
Abstract
Objectives:
To analyze device designs, similarities and overlaps of custom-made fenestrated arch endografts intended for mid/distal arch thoracic endovascular aortic repair.
Materials and Methods:
A multicenter cross-sectional study analyzing custom-made anonymized graft plans was performed. Graft plans were included from a cohort of mid/distal aortic arch repairs using custom-made fenestrated aortic endografts treated at 8 centers. Grafts targeting >2 arteries were excluded. No patient/clinical data were analyzed. A descriptive analysis was performed followed by an analysis of overlap of the designs to reach a common design in which the greatest number of grafts would overlap.
Results:
One hundred thirty-one graft plans were included. All grafts were custom-made grafts from the COOK Medical Fenestrated arch platform. Ninety-four (71.8%) had a scallop-and-single-fenestration design, 33 (25.2%) had a single fenestration and 4 (4.3%) a single scallop. For analysis purposes, these latter 4 grafts were excluded. Two main graft plans (Plans 1 and 2) were proposed after analysis with similar configuration (1 scallop with 30 mm width, 20 mm height, 12:00 position; 1 preloaded fenestration with 8 mm diameter, 26 mm from the top of the graft and 12:00 position; tapered, with a 193 mm length and 32 mm distal diameter) but with 2 different proximal diameters of 38 mm (Plan 1) and 44 mm (Plan 2), reaching an overall feasibility of 85.8% (n=109), being 47.2% (n=60) and 38.6% (n=49) for each design, respectively.
Conclusion:
The degree of overlap between the studied fenestrated and/or scalloped thoracic endovascular aneurysm repair (TEVAR) graft designs was high. Future studies analyzing these designs in a real-world cohort of patients are needed to further address off-the-shelf feasibility.
Clinical Impact
In a multicenter study analyzing 127 fenestrated aortic arch endograft plans from 9 aortic centers, we found that the degree of overlap between the studied fenestrated and/or scalloped arch graft designs was high and that 2 proposed graft designs would be theoretically applicable in 85.8% of cases. Future studies analyzing these designs in a real-world cohort of patients are needed to further address off-the-shelf feasibility.
Keywords
Introduction
Thoracic aortic aneurysms have a calculated incidence and prevalence of 5.3 per 100 000 individuals/year and 0.16%, respectively. 1 They are usually asymptomatic but mortality is very high if they rupture, making timely treatment extremely important for these patients. 1 Thoracic endovascular aneurysm repair (TEVAR) is now the preferred method in most patients, but a healthy landing zone is required in the thoracic aorta, which should ideally be at least 2 cm in length. 2 Frequently, the healthy landing zone for descending thoracic aortic aneurysms is only found in Ishimaru Zone 1 or 2, leading to necessary inclusion or covering of the supra-aortic trunks.
Covering the left subclavian artery has shown to increase the risk for cerebral events and post-operative spinal cord ischemia, especially if long coverage of the aorta is expected.3,4 A hybrid approach with Zone 1 or 2 cervical debranching has been mostly used with acceptable results; 5 however, complications, such as stroke, phrenic nerve injury, brachial plexus injury, lymphatic leak, and bleeding complications may occur. 6 Alternatively, fenestrated endografts with scallops and fenestrations for the supra-aortic trunks have been used to overcome these limitations. A recent multicenter study by Tsilimparis et al,7,8 has shown that preloaded fenestrated endografts for landing Zones 1 and 2 are safe and feasible. However, these devices require customization to patient anatomy that may exclude patients with very large or urgent aneurysms due to time constrains patient anatomy that may exclude patients with very large or urgent aneurysms due to time constrains. Spanos et al, 9 have studied a series of custom-made designs of aortic arch branched devices intended for Zone 0 and found that due to similar arch anatomies, off-the-shelf grafts would be feasible for most patients, and therefore could be used for urgent cases. In this study, we aimed to analyze fenestrated endografts designs intended for Zone 1 or 2 from high-volume experienced centers to understand device design similarities and overlaps and possibly recommend off-the-shelf designs that would be feasible for urgent cases.
Materials and Methods
This study followed the reporting guidelines from the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for cross-sectional studies. 10
Study Design, Setting, and Participants
An international multicenter cross-sectional study based on retrospective analysis of custom-made anonymized graft plans was performed. All included grafts were custom-made grafts from the COOK Medical (Cook Medical, Bloomington, IN, USA) platform. Graft plans were included from a cohort of mid/distal aortic arch repairs using custom-made fenestrated aortic endografts treated at 8 high-volume aortic centers since the beginning of their experience up to January 2022. Only grafts targeting 2 or less supra-aortic vessels were included. No patient or clinical data were included in this study, therefore, ethical approval was waived. There were no company or other device-related limitations for inclusion in the study. We excluded graft plans in which more than 2 target vessels were included with either a dedicated fenestration or scallop or if no sizing details, including graft diameter and length, position of fenestration/scallop, and size and format of the fenestration/scallop were available.
