
Abstract
Purpose:
To describe the technical aspects and early results of a new endovascular fenestration method for false lumen occlusion in chronic aortic dissection: the Knickerbocker Technique.
Methods:
A retrospective observational study including all consecutively treated patients between November 1, 2012, through May 31, 2016, who underwent thoracic endovascular aortic repair with false lumen occlusion using the Knickerbocker Technique for thoracic false lumen aneurysm in chronic aortic dissection in a tertiary care center. Primary endpoints consisted of technical (correct deployment of the stent-graft) and clinical (false lumen occlusion) success. Secondary endpoints included overall survival and morbidity after 30 days. In 12 patients, follow-up computed tomography angiogram (CTA) was available and aortic remodeling was evaluated.
Results:
We identified 16 eligible patients (75% men, mean age: 69 years, range: 52–80 years). Technical success was 94%. Overall survival after 30 days was 100%; there was 1 aortic reintervention (additional false lumen embolization due to endoleak type 1a in 1 patient). Median total follow-up was 31.5 months (range: 3–66 months). Four (25%) of 16 patients died during follow-up, in 3 of those patients the cause of death is unknown, and 1 patient developed cardiac tamponade after being treated by fenestrated thoracic endovascular aortic repair. Imaging follow-up with CTA was available in 12 patients (median imaging follow-up: 27.5 months, range: 1–57 months). Nine (75%) of 12 patients showed thoracic aortic remodeling, and in 3 patients aneurysm size was stable. No patient showed aneurysm growth.
Conclusion:
The Knickerbocker Technique is a feasible endovascular fenestration method to achieve false lumen occlusion and aortic remodeling in chronic aortic dissection with low invasiveness.
Introduction
Chronic aortic dissection is a complex disease that needs different treatment strategies compared with acute or subacute aortic dissection.1,2 Thrombosis of the false lumen is the key to successful aortic remodeling. 3 Besides open strategies of false lumen occlusion, which are associated with high rates of morbidity and mortality, several promising endovascular concepts were developed to achieve false lumen thrombosis.4–6 In patients with a false lumen aneurysm only in the thoracic aorta, strategies to prevent false lumen back-flow limited to the thoracic segment may have a lower risk of spinal cord ischemia (SCI) compared with a full thoracoabdominal coverage necessary in fenestrated/branched endovascular aortic repair (f/bEVAR). The Knickerbocker Technique was introduced in 2012 and represents an endovascular fenestration method to achieve false lumen occlusion proximal to the celiac trunk. 7
Since the first description of this technique in 2014, the Knickerbocker graft has been used as a custom-made device (CMD).
This study describes indication, technical aspects, and early results of this new endovascular technique for false lumen occlusion in chronic aortic dissection.
Methods
Study Design
A retrospective single-center observational study was conducted between November 1, 2012, and May 31, 2016. All consecutive patients with thoracic false lumen aneurysm and false lumen back-flow due to distal entries in chronic aortic dissection, who were treated with the Knickerbocker Technique for false lumen occlusion, were included. Treatment indications included false lumen aneurysm of >5.5 cm (total aortic diameter) or rapid diameter progression. 8 The Knickerbocker Technique was performed as described below. Included patients had suitable anatomy with a maximum aortic diameter above the celiac trunk of 45 mm.
The Knickerbocker Technique—Stent-Graft Design, Deployment, and Requirements for Use
The Knickerbocker stent-graft (Cook Medical, Bjæverskov, Denmark) is a double-tapered tubular endograft that is constructed of woven polyester fabric sewn to self-expanding nitinol stents with braided polyester and monofilament polypropylene sutures. The Knickerbocker graft is deployed into the true lumen above the celiac trunk with a sufficient proximal diameter and overlap to the proximal stent-graft. The asymmetrical bulbous section is marked with gold markers to orient it toward the dissection membrane and allow for correct orientation. Dilatation of this expandable portion using a compliant balloon fenestrates the dissection membrane and allows expansion of the stent-graft to the outer aortic wall preventing back-flow to the thoracic false lumen proximal to the reno-visceral segment (Figure 1). The distal diameter of the graft is chosen according to the crescent length of the true lumen to prevent a distal stent-graft-induced new entry-tear (SINE). The bulbous section has 1 full non-tapered stent in the middle to expand to the outer aortic wall. The diameter at this level should not exceed the maximum diameter of the complete aorta at the intended sealing area. Two tapered stents frame the larger stent above and below to complete the double-tapered structure of the graft. The bulbous section is planned to seal the false lumen about 5 cm proximal to the celiac trunk. The maximum diameter of the bulbous section is 46 mm. The size of the compliant balloon is chosen accordingly. The Knickerbocker graft is loaded on a 20 or 22F Z-Trak Plus hydrophilic Introduction system (William Cook Europe, Bjaeverskov, Denmark).
