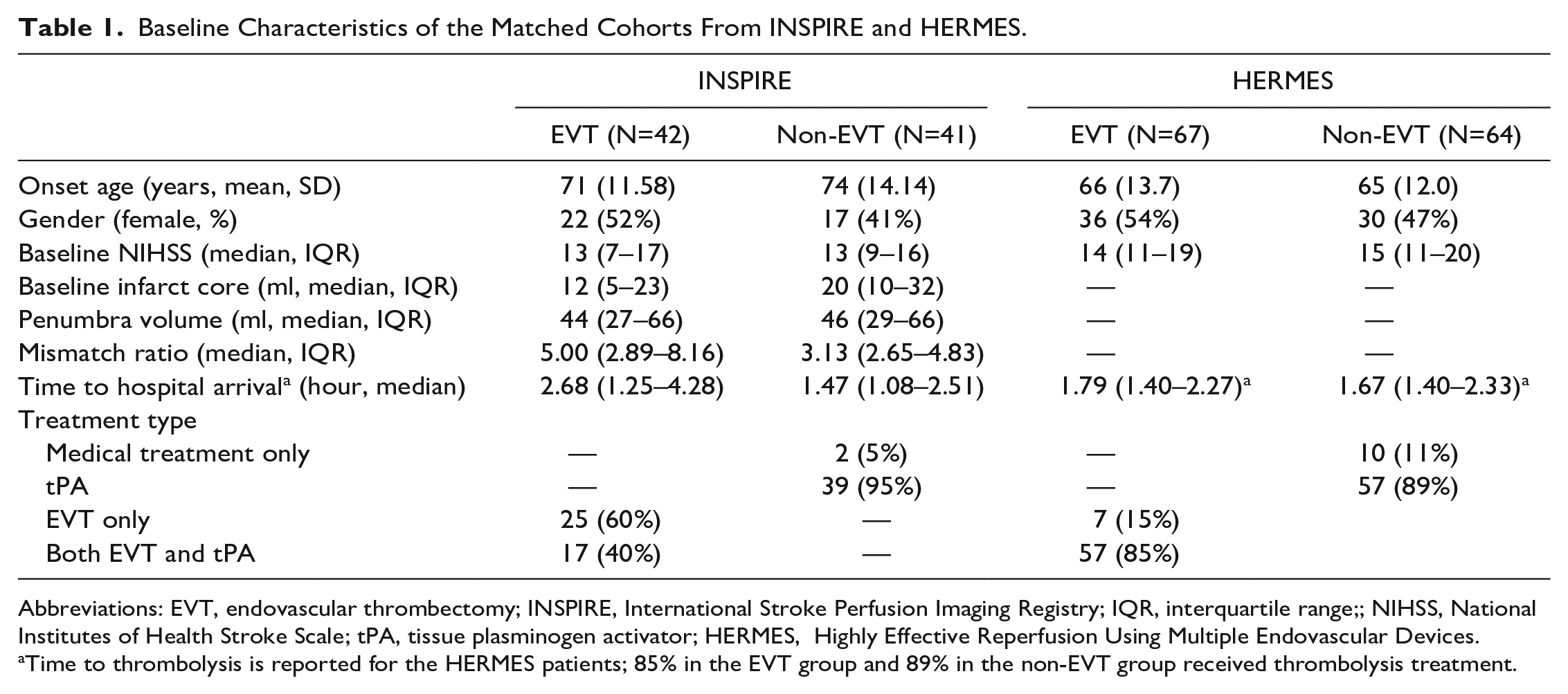
Abbreviations: EVT, endovascular thrombectomy; INSPIRE, International Stroke Perfusion Imaging Registry; IQR, interquartile range;; NIHSS, National Institutes of Health Stroke Scale; tPA, tissue plasminogen activator; HERMES, Highly Effective Reperfusion Using Multiple Endovascular Devices.
Time to thrombolysis is reported for the HERMES patients; 85% in the EVT group and 89% in the non-EVT group received thrombolysis treatment.
The distribution of propensity scores after matching by EVT status is shown in Supplementary Figure 2.