Variables, Data Sources/Measurement, Bias, and Study Size
All graft plans were anonymized, and no patient or clinical data were shared. Only information available on the graft plan was included (Figure 1). This information included graft diameters, graft length, tapering, position of fenestrations and scallops, graft markers, distance from the top to the end of the scallop and to mid fenestration, scallop height and length, fenestration diameter, existence of fenestration struts, presence of preloaded catheter and wire, inner vessel diameter at the level of the scallop and fenestration, length of introducer tip, presence of orientation notch, existence of proximal barbs, spiral stabilizing wire, type of fabric (low profile or normal), curved nitinol cannula, pro-form design, outer diameter of the delivery system, and sheath length of the delivery system. An example of anonymized graft plans is depicted in Figure 1.
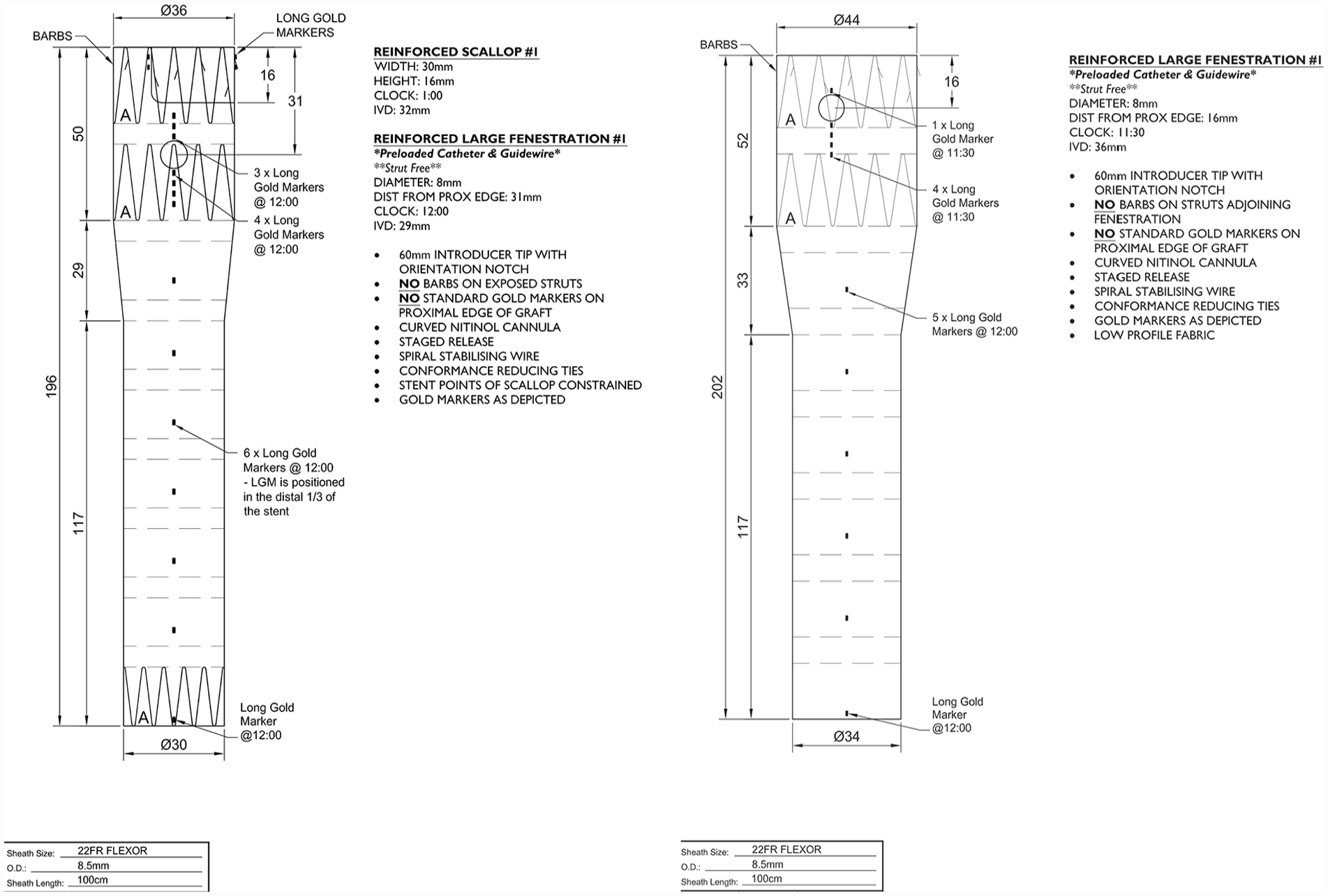
Illustration of an anonymized graft plan. On the left, a scallop and single fenestrated design, and on the right, a single fenestrated design.
The corresponding flat distance to each target vessel’s clock position was calculated using the inner vessel diameter and taking the 12 O’clock position as the reference point and as “0.” In this way, the flat distance was obtained by calculating the circumference according to the inner vessel diameter
In addition, if 2 target vessels were included the distance from the mid fenestration to the end of scallop was calculated according to the measurement present in the graft.