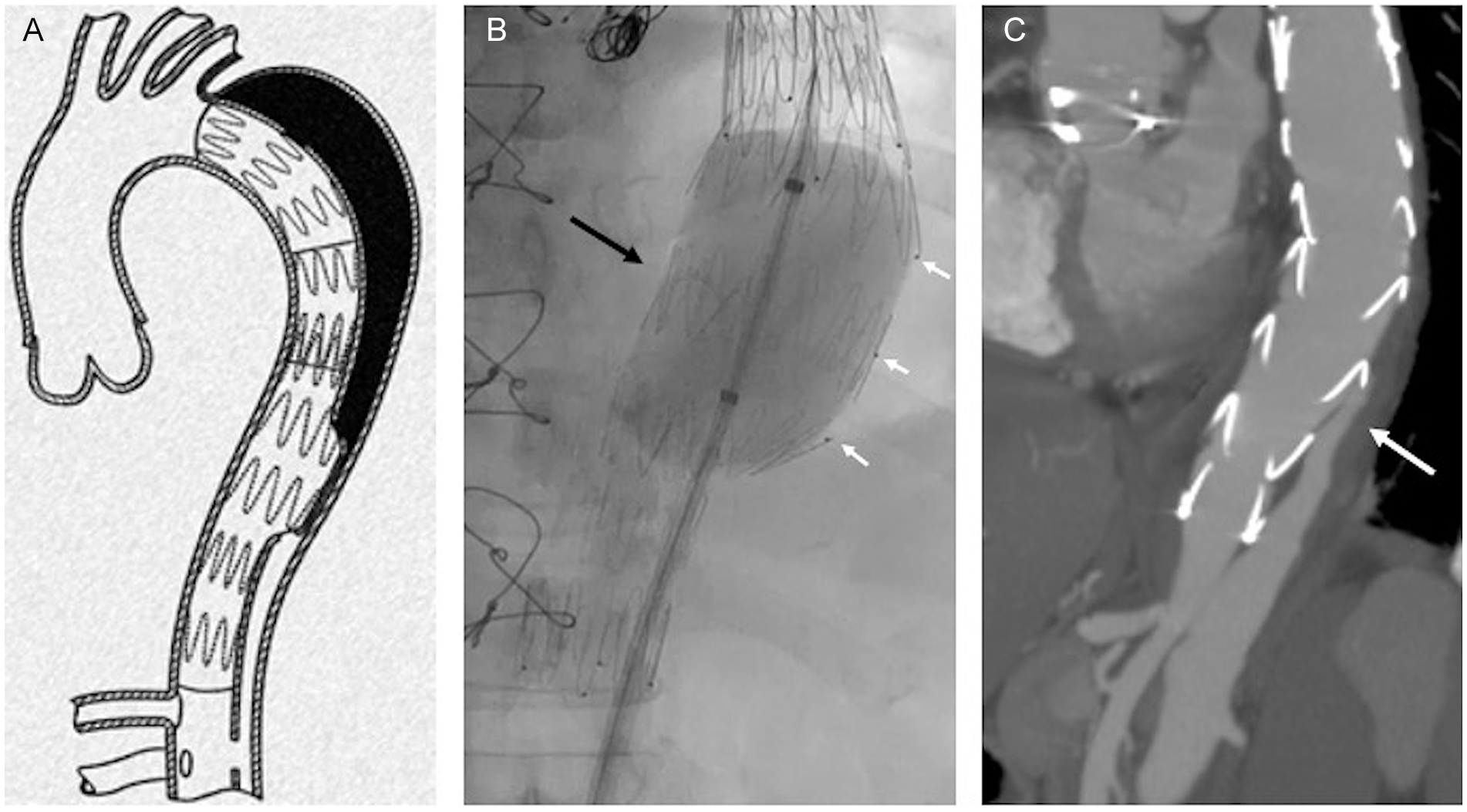
(A) Draft of the Knickerbocker stent-graft and its positioning with the double-tapered section above the celiac artery. The tapered portion of the graft should face toward the dissection membrane to rupture it locally and achieve attachment of the graft to the outer aortic wall, and (B) fluoroscopy image showing expansion of the tapered segment of the Knickerbocker stent-graft with a compliant balloon (black arrow). The gold markers (small white arrows) are oriented correctly toward the false lumen, and (C) postoperative computed tomography angiogram in maximum intensity projection (MIP) demonstrating sufficient seal of the Knickerbocker graft with prevention of false lumen back-flow to the thoracic aorta (white arrow).
