
Abstract
Purpose:
The purpose of this study was to evaluate the safety and efficacy of antegrade fenestration re-entry (AFR) using a dual guidewire angioplasty balloon for chronic total occlusion (CTO) in patients with peripheral artery disease (PAD).
Material and methods:
This is a retrospective score matching analysis study comparing a study cohort composed of PAD patients with CTO treated with AFR subintimal recanalization using a dual guidewire angioplasty balloon and a matched control group, selected on baseline cardiovascular risk factor and lesions characteristics, treated with a conventional subintimal recanalization. Procedure outcomes include procedural success, successful subintimal re-entry, need for distal puncture, procedural time, fluoroscopy time, and dose area product. Clinical variables, including primary patency, freedom from amputation, freedom from re-interventions, and freedom from death, were used to compare the study groups.
Results:
Thirty patients in the study group were compared with 60 patients in the matched control group (mean age, male). A significant higher subintimal re-entry success (100% vs 76.7% in control group, p=0.004) and lower need of distal tibial punction (0 vs 14 [23.3%] patients in control group, p=0.004) were observed in the study group. A surgical conversion to bypass was needed in 5 patients in the control group. Shorter procedural and fluoroscopy time were observed in the study group (41.1±10.8 minutes vs 146.6±62. and 16.7±3.5 minutes vs 34.3±14.2 minutes in control group respectively, p<0.001 and p<0.001). Lower DAP were observed in the study group (914.1±309.9 µGym² vs 2026.5±845.7 µGym² in control group p<0.001). No significant difference were observed in terms of primary patency, mortality, amputation, and freedom from re-intervention.
Conclusion:
AFR using the Presto dual guidewire balloon is a step forward for crossing CTO which allows a simplified and quick treatment of BTK and ATK lesions compared with conventional approaches without increase of procedural risk and maintaining good clinical outcomes.
Keywords
Introduction
Endovascular “first approach” treatment of chronic total occlusion (CTO) lesions in patients with claudication and chronic critical limb ischemia (CLI) has been increasingly adopted through the development of new dedicated devices and techniques. 1 However, in about 20% of cases, an intraluminal revascularization is impossible, particularly in long chronic total occlusions (CTO), representing 39% to 49% of lesions in patients with CLI. In these cases, Bolia introduced a subintimal approach 2 that creates an intentional dissection to cross a CTO and creates a channel between the media and intimal space to a patent artery. Several groups adopted this approach in CLI patients with a re-entry failure in about 15% to 25% of cases.2–7 Recently, Carlino et al 8 demonstrated the efficacy of antegrade fenestration with an angioplasty of the subintimal space to improve re-entry during recanalization of coronary CTO.
In our study, we evaluated the safety and efficacy of subintimal recanalization in patients treated with antegrade fenestration re-entry (AFR) using a dedicated dual guidewire angioplasty balloon and conventional guidewires to treat long CTO in patients with CLI above (ATK) and below the knee (BTK).
Materials and Methods
Study Design and Population
The “percutaneous recanalization with antegrade fenestration re-entry using dual guidewire balloon—PRAESTO Study is a retrospective score matching analysis designated to evaluate efficacy and safety of an AFR approach using a dedicated Presto dual guidewire balloon catheter (MYRIAD Medical, Hayward, CA, USA) to perform a subintimal recanalization of long ATK and BTK CTO in patients with peripheral arterial disease (PAD), study group. Outcomes were compared with a control group, selected with a propensity score matching (PSM) analysis in a large cohort of patients with PAD, treated during the same period with conventional subintimal approaches. PSM was performed to select patients in study and control group and minimize selection bias and ensure covariate balance. PSM was performed with a 1:2 matching protocol without replacement (nearest neighbor matching algorithm) and a caliper width equal to 0.02 of the standard deviation of the logit of the propensity score. PSM generated using logistic regression was performed on age, sex, cardiovascular risk factors, Rutherford class, type, length, and diameter of lesions.
All patients included in the study were (1) >18 years of age, (2) Rutherford category 2 to 6 ischemia, (3) at least 1 ATK and/or BTK CTO lesions longer than 10 cm (4) Unsuccessful conventional antegrade subintimal recanalization attempt of at least 10 minutes. Major exclusion criteria included a planned major amputation before intervention, iliac artery lesions, pregnancy, contraindications (increased risk of bleeding, recent stroke, major surgery within 72 hours, hypersensitivity), or known resistance to antiplatelet therapy.
All patients provided written informed consent. The study conformed to the Declaration of Helsinki on human research.
Study Device
The Presto 3F dual guidewire balloon angioplasty catheter (as shown in Figure 1A and B) has 3 lumens and is compatible with 5F introducer sheaths when used with 2 guidewires. The dual guidewire balloon catheter is characterized by:
A first lumen located on the distal 15cm of the catheter compatible with a .014ʺ guidewire has a rapid exchange (RX) configuration that is used to advance a guidewire in subintimal channel—distal subintimal guidewire.
A second lumen compatible with a .014ʺ guidewire has a conventional over-the-wire configuration extending from the proximal end of the balloon catheter distally with the exit proximal to the distal balloon. This guidewire is used to perform the re-entry from subintimal space into the true lumen after angioplasty and fenestration of subintimal channel—proximal re-entry guidewire.
A third lumen serves for inflation and deflation of the balloon.
The distal semi-compliant balloon of the catheter is 20 mm long, has diameters ranging from 2 to 5mm, and is used to create subintimal fenestration
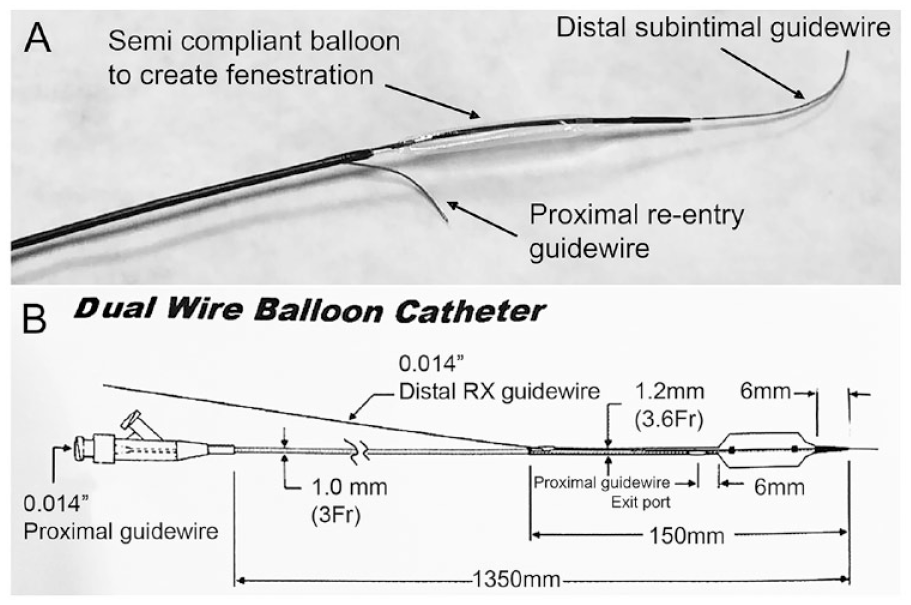
(A) The distal view of the Presto dual guidewire balloon catheter having the distal subintimal guidewire, semi-compliant balloon to create fenestration and proximal re-entry guidewire. (B) Overall view of the Presto dual guidewire balloon catheter. RX, rapid exchange.