Clinical trial participants
The HERMES collaboration consists of 7 RCTs (MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, THRACE, EXTEND IA, and PISTE). The patient-level data from each trial, including CTA or MR angiography, were pooled to extract the patients with M2 occlusions. It was reported that the subject count by the trial was MR CLEAN (n=46), ESCAPE (n=18), EXTEND-IA (n=9), SWIFT PRIME (n=24), REVASCAT (n=21), PISTE (n=4), and THRACE (n=8). 2 The detailed results of the meta-analysis are reported by Menon et al. 2
Simulation model
A Markov microsimulation model was constructed to simulate the long-term health outcomes and costs of EVT versus medical treatment alone in LVO stroke due to M2 occlusion. Markov microsimulation was selected over Markov cohort model because it allows for the memory of events (eg, recurrent stroke). Briefly, there were 7 Markov states representing 7 mRS scores (0–6) plus an absorbing state for all other causes of death. The initial status of patients in the model was their health state at day 90 as determined by their mRS score. Given significant risk of stroke recurrence (5 years cumulative incidence around 20%) 11 , we modeled for the possible changes in mRS score post a recurrent stroke. This model has been used in previous publications assessing the cost-effectiveness of EVT in LVO stroke. 4 The long-term modeling was conducted using TreeAge software (Williamstown, MA, USA). The model structure is shown in Supplementary Figure 1.
Inputs for Long-Term Simulation
Transition probabilities
The annual risk of recurrent stroke was the same in both comparison groups, but the occurrence of recurrent incidents was adjusted (ie, experiencing a recurrent stroke increases the risk of a subsequent event). The number of patients starting the long-term simulation at each of the 6 health states was the only difference in transition probabilities between the trial-based and real-world-based arms (ie, mRS scores of 0–5; patients who died in the first 90 days were excluded from the long-term modeling, but their initial costs were included). Supplementary Table 1 summarizes the transition probabilities for trial-based and real-world-based arms. Dirichlet distribution (a multivariate generalization of the beta distribution for the percentage of each mRS score) was used in the PSA to examine the uncertainty in mRS outcome post-EVT or non-EVT treatment.
Costs
All costs related to health care, non-medical care, and formal care (ie, institutional care) were considered in the model (Supplementary Table 1). Productivity losses were not considered, given the limited societal perspective taken for the analysis and average age of the patients (over 70 years old predominantly). Hospitalizations, outpatient care (consultations, pharmaceuticals, and examinations), institutional care (for patients with mRS score 4 or 5), and non-medical care (including community services use, home modifications, special aids/equipment, and informal care) were among the costs associated with each health state, sourced from published literature. 12 All costs were valued in 2021 Australian dollars (1 AUD=0.65 Euro, 2021 average exchange rate). Cost parameters, including hospitalization for recurrent stroke, and initial and ongoing stroke management were assigned a gamma distribution with 10% SD to allow for variation in the sensitivity analysis.
Quality-adjusted life year
Utility weights are based on a 0-1 cardinal scale, with 0 denoting death and 1 denoting complete health (negative values represent a health state worse than death). Utility weights are preference weights representing the strength of desirability toward different health states (ie, more preferred health states will have greater weight). Published literature was used to inform utility weights associated with being in the post-stroke health states described by mRS score in the current study. The number of QALYs gained was calculated using utility weights. The utilities were elicited from EQ-5D-3L. A utility decrement was applied immediately following a recurrent event to account for the temporarily reduced quality of life after a stroke.13,14 The utility weights used are shown in Supplementary Table 1. All utility values were assigned a beta distribution with 10% SD to allow for variation in the sensitivity analysis.
Long-term cost-effectiveness analysis
In line with the submissions seeking public subsidy in Australia, a health care system perspective was taken for the base case analysis to assess the economic credential of EVT in stroke patients with M2 occlusion. In addition, a limited societal perspective was adopted to measure the broader (ie, nursing home care and non-medical) costs and benefits over a 13-year time horizon, given the average age of the simulated cohort (ie, over 71 years) and remaining life expectancy for general Australian (ie, 82.9 years).
To achieve robust simulation results, 10 000 Australian patients with M2 occlusion stroke were simulated in the base case (a small number of simulated patients rendering the results highly subjective to randomness). The total costs and QALY gained by corresponding groups were the key outcomes of the long-term simulation. Following the National Health Technology Assessment Agency’s advice, costs and benefits were discounted at a rate of 3% each year. 15 The choice criteria were set at the often-cited willingness to pay per QALY threshold of A$50 000. Given the Markov modeling technique adopted in the current study (no individual-level variability), we were unable to compute the p value for the difference in the modeled outcomes.