After access to the true lumen is confirmed by digital subtraction angiography (DSA) and an extra-stiff Lunderquist guidewire (William Cook Europe) is placed in the ascending aorta, the Knickerbocker graft is advanced and the bulbous section is directed toward the dissection flap and the false lumen, using the gold markers and an adequate projection derived from a preoperative CTA. The device is deployed in a standard fashion landing just proximal to the celiac trunk. Access to the false lumen is not required and the Knickerbocker Technique can also be applied, if the false lumen is partially or fully thrombosed above the double-tapered segment required in contrast to the Candy-Plug technique. 9
Endpoints and Definitions
Primary endpoints consisted of technical and clinical success. Technical success was defined as correct and uncomplicated placement of the Knickerbocker stent-graft at the intended level with correct orientation. Clinical success was defined as complete elimination of false lumen back-flow at the bulbous segment of the Knickerbocker graft on final DSA and on postoperative CTA. Secondary endpoints included mortality after 30 days, complications, and aortic remodeling in patients with available follow-up CTA >30 days.
Data Collection
Retrospective data collection included the following:
Demographic patient information and comorbidities
Type of dissection (Stanford Classification), previous aortic history, symptom status, treatment indication, and urgency of procedure.
Procedural information, stent-graft dimensions, adjuvant embolization, additional thoracic endovascular aortic repair (TEVAR), and intraoperative technical and clinical success.
Thirty-day outcome including postoperative complications (stroke, spinal cord ischemia, myocardial infarction) or death, reintervention with false lumen embolization at the Knickerbocker level, postoperative outcome on early CT scan regarding stent-graft position, aortic diameter, and false lumen back-flow.
Overall survival, reintervention, and aortic remodeling during follow-up (FU). For the evaluation of aortic remodeling, anatomical measures included the largest thoracic perpendicular aortic diameter including false and true lumen after Knickerbocker treatment on the first postoperative CT scan compared with the most recent CT scan >30 days if available. A change in aortic diameter of more than 3 mm was defined as an increase or decrease. Changes of 3 mm or less were considered as stable.
Data Analysis
All data were anonymized and analyzed for the primary and secondary endpoints as defined above. For the statistical analysis, continuous variables are expressed as medians with minimum–maximum range. Categorical variables are presented as percentages. Statistical analysis was performed using SPSS (IBM SPSS Statistics for Macintosh, Version 25.0).