Graft effective seal and total seal were defined according to the Society for Vascular Surgery reporting standards. 11
Study Outcomes
First, a descriptive analysis of the graft plans, and each measurement, position, and feature was performed. This was followed by an analysis of the overlap of each design to reach a common design graft in which the greatest number of grafts would overlap. The objective was to propose a possible off-the-shelf design(s) that would accommodate most of the included patient plans.
Statistical Analysis
Statistical analysis was carried out using STATA version 16.1 (Statistics/Data analysis, StataCorp LLC, Texas, USA).
Continuous variables are presented as median (interquartile range [IQR]), with minimum and maximum values presented additionally. Categorical variables were expressed in numbers (percentage).
We defined as an overlapping graft if the proximal diameter varied 2 mm or less and if the position of the graft allowed for at least a 10 mm diameter perfusion of the target vessel intended for the scallop after graft rotation to accommodate for the position of the fenestration (i.e. the offset between the flat position of the scallop and the fenestration had to be <10 mm in a 30 mm width scallop).
Results
Included Graft Plans and Descriptive Data
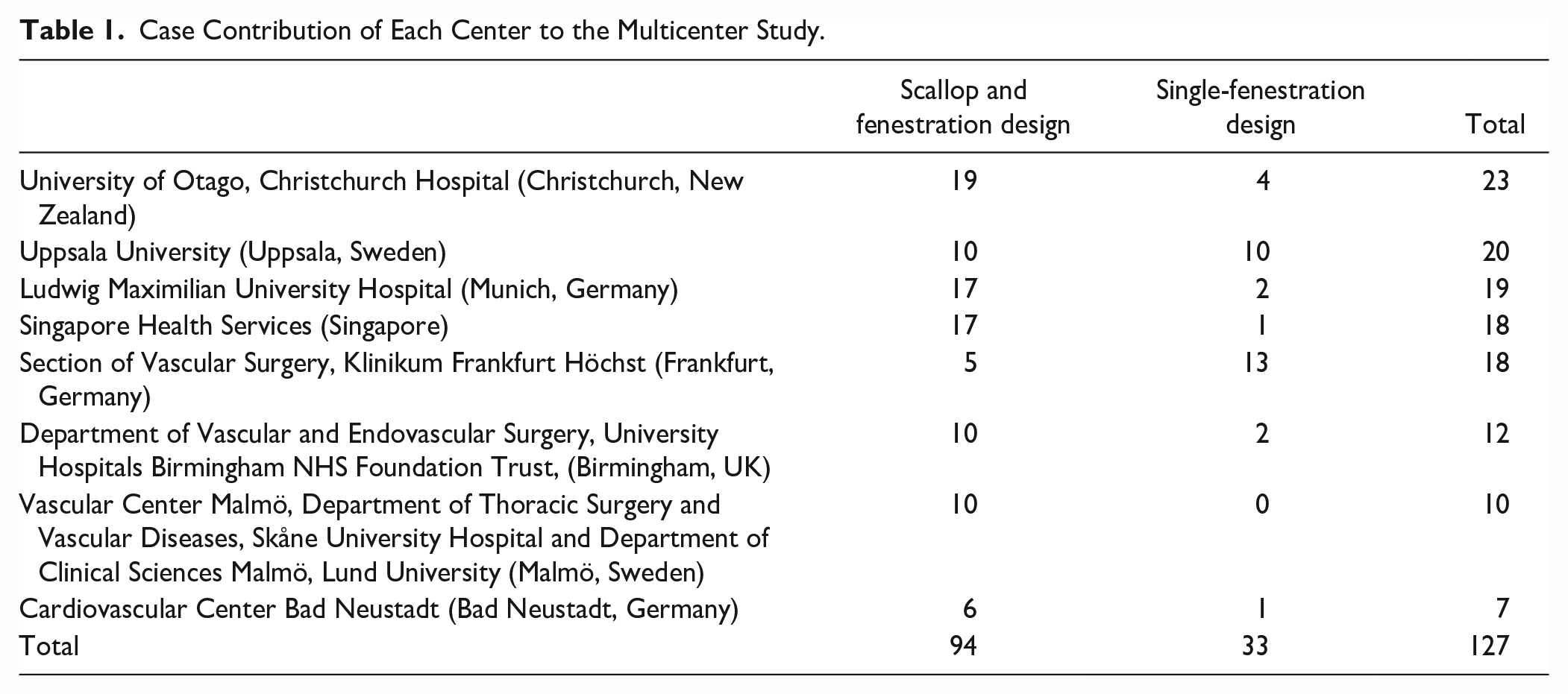
Overall, 131 graft plans were included. Most of the plans (n=94, 71.8%) had a scallop and single-fenestration design (ScFD), followed by single-fenestration design (FD) (n=33, 25.2%) and single scallop (n=4, 3%). There were no designs in which only 2 fenestrations without a scallop were used. Since only 4 graft plans had a single scallop, these grafts were not analyzed to the low representation, therefore, we analyzed 127 grafts. For analysis purposes, we first analyzed each design separately in 2 different cohorts. Each center’s contribution is depicted in Table 1.
Case Contribution of Each Center to the Multicenter Study.