Sensitivity analyses
One-way deterministic sensitivity analyses (ie, varying one model parameter at a time within a plausible range if there is insufficient evidence) were undertaken to examine the robustness of base case results (Supplementary Table 1). In addition, PSAs, which determined the distribution of key uncertain parameters, were run to explore the results further. Sensitive variables identified in the one-way sensitivity analyses were further examined in the PSA by incorporating the distributional uncertainties. The parameters for the examined distributions in PSA are shown in Supplementary Table 2.
To further examine the potential treatment benefit from EVT in M2 occlusion, matched EVT and non-EVT patients with 24 hours, the thrombolysis in cerebral infarction (TICI) outcomes were analyzed separately. The 3-month mRS outcomes from patients who achieved TICI 2b/3 (representing successful recanalization) by treatment status (24 EVT vs 27 non-EVT patients) are shown in Supplementary Figure 3
Model validation
We tested face validity and validated the modeled results against empirical data. Furthermore, the extreme value testing by assuming the identical mRS 0 to 3 outcomes in EVT and non-EVT groups were performed to validate the results. Due to a lack of long-term data, particularly for patients with LVO stroke, long-term follow-up data for patients post-stroke was used to empirically validate the results from the modeling study.
Comparison with the real-world cost-effectiveness of EVT in ICA/MCA-M1 occlusions
Using the real-world INSPIRE data, we matched patients with ICA/MCA occlusion receiving EVT versus non-EVT employing the same Stata command described above. Running through the same simulation model, the cost-effectiveness of EVT in ICA/MCA-M1 occlusion was assessed. The only difference with the M2 occlusion model was the distribution of 3-month mRS outcomes by treatment status in ICA/MCA occlusion. The baseline characteristics of the matched patients are shown in Supplementary Table 3, and 3-month mRS outcomes are presented in Figure 1.
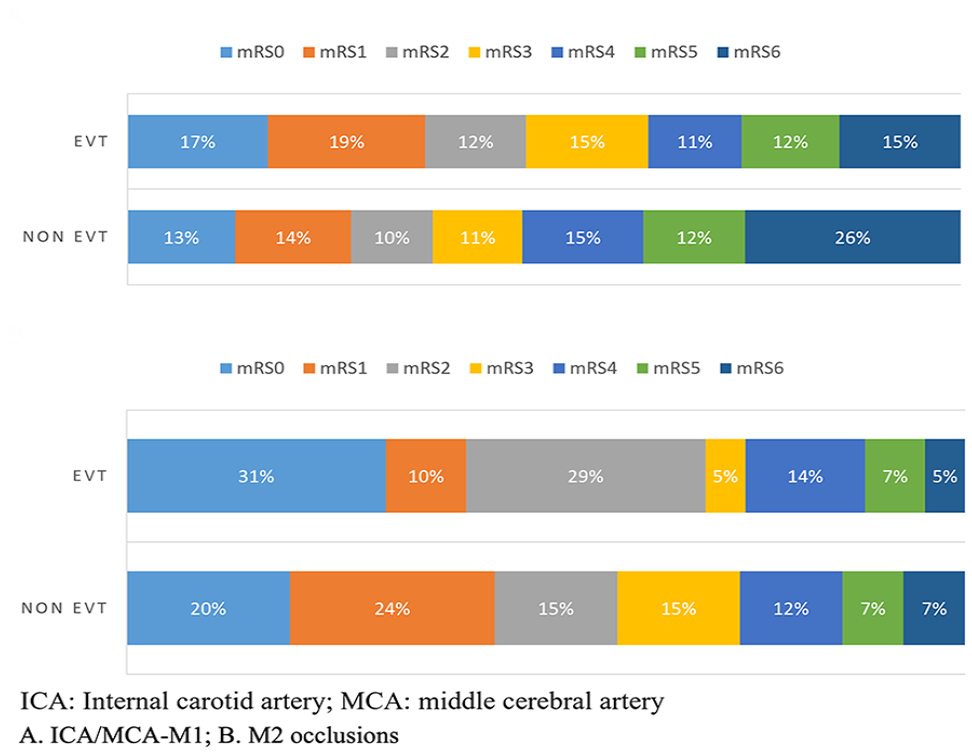
Three-month modified Rankin scale (mRS) outcomes from the matched International Stroke Perfusion Imaging Registry (INSPIRE) patients with M2 or internal carotid artery/middle cerebral artery-M1 (ICA/MCA-M1) occlusions. mRS, modified Rankin scale; EVT, endovascular thrombectomy.