Procedure
All procedures were performed in a dedicated angiographic suite under local anesthesia (lidocaine 2%) and mild sedation. An administration of a dual antiplatelet therapy with low-dose aspirin (100 mg/d) and clopidogrel (75 mg/d) was performed before the procedure. All procedures were performed through an antegrade ipsilateral common femoral artery approach using a 6-cm, 6-F Radifocus Introducer II sheath (Terumo, Tokyo, Japan). An activated clotting time ≥250 seconds was maintained during the procedure with an initial intra-arterial heparin bolus (3000–5000 units), followed by periodical infusion. Diameter and length of the target lesion was evaluated with a procedural biplanar angiography and a quantitative analysis using an automated contour detection program (Philips Healthcare, Best, The Netherlands).
In the study group, first attempts of intraluminal and subintimal recanalization of ATK and BTK CTO were performed with a conventional technique to luminally cross CTO as shown in Figure 2A. After 10 minutes of fluoroscopy time, a conventional luminal/subintimal approach to cross CTO was considered unsuccessful. Next, an AFR approach began, using the dual guidewire balloon by placing a distal subintimal guidewire in subintimal space distally to the CTO cap as shown in Figure 2B. The dual guidewire balloon catheter was then advanced over the distal subintimal guidewire to the middle of CTO distal cap in subintimal space. Next, the dual guidewire balloon catheter was inflated as shown in Figure 2C and deflated to create a transient fenestration between subintimal space and the true lumen. A proximal re-entry guidewire already introduced into the dual guidewire balloon catheter was then quickly traversed through the fenestration to re-enter into the distal true lumen as shown in Figure 2D. The dual guidewire balloon catheter and the distal subintimal guidewire were removed, and intervention continued using the proximal re-entry guidewire positioned in the true lumen as shown in Figure 2E. The procedure was completed with an angioplasty of the target lesion using an 0.014ʺ Amphirion balloon catheter (Medtronic, USA) or 0.035ʺ Absolute balloon catheter (Abbott, USA) with a lesion to balloon length ratio of 1:1. A subsequent angiographic control was performed to confirm successful recanalization without significant residual stenosis and flow-limiting dissection. In presence of suboptimal result, a second prolonged low-pressure dilatation was performed. A final stenting was performed if necessary, according to angiographic outcomes for persistent significant residual stenosis or flow-limiting dissection. In the control group, ATK and BTK CTO recanalization were performed using a conventional subintimal approach as previously described. 2 If necessary, in case of unsuccessful antegrade approach, a retrograde approach was attempted to complete the procedure.
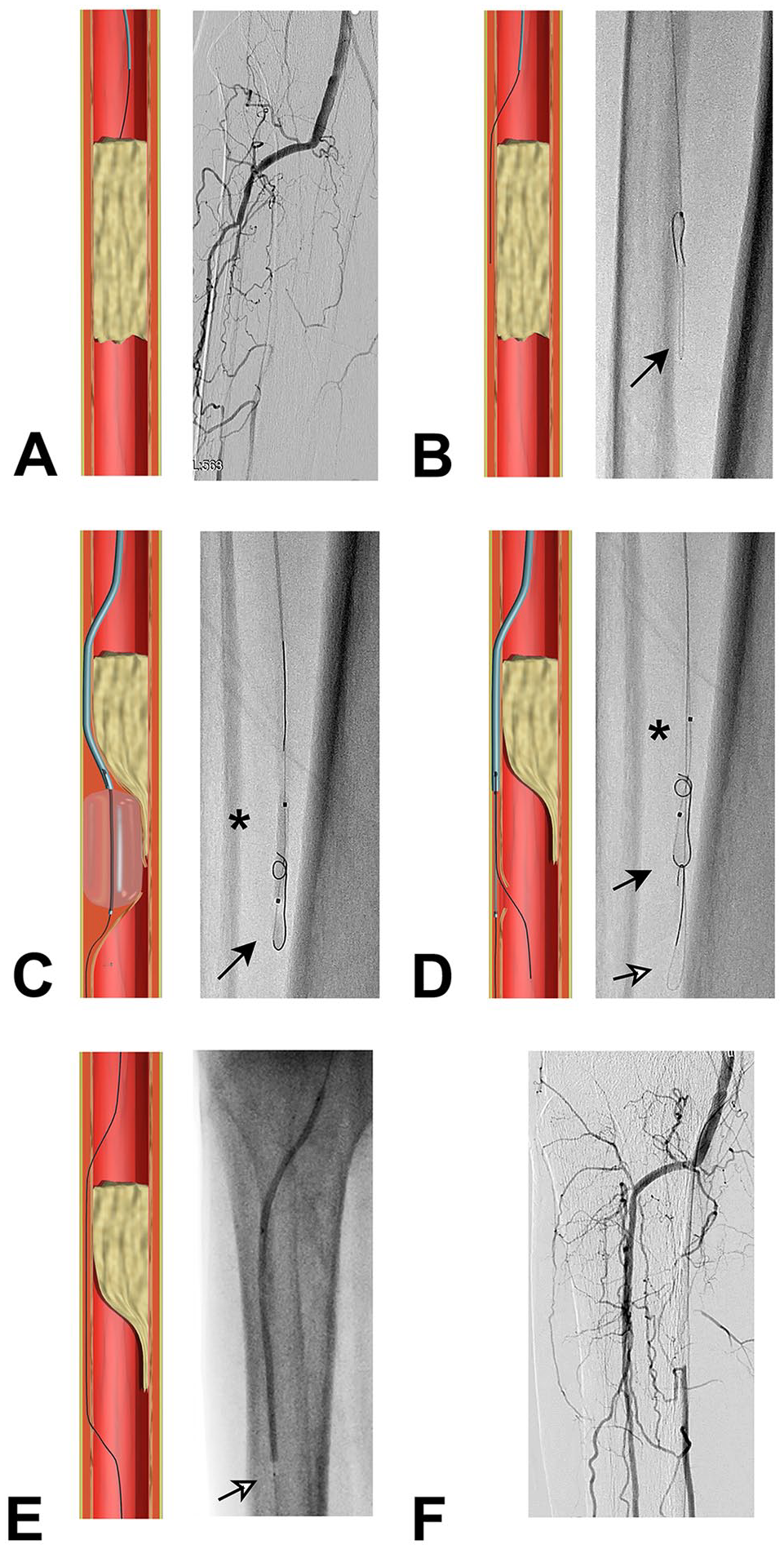
Antegrade fenestration re-entry for anterior tibial artery occlusion in patient with critical limb ischemia (CLI). After failure of a conventional subintimal approach (A), the Presto balloon was advanced on .014 guidewire (black arrow) to create a subintimal channel (B). Once joined the re-entry area, the Presto balloon was inflated (C) and deflated to create a fenestration in the subintimal space, and the second guidewire (white arrow) was advanced through the fenestration (D). The Presto balloon and first guidewire are then removed, and the procedure is completed with an angioplasty on the second guidewire (with arrow) with a conventional balloon (E, F).