Descriptive Analysis of Graft Designs
Detailed measurements and graft construction details are depicted in Table 2. All grafts had a preloaded catheter and wire for the fenestration. All fenestrations were strut-free and most were 8 mm in diameter (67% in the ScFD and 70% in FD), with the remainder being 10 mm. All scallops were reinforced and varied between 2 widths, either 20 mm, which was the more common (52%) or 30 mm (found in 48%). Tapering was found in most grafts (75.5% in ScFD and 54.5% in the FD). Low-profile fabric was found in 58 ScFD (61.7%) and 15 FD (45.5%). All grafts were designed with no proximal barbs on exposed struts, curved nitinol cannula, staged release mechanism, an orientation notch and spiral stabilizing wire. Scallop and fenestration position can be depicted in Figure 2A (for ScFD) and Figure 2B (FD), and are detailed in Table 2.
Descriptive Graft Plan Data.
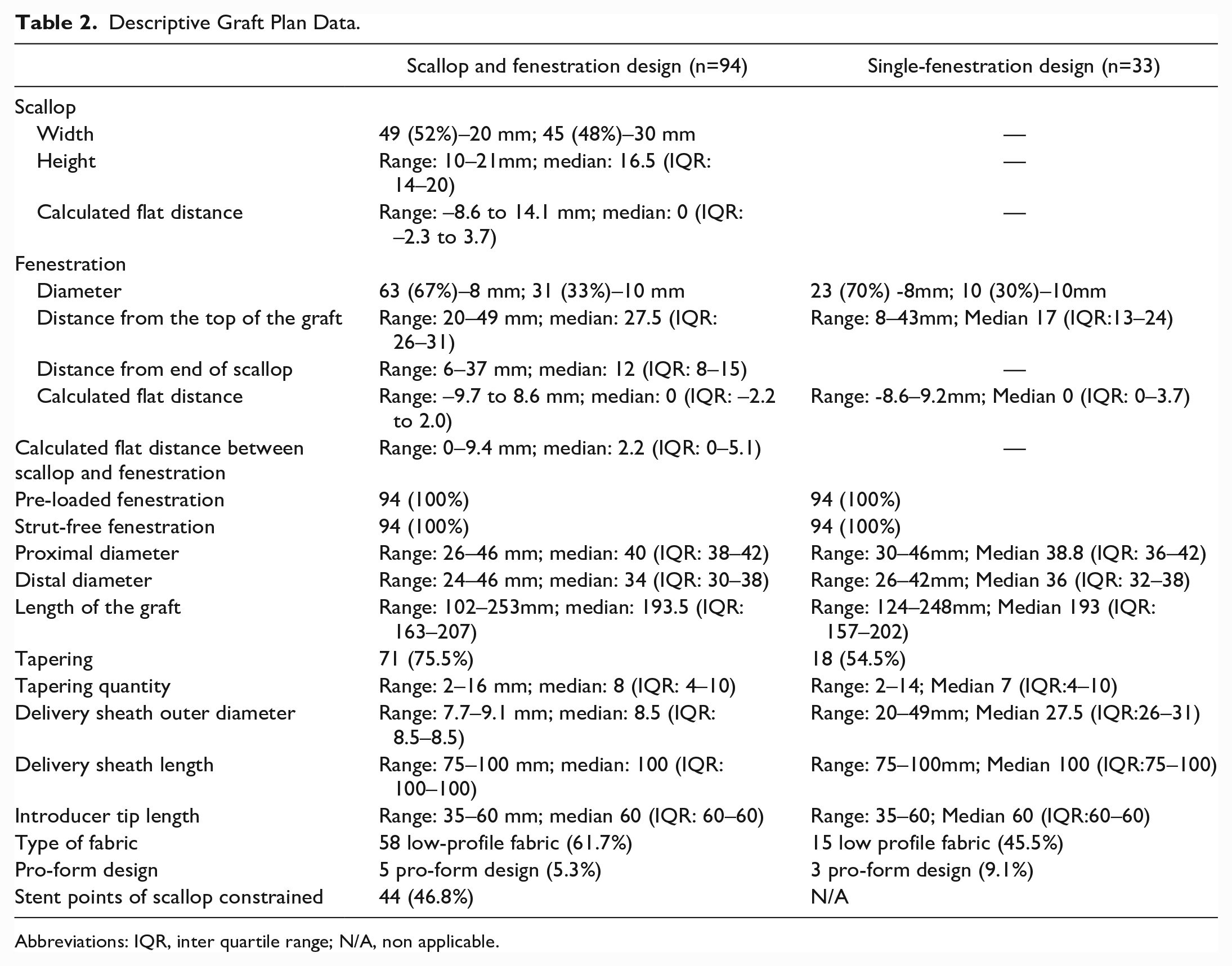
Abbreviations: IQR, inter quartile range; N/A, non applicable.