Results
Real-World Population
A total of 83 (n=42 for EVT and n=41 for non-EVT) patients were matched of 278 (n=45 for EVT & n=233) patients in INSPIRE who had an M2 occlusion stroke at presentation (Table 2). Patients who could not be matched were mainly those with missing baseline NIHSS scores (N=3). Patient characteristics were closely matched between the EVT and non-EVT groups. However, patients from the non-EVT group generally had younger age, more males, and shorter time from onset to hospital arrival, compared with the EVT-treated patients. The 3-month mRS scores by treatment status for the matched patients are presented in Figure 1.
Cost-Effectiveness Results Using Both Real-World and Clinical Trial Evidence for M2 and ICA/MCA-M1 Occlusions.
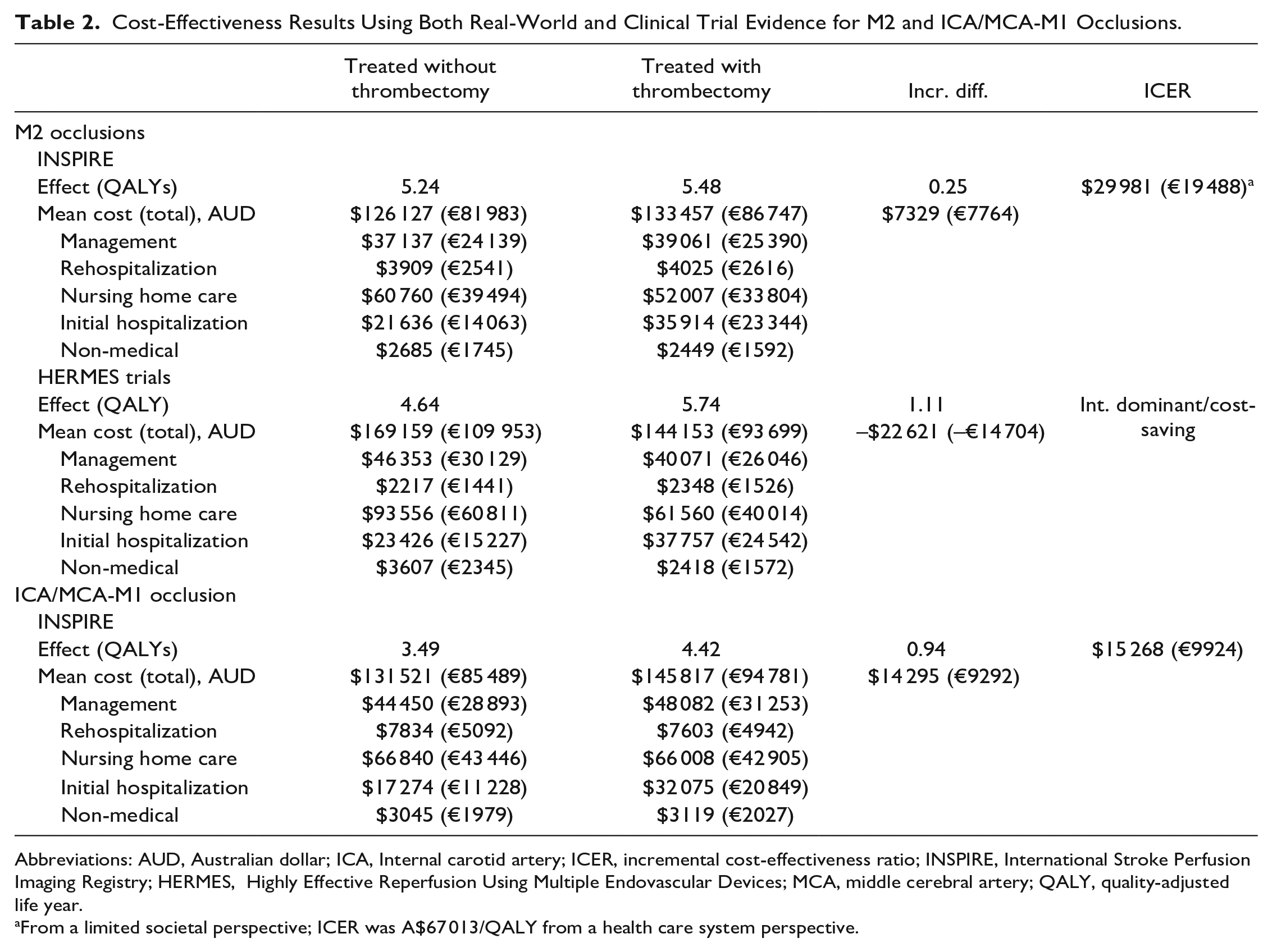
Abbreviations: AUD, Australian dollar; ICA, Internal carotid artery; ICER, incremental cost-effectiveness ratio; INSPIRE, International Stroke Perfusion Imaging Registry; HERMES, Highly Effective Reperfusion Using Multiple Endovascular Devices; MCA, middle cerebral artery; QALY, quality-adjusted life year.