Follow-up and Wound Care
Duplex ultrasound was performed at 1, 6, 12, and 24 month. Duplex ultrasound was performed at each visit; if the peak systolic velocity ratio was >2.5, the patient was classified as having restenosis >50%. Clopidogrel was maintained for a minimum of 3 months and then discontinued. Aspirin was maintained lifelong. In patients with CLI, a medical wound care was performed by an independent group of specialists not involved in the study. Proper shoes were prescribed according to ulcer location. Surgical debridement was performed at each visit according to progression of the ulcer to facilitate healing. In presence of positive bacterial culture, an adequate broad-spectrum antibiotic therapy was administered during follow-up.
Endpoints
The primary efficacy endpoint was a successful subintimal recanalization of the target vessel with successful re-entry into the true lumen documented by a distal angiography. The primary safety endpoint was the subintimal recanalization without vessel perforation, dissection, and periprocedural major adverse events (MAE). Successful procedure was also evaluated and defined as successful recanalization angioplasty and/or stenting in absence of residual stenosis >30% at final angiographic control. Procedural and fluoroscopy time, and Dose Area Product (DAP) were also evaluated, plus primary patency at 12 and 24 months Doppler FU was evaluated. Restenosis was defined as presence of the peak systolic velocity ratio >2.5 at target lesion. Major adverse events (MAE) included death, stroke, bleeding, needing transfusions myocardial infarction, need for surgical revascularization, distal embolization, and recurrence of CLI. Clinically-driven target lesion revascularization and limb salvage were also evaluated at 12 and 24 months.
Statistical Analysis
Statistical analysis was performed using SPSS software (Version 25.0, SPSS Inc, Chicago, IL). No statistical powering requirements were specified for this retrospective safety and efficacy evaluation. Continuous variables are described as mean ± standard deviation. Categorical variables are given as the numbers. Comparison between groups of continuous variables were performed with unpaired Student t test. Categorical variables were compared with chi-square test. Primary patency, freedom from amputation, re-intervention, and death were evaluated according to Kaplan-Meier methods and compared with log-rank test. A value of p<0.05 was considered as statistically significant.
Results
Between May 2018 and December 2019, 294 patients were treated with a subintimal approach for long ATK and/or BTK CTO for CLI: 44 patients using the AFR with dual guidewire balloon and 250 with a conventional subintimal approach. Ninety patients were selected with a propensity score–matched analysis: 30 patients in the study group and 60 in the control group. Baseline demographics and lesions characteristics are reported in Table 1. Overall, 33 ATK CTO and 68 BTK CTO were treated with a subintimal approach in both groups. In the study group, 34 CTO lesions (11 ATK and 23 BTK) were treated using the dual guidewire balloon, and in the control group, 67 CTO lesions (22 ATK and 45 BTK) were treated using conventional techniques. Lesion characteristics are reported in Table 2. No difference in lesions length, diameter, and PACSS calcification score 9 were observed between the two groups.
Demographic Variables.
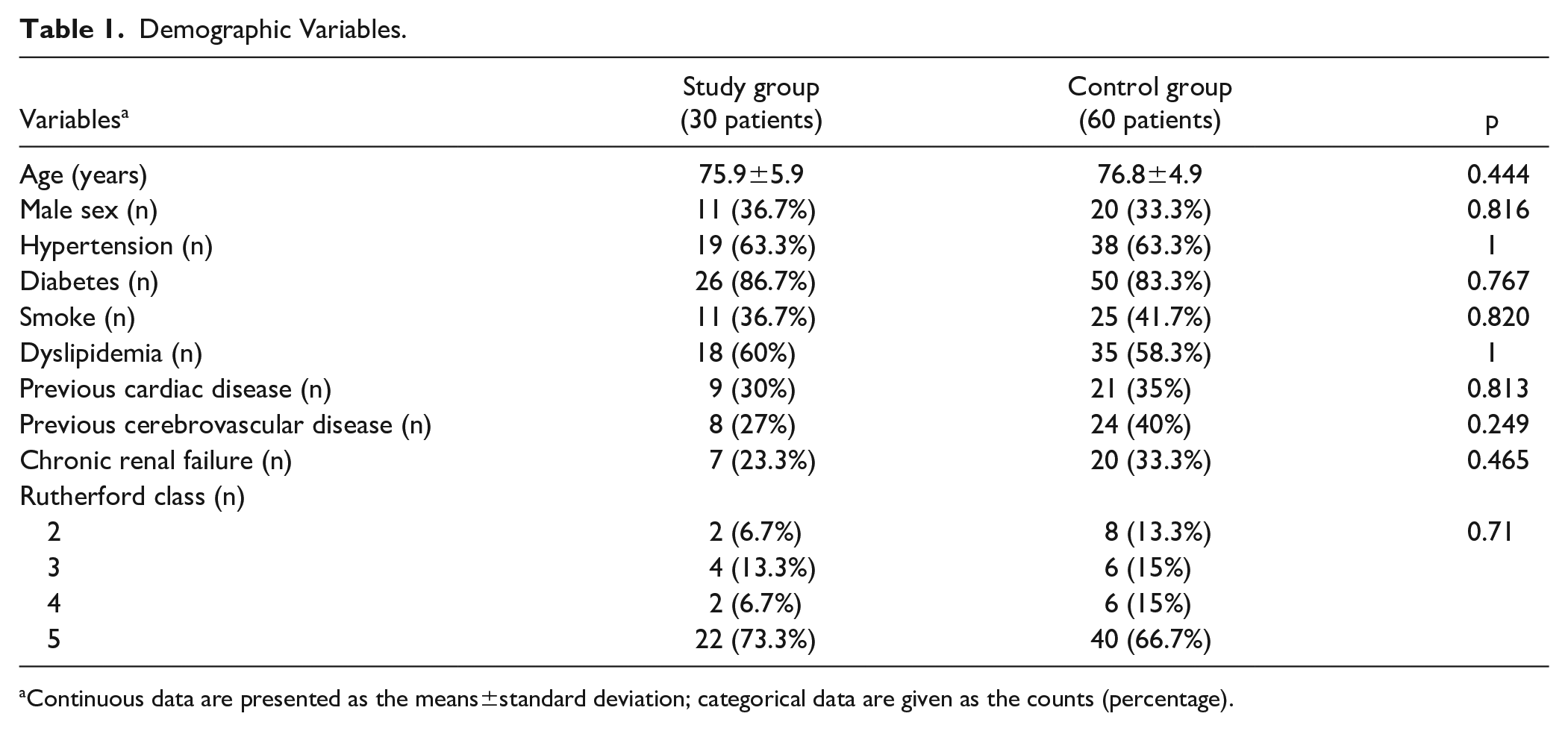
Continuous data are presented as the means±standard deviation; categorical data are given as the counts (percentage).