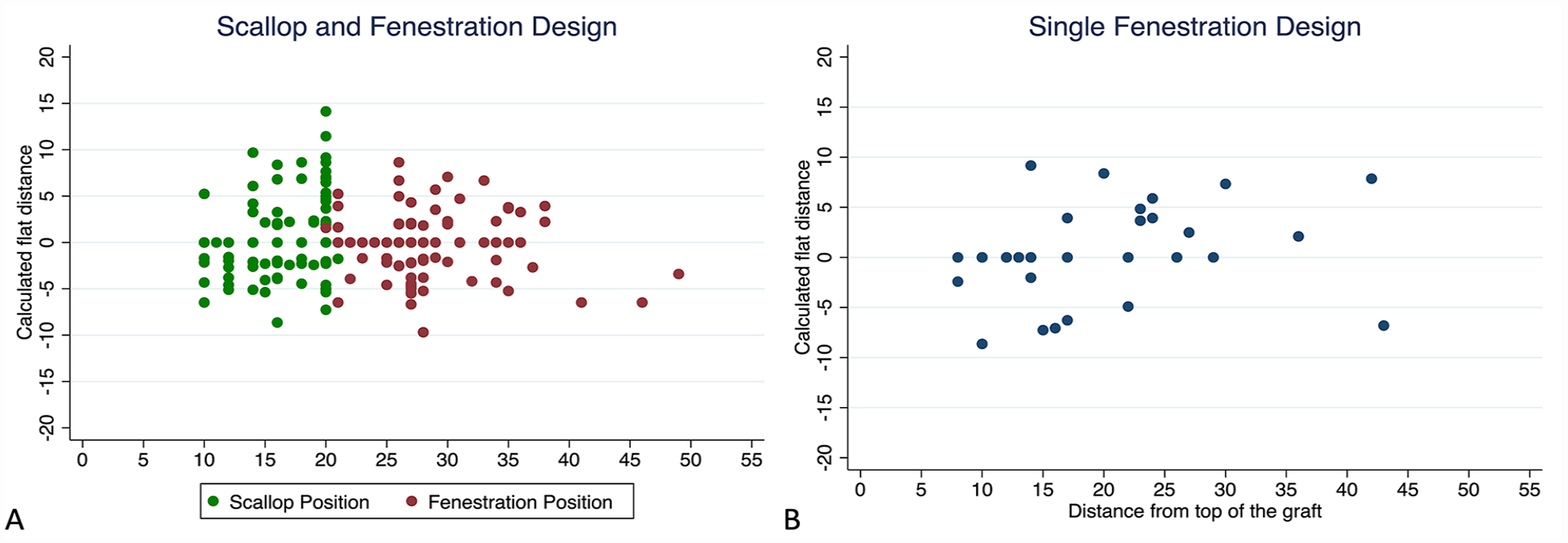
(A) Scatterplot illustrating the positions of the scallop and fenestration in the scallop and fenestrated arch designs. (B) Scatterplot illustrating the positions of the fenestrations in single fenestrated arch designs. Dots represent the distance from the top of graft to the distal end of the scallop (height of the scallop) and from the mid fenestration to the top of the graft.
Overlapping Graft Designs and Possible Off-the-Shelf Designs
Scallop and fenestration design
When analyzing clock positions and calculated flat distances for the scallop and fenestration in ScFD (Table 2), the maximum flat distance between both targeted arteries was 9.4 mm. This means that if a 12 O’clock position scallop and fenestration are used, with a preloaded catheter and wire for the fenestration, after graft alignment (to the fenestration position), the biggest offset between the center of the target artery and the middle of the scallop would be 9.4 mm. If a 30 mm width scallop is used, this means that for every case, a minimum of at least 10 mm diameter circumference would be left for the intended target vessel at the scallop area. Therefore, a 12 O’clock positioned fenestration and scallop would be feasible for every position we analyzed according to clock positions. Considering the distance between the end of scallop and mid fenestration, the minimum distance was 6 mm. This means that with a 20 mm deep scallop, 30 mm width scallop, 8 mm fenestration diameter, 12 O’clock position scallop, and fenestration and with a distance between the end of the scallop and the fenestration of 6 mm, every graft would be feasible, leaving only a question of graft diameter to accommodate off-the-shelf feasibility.
Regarding proximal diameters, the most common diameter was 40 mm (n=19, 20.2%). If one considers a 2 mm variability to be feasible, a 40 mm graft would accommodate for 50 of the graft plans (53.2%). In addition, if one adds 2 graft sizes, a 38 mm (feasibility n=43, 45.7%) and a 44 mm graft (feasibility n=38, 40.4%), that would accommodate a cumulative total of 81 of the 94 graft plans, with a cumulative overlap of 86.2%.
Taking this into account to accommodate for the biggest degree of overlap, one would consider 2 designs (Table 3):
Plan 1. Scallop positioned at 12:00, with 30 mm width, 20 mm height; fenestration position at 12:00, 8 mm diameter, and 6mm distance from the scallop to mid fenestration; with 38 mm proximally and 32 mm distally with a 193 mm length.
Plan 2. Scallop positioned at 12:00, with 30 mm width, 20 mm height; fenestration position at 12:00, 8 mm diameter, and 6 mm distance from the scallop to mid fenestration; with 44 mm proximally and 32 mm distally with a 193 mm length.