From a limited societal perspective; ICER was A$67 013/QALY from a health care system perspective.
Clinical Trial Population
Of patients with M2 occlusion, a total of 67 patients received EVT, while 64 were randomized to the control group. The average age of the participants ranged from 65 to 66 years, with a median baseline NIHSS of 15 vs 14 in the EVT and non-EVT groups, respectively. Most of participants in both groups received thrombolysis (85.1% in the EVT vs 89.1% in the non-EVT group). 2
Long-Term Cost-Effectiveness Analysis
The long-term simulation estimated that offering EVT to M2 segment occlusion stroke patients was associated with greater benefits (5.48 VS 5.24 QALY gains), and higher costs (A$133 457/€ 86 747 EVT vs A$126 127/€81983 non-EVT), compared with non-EVT treatment. The incremental cost of the EVT procedure was mainly due to increased costs related to initial hospitalization (A$14 278/€9281), however, cost-saving from long-term non-medical care (–A$236/€153) and nursing home care (–A$8753/€5689) partially offset the incremental cost due to EVT. (Table 2).
The analysis using the data from HERMES collaboration yielded consistent results for the EVT patients while different results for the non-EVT patients (Table 2). Particularly, non-EVT patients in the HERMES trials obtained lower long-term QALY gains when compared with their counterparts from INSPIRE (4.64 vs 5.74 QALYs). The potential causes for such discrepancy may include the proportion of patients receiving thrombolysis (89% vs 95%), and others stroke-related characteristics that were not reported (advanced imaging determined volume of ischemic core and penumbra)
Comparison With the Real-World Cost-Effectiveness of EVT in ICA/MCA-M1 Occlusions
Our modeled cost-effectiveness analysis of EVT in ICA/MCA occlusion using INSPIRE real-world data indicated that EVT treatment led to greater costs and benefits (both QALYs and LY gains). Specifically, EVT was associated with an additional cost of A$14 295/€9292, and 0.94 QALY gained per patient treated (Table 2). Compared with the cost-effectiveness of EVT in M2 occlusion using INSPIRE data, the benefits from EVT were smaller in M2 occlusion than that of ICA/ICA occlusions (0.25 vs 0.94 QALY gains). Consequently, the ICER of EVT was lower in the ICA/MCA-M1 occlusion than in the M2 occlusion (A$15 268/€9924 vs A$29 981/€19 488), indicating more favorable cost-effectiveness.
Sensitivity Analysis
One-way deterministic sensitivity analysis suggested that cost of nursing home post-stroke (mRS 3), probability of recurrent stroke, and discount rate were the main drivers for the ICER. In comparison, ICER was less sensitive to the variations in the mortality post a recurrent stroke, cost of management post-stroke (first year, mRS 4 and 5), utility weight of mRS 4/5, and cost of non-medical care (mRS 4) for the INSPIRE based results (Supplementary Figure 4).
Probabilistic sensitivity analysis indicated that EVT had a probability of 100% being cost-effective when compared with non-EVT treatment for patients with M2 occlusion stroke [Figure 2 and Supplementary Figure 5, Supplementary Table 4) in the real-world. Additional threshold analyses are shown in Supplementary Figures 6 and 7.