Intraoperative and Lesions Variables.
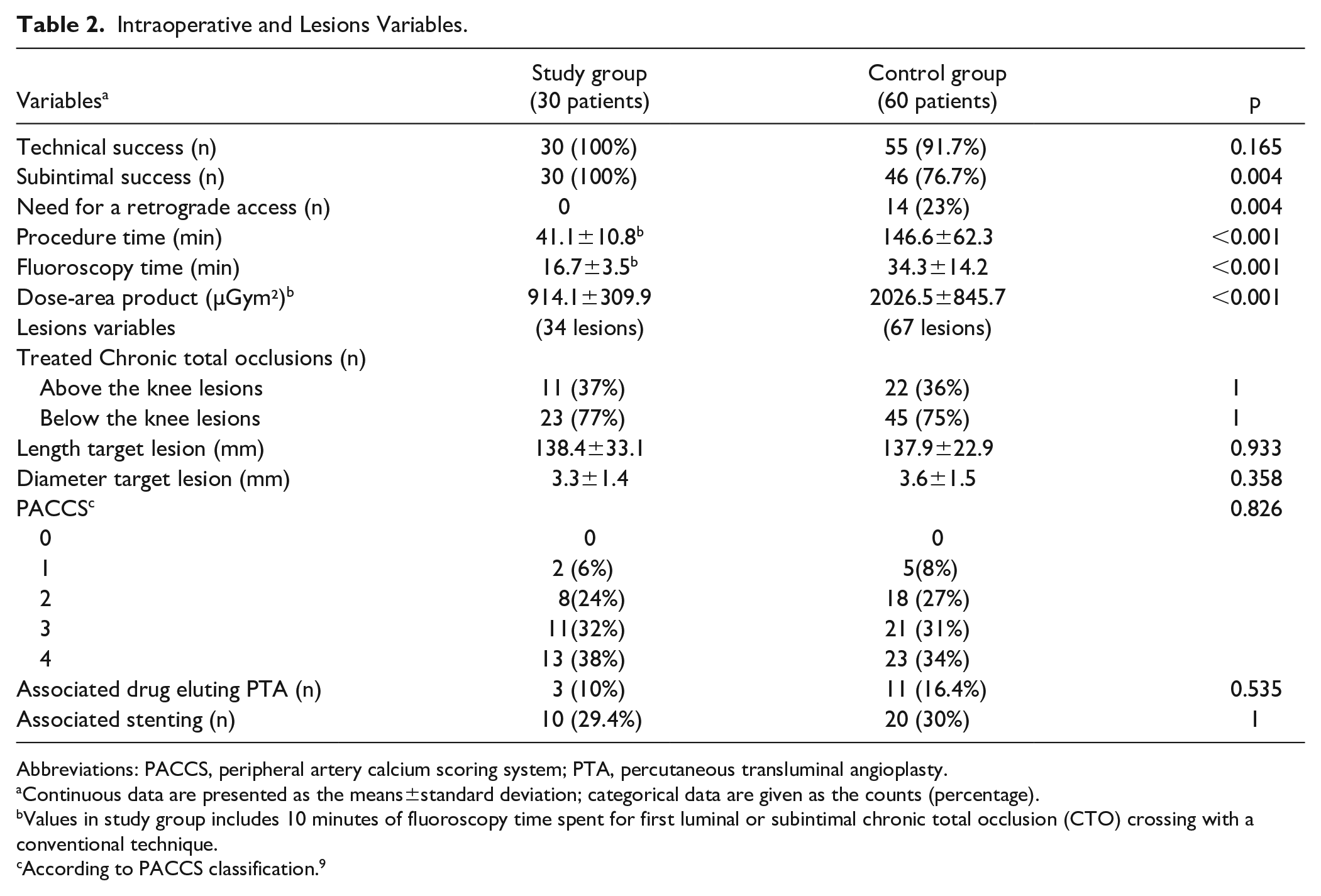
Abbreviations: PACCS, peripheral artery calcium scoring system; PTA, percutaneous transluminal angioplasty.
Continuous data are presented as the means±standard deviation; categorical data are given as the counts (percentage).
Values in study group includes 10 minutes of fluoroscopy time spent for first luminal or subintimal chronic total occlusion (CTO) crossing with a conventional technique.
According to PACCS classification. 9
A successful procedure was obtained in all 30 patients in the study group (100%) and in 55 patients (91.7%) in control group (p=0.165). A successful antegrade subintimal recanalization was obtained in all patients in the study group (100%) and in 46 patients (76.7%) in control group (p=0.004). In 14 patients (23.3%) from the control group, recanalization was completed through distal puncture of BTK vessel and a retrograde recanalization. In 5 patients (8.3%), the procedure was converted to a distal surgical bypass for distal extension of the dissection or vessel rupture. No other major complications were observed in both groups. Procedural time was 41.1±10.8 minutes in the study group and 146.6±62.3 minutes in the control group (p<0.001). Fluoroscopy time and dose area product were respectively 16.7±3.5 minutes and 914.1±309.9 µGym² in the study group and 34.3±14.2 minutes and 2026.5±845.7 µGym² in the control group (respectively p<0.001 and p<0.001).
At 12 months, 2 major amputations were observed in the study group and 7 amputations were observed in the control group (p=0.712). One additional major amputation was observed in the study group and 2 in the control group at 24-month follow-up (p=0.744) (Figure 3). All amputations occurred in patients with a previous critical limb ischemia. Primary patency was 88% (91% in ATK lesions and 48% in BTK lesions) in the study group and 71% in the control group (82% in ATK lesions and 47% in BTK lesions) as observed at 12 months US Doppler control. Primary patency at 24-month follow-up was 48% (73% in ATK lesions and 34% in BTK lesions) in the study group and 50% (73% in ATK lesions and 36% in BTK lesions) in the control group (p=0.897) (Figure 4). Freedom from target lesion revascularization was 76% in the study group and 71% in the control group at 12-month follow-up and 73% in the study group and 69% in the control group at 24-month follow-up (p=0.914) (Figure 5). Freedom from death was 93% and 87% in the study group and 92% and 83% in the control group, respectively at 12- and 24-month (p=0.666) follow-ups (Figure 6). Midterm results are reported in Table 3.