Off-the-Shelf Proposed Graft Plans and Overlapping Feasibility.
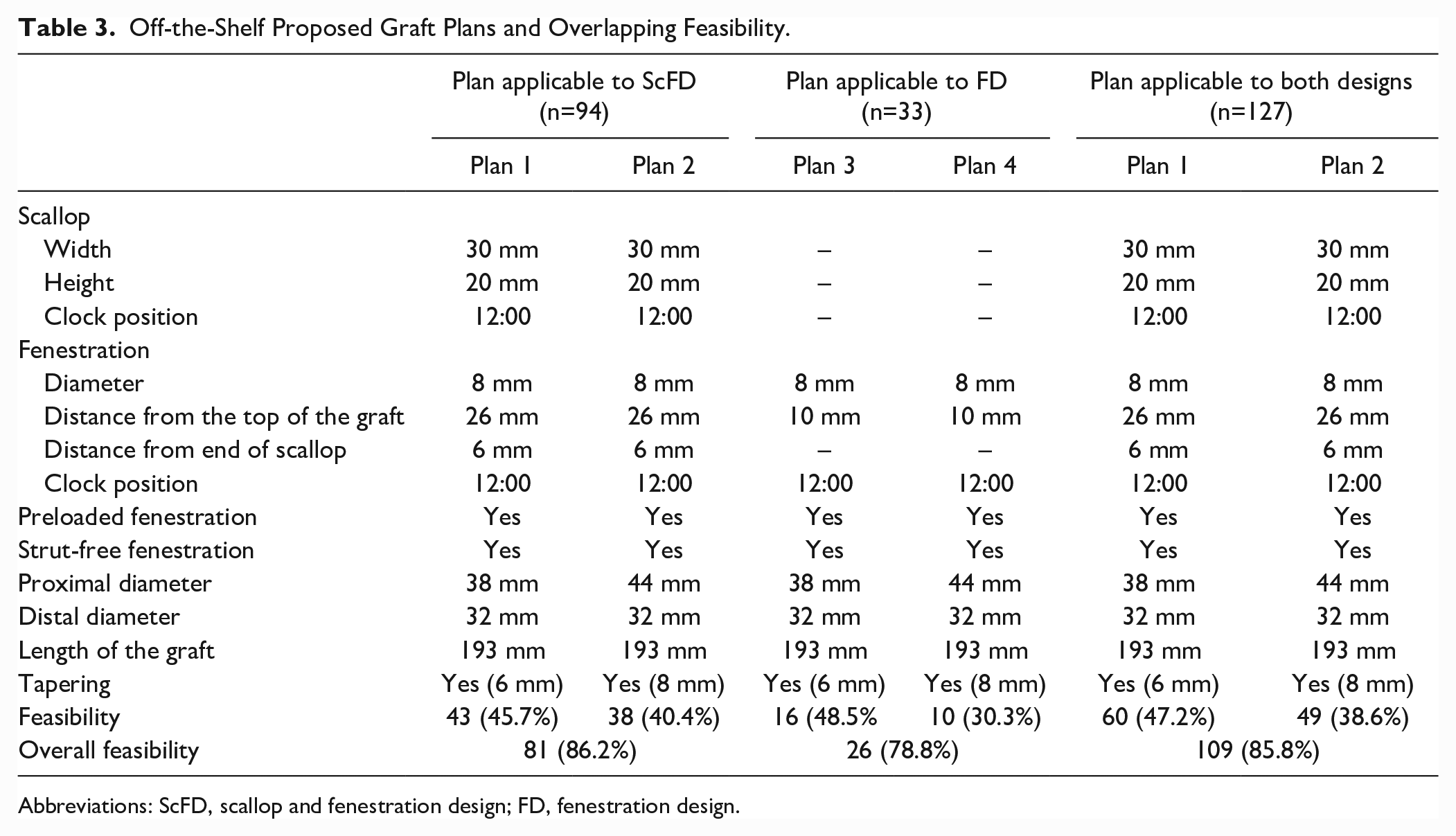
Abbreviations: ScFD, scallop and fenestration design; FD, fenestration design.
Single-fenestration design
When analyzing the single FD (Table 2), using the preloaded catheter and wire, the graft can be rotated to accommodate for various clock positions of the intended target artery. Since the median clock position was 12 O’clock, a 12 O’clock position 8 mm fenestration would be feasible according to the graft plans. The distance from the top of the graft varied between 8 and 43 mm. If a 10 mm distance from the top is used, 94% (n=31) of grafts would be feasible.
Regarding proximal diameters, the most common diameter was 38 mm (n=10, 30.3%). If one considers a 2 mm variability to be feasible, a 38 mm graft would accommodate for 17 of the graft plans (51.5%). In addition, if one adds a 44 mm graft that would accommodate an extra 11 graft plans (33.3%). Adding both sizes would have a cumulative overlap of 84.5% (n=28). Subtracting the 2 patients excluded using a 10 mm distance from the top, the overall feasibility would be 78.8% (n=26), being 48.5% (n=16) and 30.3% (n=10) for the 38 and 44 mm graft, respectively.