Results
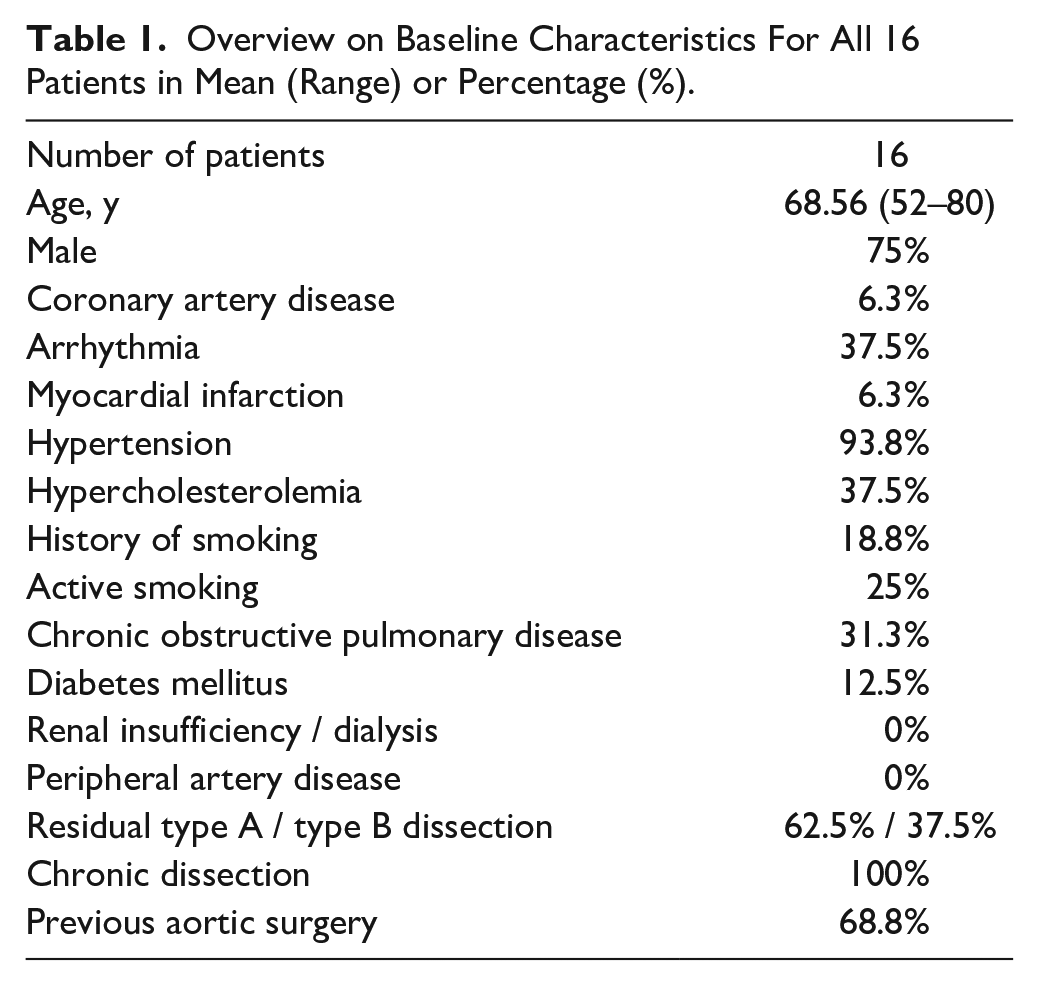
From November 1, 2012, through May 31, 2016, 16 consecutive patients (75% men, mean age: 69 years, range: 52–80 years) underwent elective false lumen occlusion with the Knickerbocker Technique. Treatment indications included false lumen aneurysm of >5.5 cm in 12 patients (total aortic diameter) and rapid diameter progression in 4 patients. Overview of the demographic data is given in Table 1.
Overview on Baseline Characteristics For All 16 Patients in Mean (Range) or Percentage (%).
Disease-Specific Features
Residual type A aortic dissection (TAAD) was present in 10 (62.5%) patients, while 6 patients (37.5%) had type B aortic dissection (TBAD). All patients had chronic aortic dissection >90 days after the initial event. Eleven patients (68.8%) had previous aortic operations including 7 open supra-coronary ascending or hemiarch replacements of the aorta. Two patients had previous TEVAR procedures and 2 patients had both previous open repair and TEVAR. Five patients had no previous aortic repair. No patient presented with malperfusion or rupture.
Early Outcomes
Additional intraprocedural false lumen embolization with coils and glue at the Knickerbocker level was needed in 5 patients (31.3%) due to persisting false lumen back-flow. Additional TEVAR proximal to the Knickerbocker graft was performed in 10 patients (62.5%). Three (18.8%) of those patients had fenestrated TEVAR with fenestration and/or a scallop for the left subclavian artery and/or the left common carotid artery, and 5 (31.3%) received branched TEVAR with branches for the innominate artery and the left common carotid artery.
Technical success was 93.8% with 1 stent-graft being malrotated. Initial clinical success was 75% with 12 patients showing no false lumen back-flow on final angiogram. There was 1 intraprocedural complication with coverage of the celiac trunk in 1 patient requiring implantation of a covered stent. This was not associated with the bulbous section of the Knickerbocker graft or the use of the compliant balloon but with a too distal landing of the stent-graft above the celiac trunk.
30-Day Postoperative Course
The 30-day postoperative CT scan was available in all patients, and successful Knickerbocker placement at the intended level was confirmed in all patients except the one with the malrotation (93.8%). Complete distal false lumen occlusion was present in 15 patients (93.8%) with only mild back-flow in 1 patient not requiring reintervention.