Immediate and Mid-Term Outcomes.
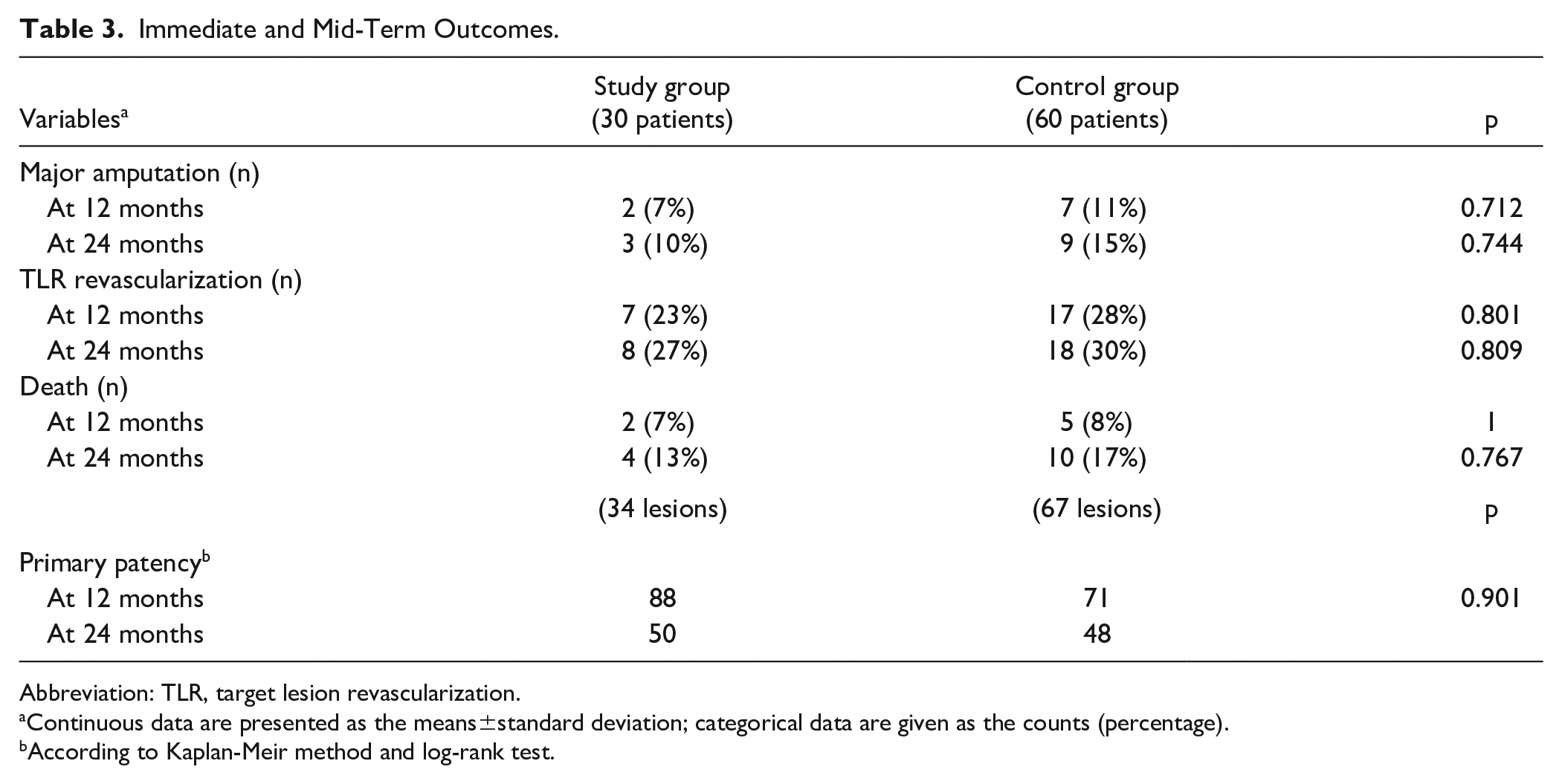
Abbreviation: TLR, target lesion revascularization.
Continuous data are presented as the means±standard deviation; categorical data are given as the counts (percentage).
According to Kaplan-Meir method and log-rank test.
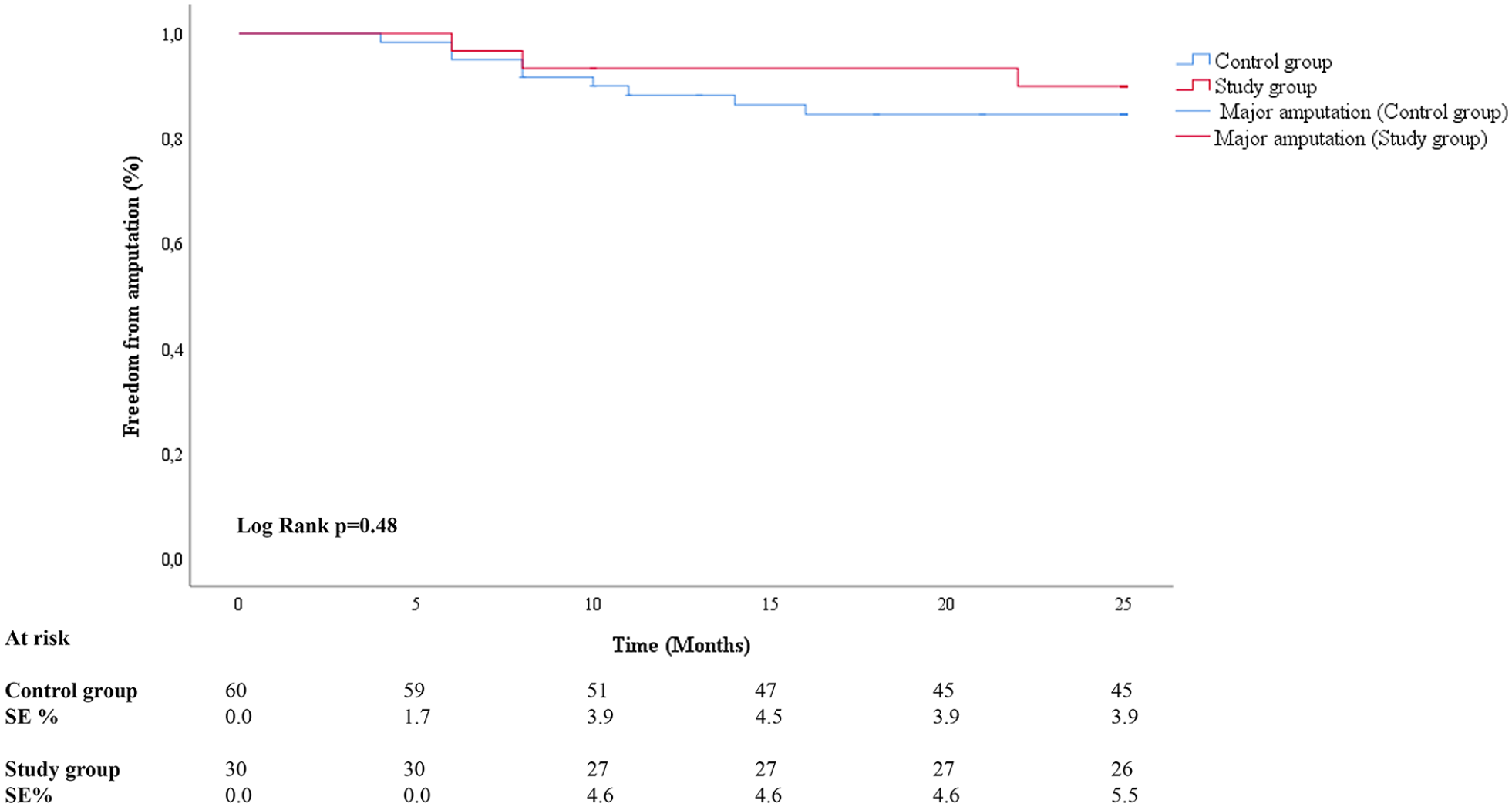
Freedom from amputation according to Kaplan-Meier method.