Taking this into account to accommodate for the biggest degree of overlap, one would consider 2 designs (Table 3):
Plan 3. Fenestration position at 12:00, 8 mm diameter, and 6 mm distance from the top of the graft to mid fenestration; with 38 mm proximally and 32 mm distally with a 193 mm length.
Plan 4. Fenestration position at 12:00, 8 mm diameter, and 6 mm distance from the top of the graft to mid fenestration; with 44 mm proximally and 32 mm distally with a 193 mm length.
Considering both designs (Table 3)
If one considers the same fenestration and scallop design adapted for both designs and considering the clock position would apply, the overall feasibility using Plans 1 and 2 would be 85.8% (n=109).
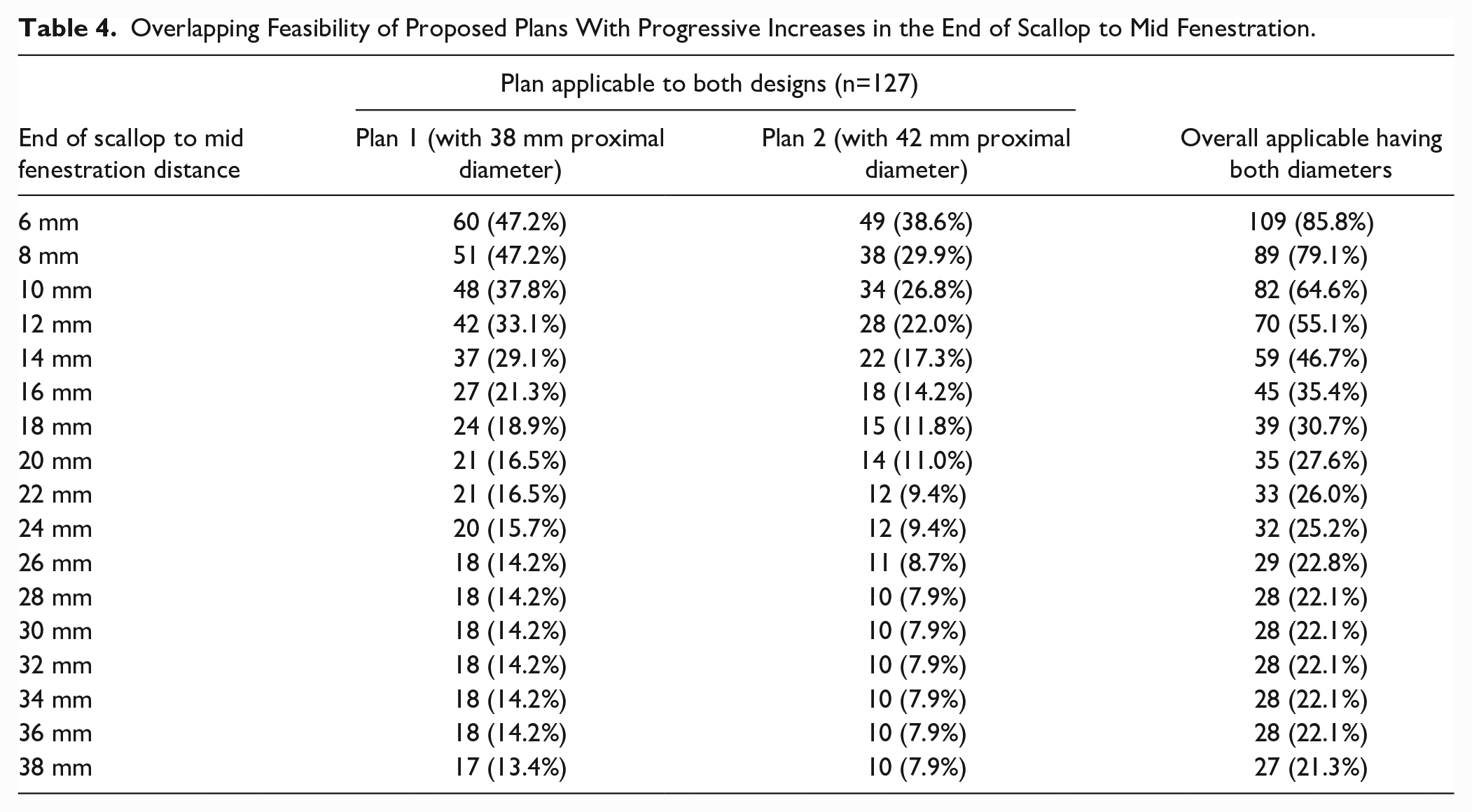
Keeping the same design and increasing the distance from the end of the scallop to mid fenestration decreases feasibility as depicted in Table 4. Overall having both Plans 1 and 2, increasing this distance to 12 mm will lower the feasibility to 55.1% (Table 4).
Overlapping Feasibility of Proposed Plans With Progressive Increases in the End of Scallop to Mid Fenestration.
Regarding distal diameter, the more common was 32 mm (n=21, 16.5%) considering both designs. We did not consider this as a limitation since it can be mated with distal thoracic grafts to accommodate for the necessary distal diameter.