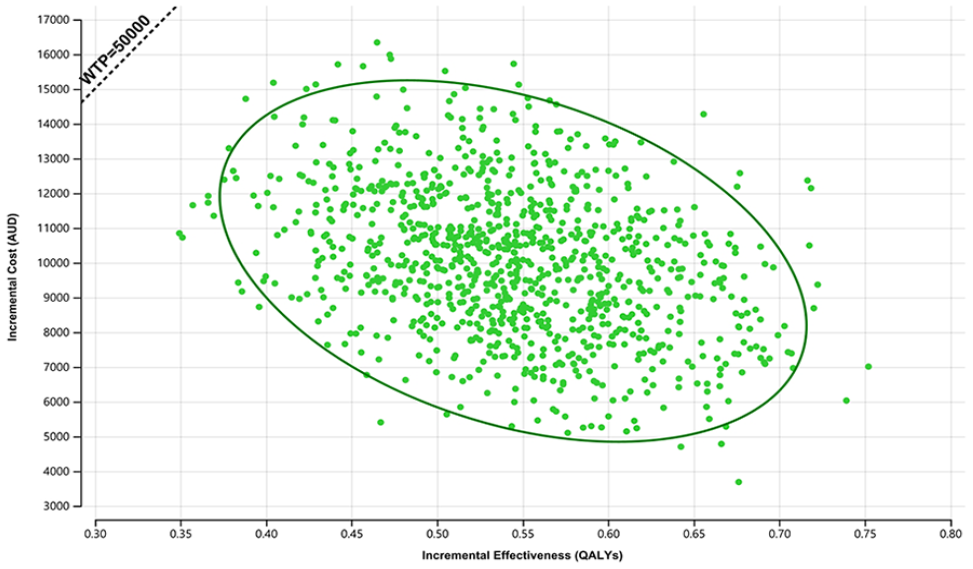
Results from the probabilistic sensitivity analysis showing the probability of endovascular thrombectomy (EVT) being cost-effective based on International Stroke Perfusion Imaging Registry (INSPIRE) patients. The dotted line represents the willingness to pay per quality-adjusted life year (QALY) threshold in Australia. The green dots suggesting the intervention being cost-effective while red dots showing the results being cost-ineffective. The eclipse is for the 95% confidence interval. WTP, willingness to pay; AUD, Australian dollar.
In 24 h TICI 2b/3 patients, EVT became a dominated (ie, more costly and less effective) treatment compared with the non-EVT treatment in M2 occlusion patients (Supplementary Table 5).
Model Validation
Model structure, inputs and results were checked by a neurologist specializing in stroke treatment (MP). Extreme value testing indicated that EVT might become cost-ineffective (with marginally higher QALY and significantly higher costs) in M2 occlusion (Supplementary Table 8). Our model predicted that the 5-year cumulative rate for recurrent stroke was 20% and the survival rate was 80%, respectively, similar to the real-world observations identified by our literature search.16,17
Discussion
Our modeled analysis suggested different cost-effectiveness conclusions for EVT in M2 segment occlusion stroke patients in Australia using trial (ie, additional benefits with cost-saving) or real-world (ie, more benefits with increased costs) data, although the long-term benefits from EVT appeared to be similar. For the long-term costs, nursing home care, initial hospitalization, and management costs were the key cost drivers in both EVT and non-EVT-treated patients.
The treatment benefits from EVT in M2 occlusion seemed less than that in ICA/MCA-M1 occlusions from our model-based analysis, however, there was still a benefit of EVT over medical treatment, including intravenous thrombolysis, a finding that is consistent with the literature. We also performed a quick literature search to identify relevant published cost-effectiveness analyses of EVT in ICA/MCA-M1 occlusion LVO stroke from the United States, Europe, and Australia.5,12,18–23 Even though the results from these cost-effectiveness analyses were not directly comparable due to the heterogeneity in their methods, jurisdictions, and model inputs, it appeared that QALY gains from EVT were likely to be greater in the ICA/MCA-M1 occlusion patients than in M2 occlusion patients using clinical trials evidence (Supplementary Table 6 and Table 2), which may be due to the reduced functional benefits (ie, mRS outcome) from EVT. The cost-effectiveness results from published literature were supportive of our findings in relation to ICA/MCA-M1 occlusion. From INSPIRE registry, around 68% of patients achieved mRS≤2 at 3-month without the EVT treatment regardless of the occlusion locations, while in trials with predominantly ICA/MCA-M1 occlusions (over 90%), around 26.5% of patients achieved the same outcome in the absence of EVT treatment. This may potentially explain the reduced benefits of EVT in M2 occlusions.