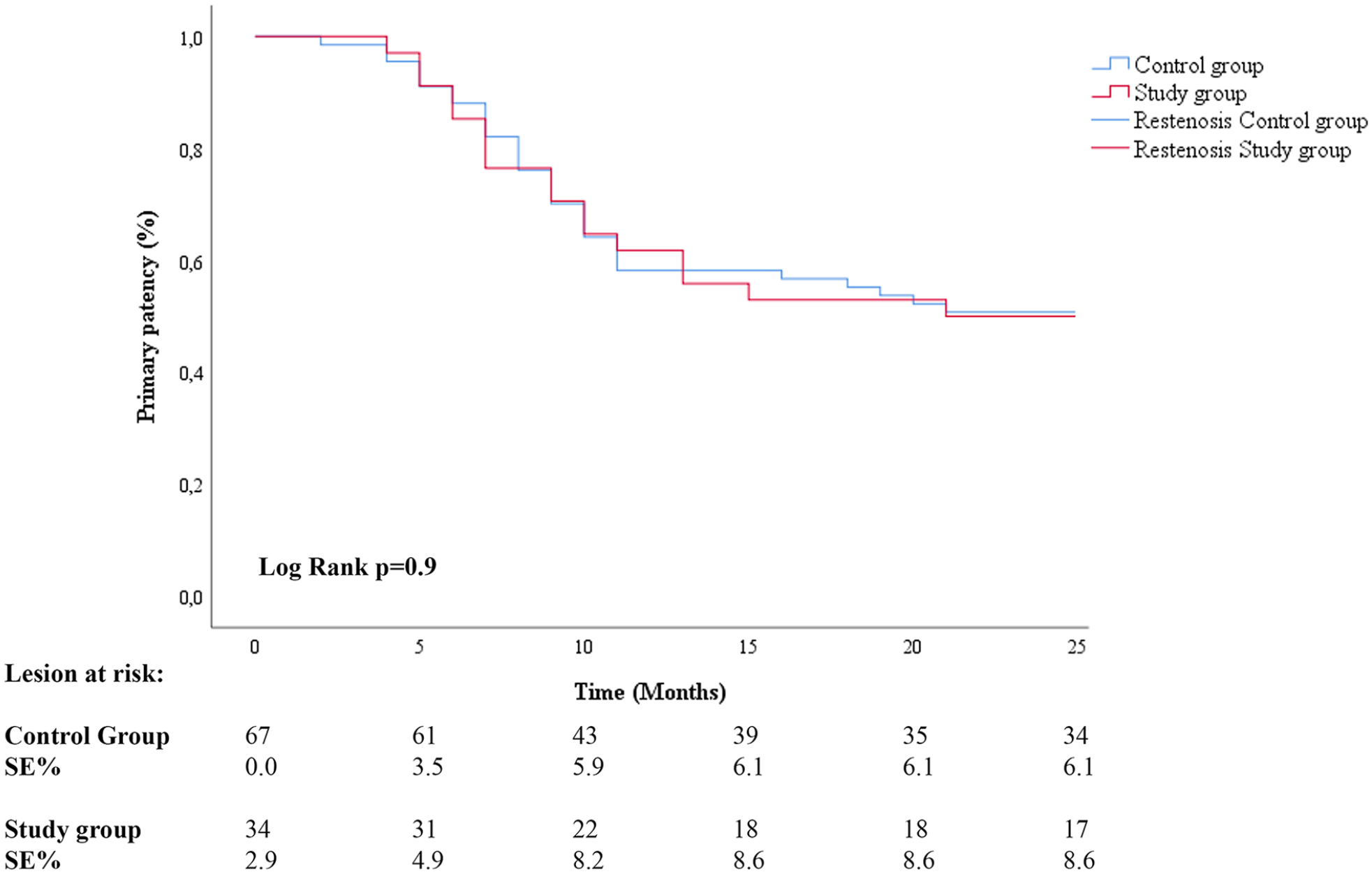
Primary patency according to Kaplan-Meier method.