In Tables 3 and 4, the off-the-shelf designs and their respective feasibility is depicted.
Discussion
The main findings from this study were the degree of overlap between the study designs which may have possible implications for feasibility with off-the-shelf designs. By having these grafts available, they might be useful to treat urgent patients unable to wait for a custom-made design. With Plans 1 and 2 as described above, overall feasibility would be 85.8%, looking at the overlap between the graft plans. The main limitation with these plans, however, would be the short length of effective seal with only 6 mm distance between the end of the scallop and mid fenestration, meaning an extra 10 mm of effective seal and 40 mm of total seal if one would compare with a straight standard endograft. Increasing the distance between the end of the scallop and mid fenestration by 6 mm would decrease feasibility overlap to 55% (Table 4).
One may argue that for urgent cases, covering of the left subclavian artery or cervical debranching would be an easier approach. Covering the left subclavian artery may, however, increase the risk of spinal cord ischemia and cerebral events3,4 and also increase the risk of Type 2 endoleaks with frequent need for adjunctive or secondary interventions, such as occluding the origin of the left subclavian artery with coils or plugs. 12 In situ fenestrations, parallel grafts or physician modified grafts are possible solutions in urgent cases, however, the durability of these options is not estabilished.13,14 Alternatively, single-branch devices might also be used, however, if graft-to-wall apposition is expected, technical difficulties maybe encountered with outer branch devices.15,16 A custom-made single inner branch is also available in certain companies; however, no data have been published using these devices for mid-to-distal arch repair.
Cervical debranching and TEVAR is a valid treatment option with proven results, however, complications, such as peripheral nerve injury, post-operative bleeding complications and phrenic nerve palsy are not uncommon. 6 Konstantinou et al 5 have shown that in a high-volume experienced center, bleeding complications still occurred in 11.4%, peripheral nerve damage in 9,5%, chylous fistula in 3.8%, local wound infection in 2.4%, and stroke in 4.3%. Furthermore, if performed in the same stage as the endovascular aortic repair, as is the case for most urgent procedures, local complications are even higher. 6
Fenestrated TEVAR may have some benefit by avoiding the need for cervical debranching, supra-aortic vessel occlusion and need for secondary or adjunctive interventions. Konstantinou et al 12 have shown that for Zone 2 pathologies, fenestrated TEVAR compared with TEVAR and cervical debranching had high technical success with similar patency rates for target vessels without the complications related to cervical debranching.
Fenestrated TEVAR is, however, a complex procedure and should be performed in experienced centers. The use of a preloaded catheter and wire may improve correct device alignment and fenestration and target vessel catheterization and stenting. 7 However, wire entanglement may occur between the preloaded wire and the main stiff wire or may also catch the edge of the proximal stent that can be avoided with careful advancement and pulling on the preloaded wire in a through and through configuration.7,8 In addition, very tortuous anatomies might make it difficult to align the graft in the arch, especially if some rotation is necessary to correctly align the device fenestration. 7 This may be an added challenge when using an off-the-shelf device with a fixed 12 O’clock position. In our cohort, the most “extreme” angulations for the fenestration varied 1 hour from the 12 O’clock position. In these cases, if tortuous anatomies exist in the aorta, it might be difficult to rotate the graft into the intended position, which is a limitation of not using a custom-made device. Therefore, case selection is also paramount to achieve technical and procedural success. 7 In addition, adequate cardiac output reduction may be important to precisely position the graft in the arch.17,18
Custom-made devices have the advantage of being the optimal device for the patient’s anatomy and should be preferred in elective settings.7,8,19 –21 However, device planning, design and manufacturing times make it not possible to use in urgent settings. In these cases, having an off-the-shelf graft with an appropriate design would be very useful, and our data show that this would be feasible for a significant number of patients.
Our study has some limitations. The cross-sectional study of device design makes it only possible to analyze design overlap and theoretical feasibility based on device design similarities. We did not analyze any patient data; therefore, it is not possible to accurately state that the same degree of feasibility would exist when analyzing each patient and their clinical case presentation. Furthermore, although these grafts were intended for mid/distal arch repairs we do not have information on which target arteries were included, which may have implications of the design applicability. No longitudinal data or external applicability of our proposed designs were analyzed; therefore, we cannot predict if these off-the-shelf plans would have the same technical and procedure success or durability as custom-made devices.
This study, however, describes relevant descriptive data on device design and device overlap which may lead to the development of off-the-shelf designs for patients with mid to distal arch pathologies. Future studies are required to determine the external applicability and feasibility of these proposed off-the-shelf designs in a cohort of patients with Zone 1 or 2 pathologies.
Conclusions
The degree of overlap between the studied fenestrated and/or scalloped TEVAR graft designs was high. With 2 main proposed off-the-shelf graft plans according to device design, feasibility was 85.8%. Future studies analyzing these designs in a real-world cohort of patients are needed to further address off-the-shelf feasibility.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: ΝΤ and DA are proctors for and have received institutional Research funding from Cook Medical.