The results from our study are different from that based on clinical trial outcomes (ie, HERMES collaboration) which reported EVT was cost-effective in patients with M2 occlusion stroke in the United States. 4 This is mainly due to non-EVT patients in the HERMES achieving poorer outcomes compared with those in INSPIRE (mRS=0–2: 39.68% vs 62.22%), while EVT patients had similar outcomes from trials and real-world (mRS=0–2: 58.21% vs 56.10%). Our model showed that EVT patients achieve comparable QALY gains in the long-term from HERMES and INSPIRE (5.79 vs 5.70), suggesting no significant difference in EVT’s benefits in everyday practice. Furthermore, INSPIRE recruited older patients than those from HERMES (median age=72 vs 66 in the EVT treatment group, respectively), while there is evidence indicating better outcomes post EVT in younger patients.24,25 However, if the effectiveness of EVT from the HERMES collaboration was used in our economic model, the cost-effective conclusion would be the same as the US-based study (ie, cost-saving and more effective).
Due to the difficulties in determining the location (proximal or distal) of the M2 occlusion in the real-world environment, one of the INSPIRE registry’s limitations is that the location (proximal or distal) of the M2 occlusion was not documented. The HERMES collaboration predominantly had patients with the proximal location of M2 occlusion (116/130), while many proximal M2 occlusions are more easily accessible for EVT as seen with M1 segment occlusion. 26 Considering the timeframe of the INSPIRE data capturing (2015–2019), proximal M2 occlusions probably contributed to most of the cases included in this analysis.
Even though it may be cost-effective to offer EVT in M2 occlusion stroke, there are still technical considerations to factor into decision-making. Mechanical EVT is designed in a way to match the target arterial profile (M1 segment) and allow optimal access. Devices suitable in the proximal arterial segments are less likely to fit the distal arterial segment’s arterial profile and access requirements. Of 27 (the other 15 patients had the missing outcome in TICI) M2 occlusion and EVT-treated patients in INSPIRE, 25 patients achieved TICI 2b/3 at 24 hours. It is worth noting that compared with patients in whom reperfusion (TICI 2b/3) could be achieved with non-EVT treatment, achieving reperfusion with EVT is highly cost-ineffective due to significantly higher costs and reduced health benefits. This is largely because the use of thrombolysis in patients with an MCA-M2 occlusion is effective with a higher rate of reperfusion than in other occlusion locations, such as the MCA-M1 where thrombolysis is less effective. Smaller diameter next-generation stent retrievers and aspiration catheters could potentially further enhance reperfusion rates and lead to better clinical outcomes in patients with M2 occlusions. 27 Meanwhile, improvements in technique and devices are associated with varied recanalization rates. A meta-analysis of 12 studies, most of which had a retrospective study design, reported a non-significant association between device type and recanalization outcome. 3 Particularly, it was found that 87% recanalization was achieved with stent retriever thrombectomy (SRT) first and 80% with aspiration first, with functional independence in 57.6% with SRT first and 48.6% with aspiration first. Conversely, another study observed that recanalization was 80.5% for SRT compared with 86.8% in aspiration first technique, with good outcomes in 59.9% with SRT and 74.5% with a direct aspiration first pass technique. 28
The absence of clear clinical guidelines has led to significant variations in the application of EVT for the treatment of M2 occlusions. 29 The revised AHA guidelines 2019 stipulated that even though the benefits are uncertain, EVT with a stent retriever may be reasonable for carefully selected patients with acute ischemic stroke who had causative occlusion of MCA segment 2 (M2) or 3 (M3). In a recent international, multidisciplinary survey in 2019 of 607 physicians, 65.4% of respondents favored EVT in acute M2 occlusions under current local resources. 29
Suboptimal access to treatment facilities with EVT capabilities and monetary (EVT procedure could cost over USD20 000) and health–policy-related limitations are possible causes of low EVT decision rates in some regions, specifically in developing countries. Our model-based analysis showed inconsistent health economics results of EVT from the long-term using real-world vs trial-based effectiveness, highlighting the need for a dedicated RCT to address this critical question.