During 30-day postoperative follow-up of all 16 patients, no deaths occurred. There were 4 adverse events: 1 patient with spinal cord ischemia (SCI), 1 patient who developed severe inflammatory response syndrome (SIRS), and 2 patients with bleeding from the femoral vessels at the puncture site needing reintervention. There were no reinterventions in association with false lumen embolization at the Knickerbocker level. In addition to the 2 reinterventions at the access vessels, there was 1 more reintervention needed for proximal false lumen embolization due to endoleak type Ia, so the total number of reinterventions was 3 (18.75%). Mean stay on intensive care unit stay was 3 days (range: 2–7 days).
Midterm-Outcomes
Median follow-up was 31.5 months (range: 3–66 months). Four (25%) of 16 patients died during FU, 1 patient suffered retrograde TAAD after a fenestrated TEVAR procedure, in 2 patients the cause of death was unknown, and 1 patient died due to aortic rupture but no details were known. Two patients (12.5%) had false lumen embolization at the thoracic level due to type Ia endoleak. Two patients (12.6%) received a planned distal extension with f/bEVAR due to large abdominal false lumen aneurysm. Other aortic reinterventions in 2 patients (37.6%) included fenestrated TEVAR (as mentioned above with the complication of cardiac tamponade and death) and stenting of 1 renal artery.
Twelve patients had available CT FU (median CT FU: 27.5 months, range: 1–57 months). Of those 12 patients, 3 (25%) showed stable aneurysm size and 9 (75%) had aortic remodeling with a diameter reduction >3 mm (Figure 2). There was no aortic growth (Table 2).
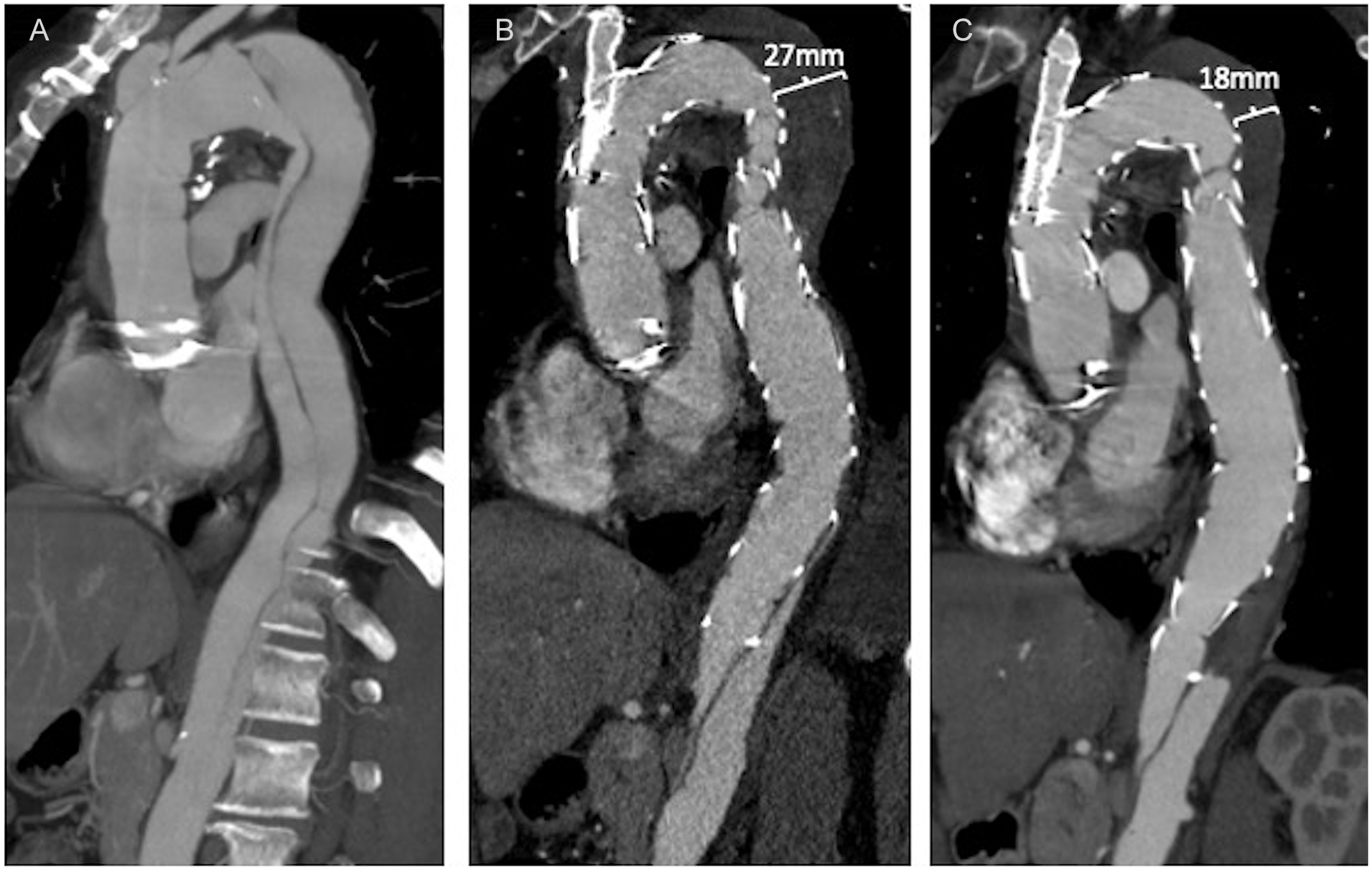
Multiplanar reconstruction (A) of initial presentation of a residual TAAD after open Bentall-Repair, (B) after Knickerbocker repair as distal extension in combination with branched arch repair showing complete false lumen occlusion of the thoracic aortic segment, and (C) 1-year FU of the same patient showing good remodeling of the thoracic false lumen aneurysm.