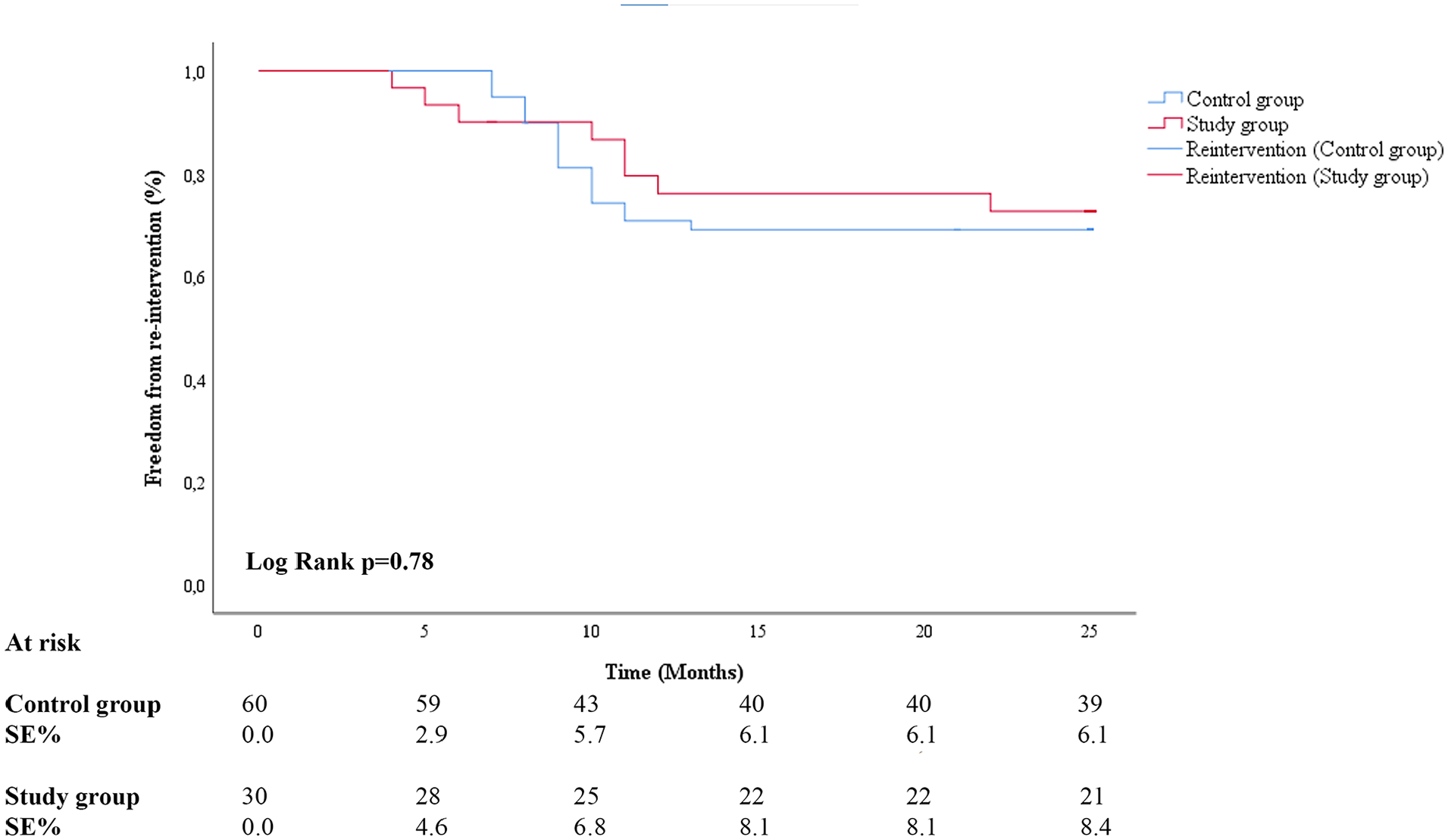
Freedom from re-interventions according to Kaplan-Meier method.
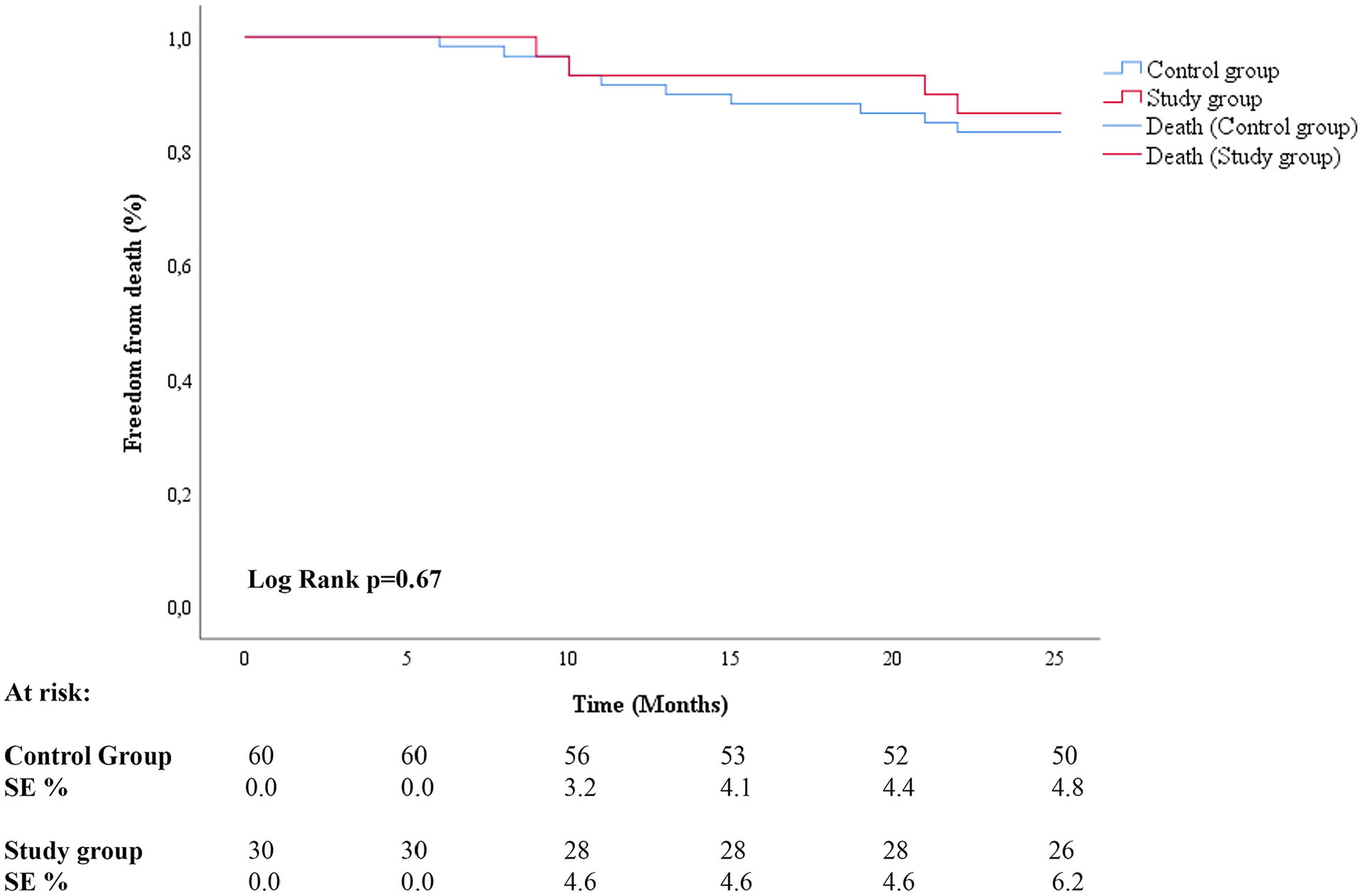
Freedom from death according to Kaplan-Meier method.
Discussion
In this retrospective study, we did not observe any difference in terms of patency when comparing the AFR re-entry using the dual guidewire balloon versus a conventional guidewire re-entry. In literature, technical success rate of conventional subintimal approach range between 74% and 94% for ATK lesions without the use of re-entry device10–13 and 82% and 98% for BTK lesions,2,3,5,7 with a variability that is dependent on operator skill and experience.