This is the first economic evaluation of EVT in M2 occlusion stroke using real-world and trial-based results in Australia. There are some limitations. First, patients’ characteristics in the EVT and non-EVT treatment groups from the INSPIRE were not perfectly (but closely) matched due to technical difficulty (propensity score matching is based on a range of baseline characteristics rather than a single variable). Second, we only took a limited societal perspective to measure the costs and benefits. Due to the median age of INSPIRE participants (over 70 years old while the current age for pension access is around 66 in Australia), we did not estimate the costs due to productivity loss. Third, the probability of recurrent stroke was sourced from all stroke types. However, sensitivity analyses suggested that this was not a key determinant of cost-effectiveness. After matching, there were still differences between the 2 groups, which may introduce bias in the cost-effectiveness results. However, the baseline NIHSS, a measure of stroke severity, was highly comparable in the matched cohorts. In addition, given that all the costs were derived from the Australian context, the results may not be generalizable to other countries without universally funded health care. While the trends identified in the data are likely still to apply, but the effect size would be altered. Moreover, one limitation of using registry data for cost-effectiveness analysis lies in the potential bias in deriving the effectiveness of EVT. Similar bias may arise from pooling subgroup patients of RCTs examining LVO strokes. It is uncertain in which direction the bias may have impacted the cost-effectiveness results. Even though the PSA was undertaken to test the uncertainty around the 3-month mRS outcomes, it should be acknowledged that unlike the continuous end point in the clinical trial where the standard deviation was captured, the distribution of mRS outcome cannot seize the potential uncertainty in the same way as SD (ie, the larger SD leads to wider confidence interval which are more likely to generate different outcomes in the simulation that ultimately leading to higher value of additional information to reduce the uncertainty). The additional value of collecting further evidence seemed low, however, this was due to the limitation of PSA around distributional outcome. Nonetheless, the probability of EVT being cost-effective in M2 occlusion was similar to that reported in an earlier study that was based on the HERMES collaboration data. Fourth, compared with inverse probability weighting, propensity score matching has to exclude some subjects because no match can be found. Therefore, the analysis is restricted to a sub-population that is not explicitly described. Due to the smaller sample size of EVT patients from INSPIRE, the effectiveness of EVT in the real-world may not be reliably demonstrated. However, this is the best available evidence given the absence of a dedicated RCT in M2 segment occlusion patients. Finally, the generalizability of the cost-effectiveness of EVT in real-world and clinical trial settings to other countries may be limited considering different willingness-to-pay per QALY thresholds in various countries (ie, the United Kingdom adopted £20 000 while the United States often employed USD50 000) and unit costs applied. While due to the similarities in health care systems among certain western countries, the cost-effectiveness of interventions tends to remain consistent.
Conclusions
Our study suggested that the benefits gained from EVT in M2 occlusion stroke in the real-world were similar to that observed in the clinical trials, even though the cost-effectiveness may be different using registry or trials’ outcomes. The clinical and cost benefits from EVT appeared to be reduced in M2 compared with that from the ICA/MCA-M1 occlusions. A dedicated RCT in M2 occlusion is required to establish the effectiveness and cost-effectiveness of EVT in this subgroup.
Supplemental Material
sj-docx-1-jet-10.1177_15266028231201098 – Supplemental material for Cost-Effectiveness of Endovascular Thrombectomy in M2 Occlusion Stroke: Real-World Experience Versus Clinical Trials
Supplemental material, sj-docx-1-jet-10.1177_15266028231201098 for Cost-Effectiveness of Endovascular Thrombectomy in M2 Occlusion Stroke: Real-World Experience Versus Clinical Trials by Lan Gao, Elise Tan, Chushuang Chen, Timothy Kleinig, Bernard Yan, Andrew Cheung, Chris Levi, Carlos Garcia-Esperon, Dennis Cordato, Chris Blair, Longting Lin, Mark Parsons and Andrew Bivard in Journal of Endovascular Therapy
Footnotes
Author Contributions
LG, MP, and AB had full access to the data in the study and take responsibility for the accuracy of data analysis. Study concept and design: LG, MP, AB. Acquisition, analysis, or interpretation of data: LG, ET, CSC, TK, BY, AC, CL, CGE, DC, CB, LTL, MP, AB. Drafting of the manuscript: LG, MP, AB. Critical revision of the manuscript for important intellectual content: CSC, TK, BY, AC, CL, CGE, DC, CB, LTL, MP, AB. Statistical analysis: LG.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
All data are available within the article. Any additional data will be made available upon reasonable request by a qualified researcher.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The ethics committee of NSW Human Research Ethics Committee approved the INSPIRE (HREC/11/HNE/287).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.