Overview of the Development of Thoracic Aneurysm Diameters in 12 Patients With Imaging Follow-up (FU) Beyond 30 Days (Median Imaging Follow-up: 27.5 Months, Range: 1–57 Months) in Ascending Order of Follow-up Time.
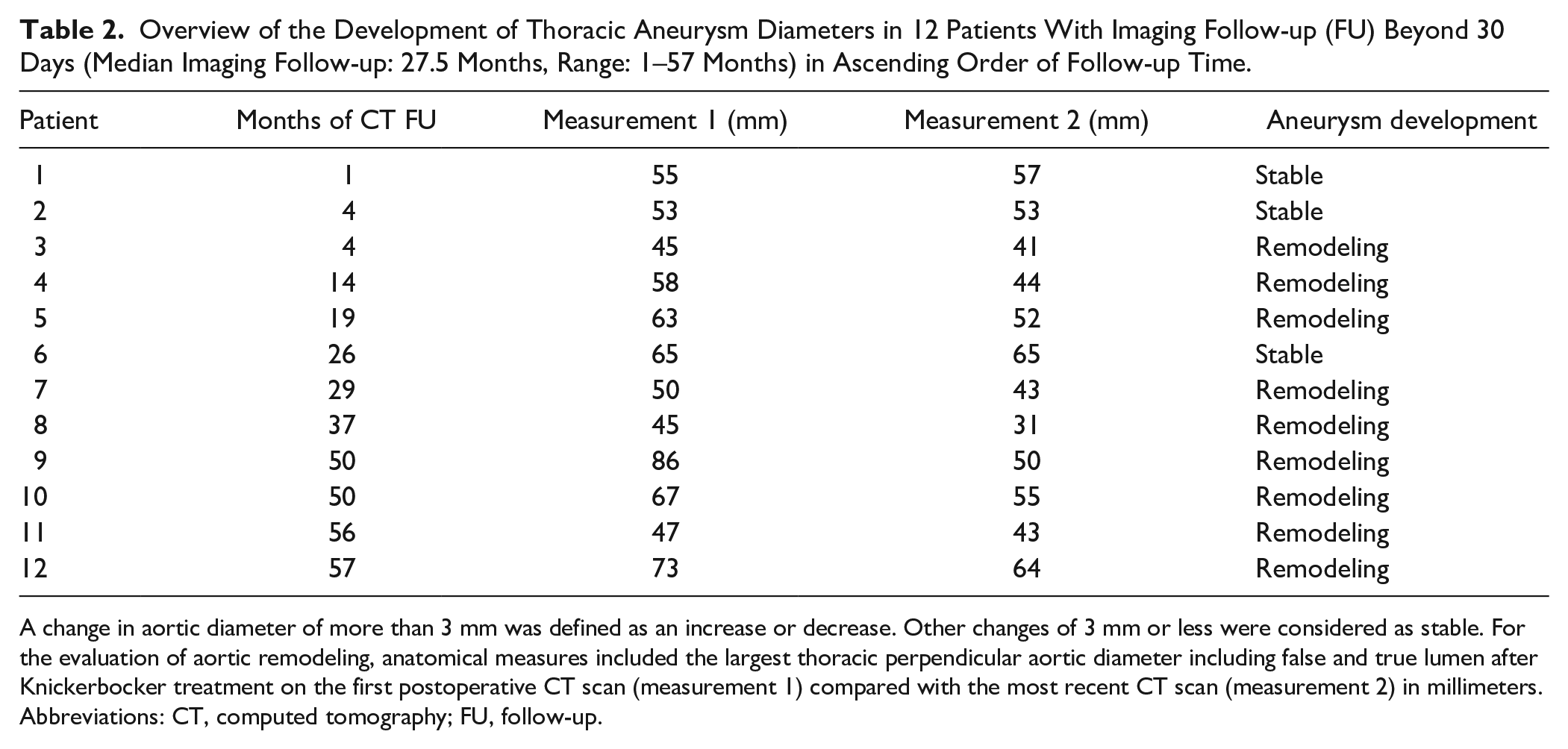
A change in aortic diameter of more than 3 mm was defined as an increase or decrease. Other changes of 3 mm or less were considered as stable. For the evaluation of aortic remodeling, anatomical measures included the largest thoracic perpendicular aortic diameter including false and true lumen after Knickerbocker treatment on the first postoperative CT scan (measurement 1) compared with the most recent CT scan (measurement 2) in millimeters.
Abbreviations: CT, computed tomography; FU, follow-up.
Discussion
Our results describe the technical feasibility of the Knickerbocker Technique with correct orientation of the bulbous segment toward the false lumen in 15 of 16 cases and an acceptable early clinical success rate of complete false lumen back-flow elimination in final angiogram and on postoperative CT scan. The characteristic of the Knickerbocker Technique is the complete endovascular strategy to fenestrate the dissection membrane and to extend the covered stent-graft to the outer wall of the aorta above the celiac trunk. In chronic TBAD or residual TAAD, false lumen aneurysm characteristically develops in the descending thoracic aorta while the abdominal segment remains non-aneurysmal. 10 In those patients, the Knickerbocker approach offers a treatment strategy avoiding coverage of longer aortic segments, thus lowering the risk of SCI compared with other techniques for occlusion of the false lumen, including f/bEVAR. 11 One patient suffered a major complication with symptoms of SCI, despite the limited thoracic aortic coverage to the celiac trunk.