The dual guidewire balloon method of action is dilatation/deflation of the balloon in subintimal space to create fenestration, a passage/aperture in the intima that allows the advancement of the guidewire from the subintimal space into the true lumen. One aspect described by Carlino et al 8 as fundamental to obtain a successful guidewire re-entry in the true lumen is a quick advancement of a guidewire in the fenestration created after balloon dilatation/deflation before the virtual aperture naturally collapses on itself, after about 10-15 seconds. The dual guidewire balloon allows to quickly maneuver the advancement of the guidewire located inside the dual guidewire balloon shaft (second guidewire) from subintimal space into the true lumen through a created aperture.8,14 The location of the fenestration may be controlled by repositioning the dual guidewire balloon in subintimal space close to the distal CTO cap. If the first pass of guidewire re-entry through the created aperture into the true lumen is not successful, the dual guidewire balloon may be repositioned to a slightly different location or orientation, and balloon inflation/deflation and re-entry through a newly created aperture repeated. In our study group, we had to reposition the dual guidewire balloon 2 times in 5 cases. Such repositioning and inflation/deflation of the dual guidewire balloon is quick and safe. This is much different from a conventional technique where re-entry is obtained perforating the subintimal space with the guidewire. Such approach often causes extension of the created subintimal space and risk to extend the dissection distally with the involvement of important collaterals. In the control group of our study, 5 patients needed a surgical conversion due to the extension of the subintimal channel or a vessel rupture during the procedure.
In the study group, the antegrade fenestration with a dual guidewire balloon resulted in a fast and straightforward procedure compared with a conventional antegrade approach in the control group where in 14 patients (23% of cases) a retrograde approach was needed to complete the procedure. This could explain a significant prolongation of the procedural time and radiation exposure for the operators in patients who presented similar complexity of the lesions in terms of length and calcifications.
It is important to mention that subintimal re-entry approach with antegrade fenestration could be performed with a conventional low-profile balloon. After subintimal fenestration is created by inflating/deflating the balloon, the balloon needs to be withdrawn to allow the second guidewire entry into fenestration and the true lumen. Using the dual guidewire balloon, there is no need to withdraw the balloon to advance a re-entry guidewire into created fenestration. The second, re-entry guidewire is located inside the shaft of the dual guidewire balloon and can be advanced into fenestration without removing the balloon. Considering the fact that the subintimal fenestration created with a balloon lasts only for a few seconds, the use of a conventional low-profile balloon significantly limits the chance of a successful re-entry in the true lumen in a such short period of time.
It is worth noting that the Presto dual guidewire balloon device is very different than the Stingray device (Boston Scientific). The Stingray device is an over-the-wire catheter characterized by a flat winged balloon and 1 central lumen in connection with 2 side ports. Once the device is advanced beyond the CTO, the distal balloon is inflated and allows an orientation and stabilization of the catheter. A dedicated stiff angled guidewire may be advanced from the central lumen through the side ports under fluoroscopy to puncture the intima and to perform a re-entry after a subintimal recanalization. After the true lumen is re-entered the stiff guidewire is recovered and a soft tip guidewire is used to complete the procedure. The Presto dual guidewire balloon is inflated/deflated in subintimal space to create fenestration. The second re-entry guidewire is advanced from the second lumen inside of the Presto balloon shaft into created fenestration and in the true lumen. Also, the re-entry guidewire advancing from the Presto dual guidewire balloon shaft into fenestration has several degrees of torqueability and maneuverability allowing a quick catheterization of the fenestration. In the Stingray device, the re-entry guidewire is directed/limited by the lateral port position without much torque and movability, thus limiting its re-entry ability.
In our experience, we observed that the AFR approach with the dual guidewire balloon is safe, effective, and may significantly reduce procedural time and radiation exposure, compared with a conventional guidewire subintimal re-entry approach. In our study group, a total procedural time including 10 minutes of fluoroscopy time spent for first luminal or subintimal CTO crossing with a conventional technique was 41.1±10.8 minutes and fluoroscopy time was 16.7±3.5 minutes using the dual guidewire balloon catheter versus 146.6±62.3 minutes of procedural time and 34.3±14.2 minutes of fluoroscopy time in the control group using a conventional guidewire re-entry.
Use of a conventional guidewire subintimal re-entry almost always requires time consuming guidewire escalation and use of several different stiffness guidewires and additional microcatheters for guidewire support. The AFR using the dual guidewire balloon requires 1 balloon catheter and 2 conventional .014ʺ guidewires. It is important to mention that other expensive specialty devices such as the Outback catheter (Cordis, Santa Clara, CA, USA) or Stingray (Boston Scientific, Marlborough, Massachusetts, USA) are often used as bailout when a conventional guidewire subintimal re-entry is prolonged or fails.
The AFR using the dual guidewire balloon catheter improves safety of the subintimal re-entry procedure. It avoids the extravascular trans fixation of the adventitia and a perivascular hematoma at the re-entry point that frequently is created by other re-entry devices that could be oriented in the wrong direction creating an extravascular passage of the guidewire. No dual guidewire balloon–related complications were observed. Potentially, the dilation of the subintimal channel may cause a vessel rupture if a too large balloon is used. For that reason, it is important to use a correct 1:1 sizing of the balloon with vessel diameter to avoid this risk.
The antegrade fenestration re-entry with the Presto dual wire balloon to cross CTO is particularly interesting option for BTK lesions and may be a game changer to obtain a quick and successful recanalization once commercially available.
Limits of the Study
This study had all the limits of a retrospective cohort study. A propensity-matched analysis were performed in order to compare the study group treated with antegrade fenestration using the dual guidewire balloon and the control group treated in same period time with a conventional antegrade and retrograde approaches in order to reduce the bias related to lesions complexity, type of angioplasty and stent used, associated comorbidities and demographic variables.
Further evaluations with a prospective randomized experience are needed to define the efficacy and safety of the AFR using the dual guidewire balloon in daily practice. A comparison with an elective retrograde approach could be also interesting to evaluate efficacy and reliability of such approach. The economic impact should also be assessed, comparing procedural and fluoroscopy time, as well as overall cost of the AFR with the dual guidewire balloon compared with conventional guidewire re-entry approach and specialty re-entry devices.
The use of the Presto dual guidewire balloon, which is based on a 0.014ʺ guidewires may be considered not convenient by operators routinely using 0.018ʺ or 0.035ʺ guidewire for superficial femoral artery disease. However, more and more operators are mimicking cardiac procedures using 0.014ʺ guidewires to perform CTO recanalization, and once the recanalization have been obtained, use a guidewire of their preferences for the final step of the procedure.
Conclusion
In our experience, the AFR approach using a dual guidewire balloon is a step forward for crossing CTO. This technique simplifies the treatment of challenging peripheral lesions in BTK and ATK by significantly reducing procedural time and x-ray exposure for interventionists and patients without an increase of procedural risk and compromising clinical outcome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.