Two patients received distal extension with f/bEVAR during FU; in those patients, the Knickerbocker Technique allowed a staged approach ahead of long aortic coverage; both patients did not suffer any neurological symptoms. Another strategy to achieve false lumen occlusion at the thoracic segment is the Candy-Plug technique using a covered obstructive large-diameter stent-graft into the false lumen in addition to TEVAR extension to the celiac trunk. The Candy-Plug technique is associated with shorter procedural times and lower radiation exposure compared with f/bEVAR. 12 The Knickerbocker Technique does not require the extra step of false lumen catheterization, which may be less time-consuming. But additional false lumen catheterization might be needed for coil embolization at the Knickerbocker level if false lumen back-flow is still seen on final angiogram. A significant proportion of cases (%) required additional embolization measures to seal the false lumen back-flow. One patient of those 5 had malrotation of the graft with the bulbous section not facing correctly to the false lumen, which explains the reason for persistent back-flow.
Despite potential theoretical advantages of the Knickerbocker Technique, our institutional policy has moved toward the use of Candy-Plug technique in suitable cases from 2016.
Limitations of our study are small patient numbers and limited FU with just 12 of 16 patients with available CTA. Also, the Knickerbocker Technique and the device are not approved and used as a CMD. Application of this technique has to be weighed against the advantages of other strategies in every single patient.
Conclusion
The Knickerbocker Technique is a feasible endovascular fenestration method to achieve thoracic false lumen occlusion in chronic aortic dissection associated with a high rate of aortic remodeling and an acceptable rate of morbidity and mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tilo Kölbel and Nikolaos Tsilimparis act as proctors for Cook Medical. Tilo Kölbel has IP with Cook Medical. He also receives travel and research grants from Cook Medical. Otherwise, there is no conflict of interest for this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.