
Abstract
Purpose:
To perform a systematic review assessing the safety and efficacy of percutaneous transluminal angioplasty (PTA) for treatment of critical hand ischemia (CHI) due to below-the-elbow (BTE) obstructive arterial disease.
Materials and Methods:
MEDLINE and EMBASE systematic searches were performed from inception to December 2020 to identify studies assessing PTA for management of BTE obstructive arterial disease. Three independent reviewers performed abstract selection, data extraction, and quality assessment. The Newcastle-Ottawa Scale was used to assess individual study bias for non-randomized controlled trials.
Results:
Eight studies comprising 176 patients with obstructive BTE vessel disease were included. All studies had a score >5 on the Newcastle-Ottawa Scale, indicative of high quality. All studies used low-profile balloons (1.5–4 mm) for PTA of stenotic lesions or chronic total occlusions (CTOs). The weighted average technical success and clinical success rates were 89.3% (range = 82%–100%) and 69.9% (range = 19%–100%), respectively, at a mean follow-up of 29.7 ± 17.1 months. The short-term (<30 days) complication rate was low at 4.7% and most commonly included access site hematomas, pseudoaneurysms, and radial artery perforation or re-thrombosis. Nearly 20% of patients required an amputation, and most (96%) were minor (either distal phalanges or digits). Only 2 patients required above-wrist amputations. The primary and secondary patency rate at 5 years were 38% and 54%, respectively. The cumulative 5-year mortality rate was 33.1%.
Conclusions:
PTA for CHI due to BTE obstructive arterial disease is feasible with a high technical success rate and a low short-term complication rate. Additional long-term comparative studies are required to unequivocally establish the clinical benefit of endovascular treatment compared with conservative management or surgical bypass.
Keywords
Introduction
Critical hand ischemia (CHI) secondary to below-the-elbow (BTE) obstructive arterial disease can be debilitating and lead to amputation.1-3 Patients generally manifest with rest pain, non-healing ulcers, and progressive gangrene of the digits. BTE artery disease is common in patients with diabetes mellitus and chronic kidney disease.4,5 There is usually a diffuse involvement of the BTE vessels, including the ulnar artery, radial artery, palmar arch, and digital vessels, with seldom isolated involvement of the interosseous artery.4-10 Distal calcific arteriosclerosis plays a pivotal role in the pathophysiology of hand ischemia, particularly in hemodialysis patients. 5
Currently, there is no consensus algorithm regarding the most appropriate revascularization strategy for patients with CHI due to BTE vessel disease. The extensive multivessel involvement seen in many of the patients with CHI limit the procedural efficacy of surgical bypass due to improper landing zone or inadequate distal run-off. 11 Alternative non-revascularization strategies aimed at symptomatic relief, such as thoracic or palmar sympathetectomy, have been described in CHI.12,13 In the last 2 decades, several studies have shown promising results with percutaneous transluminal angioplasty (PTA) of BTE arteries for the management of CHI.3,4,6-10,13 This systematic review aims to assess the feasibility, technical success, long-term outcomes, and complications of PTA for the treatment of CHI due to BTE arterial disease.
Materials and Methods
This systematic review was performed in accordance with a protocol developed a priori and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 Institutional ethics board approval was not required.
Eligibility Criteria
Study inclusion criteria were as follows: (1) human study; (2) English language; (3) prospective or retrospective study with 4 or more patients presenting with CHI due to BTE vessel disease; (4) intervention involving PTA of one or multiple BTE vessels; (5) with at minimum reported outcomes on technical success and complications. Exclusion criteria were as follows: (1) CHI due to vasculitis or connective tissue disorders in the majority of patients; (2) history of surgical or endovascular revascularization; (3) case reports and conference or meeting abstracts.
Systematic Search and Data Abstraction
The MEDLINE (1946 to December 24, 2020) and EMBASE (1947 to December 24, 2020) databases were searched for all studies assessing the feasibility, safety and efficacy of PTA of BTE vessels for patients with CHI. The detailed search strategy is shown in Supplementary Figure 1. Secondary searches were conducted by two reviewers (S.A.K. and S.M.) assessing reference lists from primary studies and review articles to identify additional relevant studies. Three reviewers (G.A.E., S.A.K., and S.M.) independently screened titles and abstracts found in the primary and the secondary literature searches. Following initial abstract screen, full texts of the remaining studies were independently reviewed. Inter-reviewer disagreements were rectified by consensus. Data extraction was carried out in duplicate by G.A.E. and S.A.K. into a standardized spreadsheet. The following data were extracted: author, publication date, number of patients, number of interventions, mean age, gender, underlying etiology of CHI, clinical presentation, onset of symptoms to intervention, vessels treated, access artery, sheath size, guidewires used, balloons used, technical success, post-procedural complications, hemostasis method, and outcomes reported in follow-up.
Quality and Strength of Recommendation Assessment
Individual study bias was assessed using the Newcastle-Ottawa Scale for non-randomized controlled trials. The Newcastle-Ottawa Scale is a 9-point rating scale with 4 points for study selection, 2 points for study comparability, and 3 points for study outcome assessment. 15 A score >5 is indicative of high quality. Study quality assessment is presented in Supplementary Table 1. All studies had a score >5, which is indicative of high quality.
Statistical Analysis
Microsoft Excel (Washington, USA) was used for data tabulation. Study characteristics and outcomes data, including odds and hazard ratios, were presented as reported in the original articles. The weighted average for technical success, clinical success, as well as complication rates were calculated using Microsoft Excel and presented with the range. Cumulative mortality rates were tabulated at 14 months, 36 months, and 60 months based on the data reported in the original articles.
Results
Literature Search and Study Selection
Results of the literature review strategy are summarized in Figure 1. Of the 3169 abstracts identified, 3127 were excluded and 42 underwent full-text review. Following full-text review, 8 articles remained that met the previously specified eligibility criteria.3,4,6-10,13
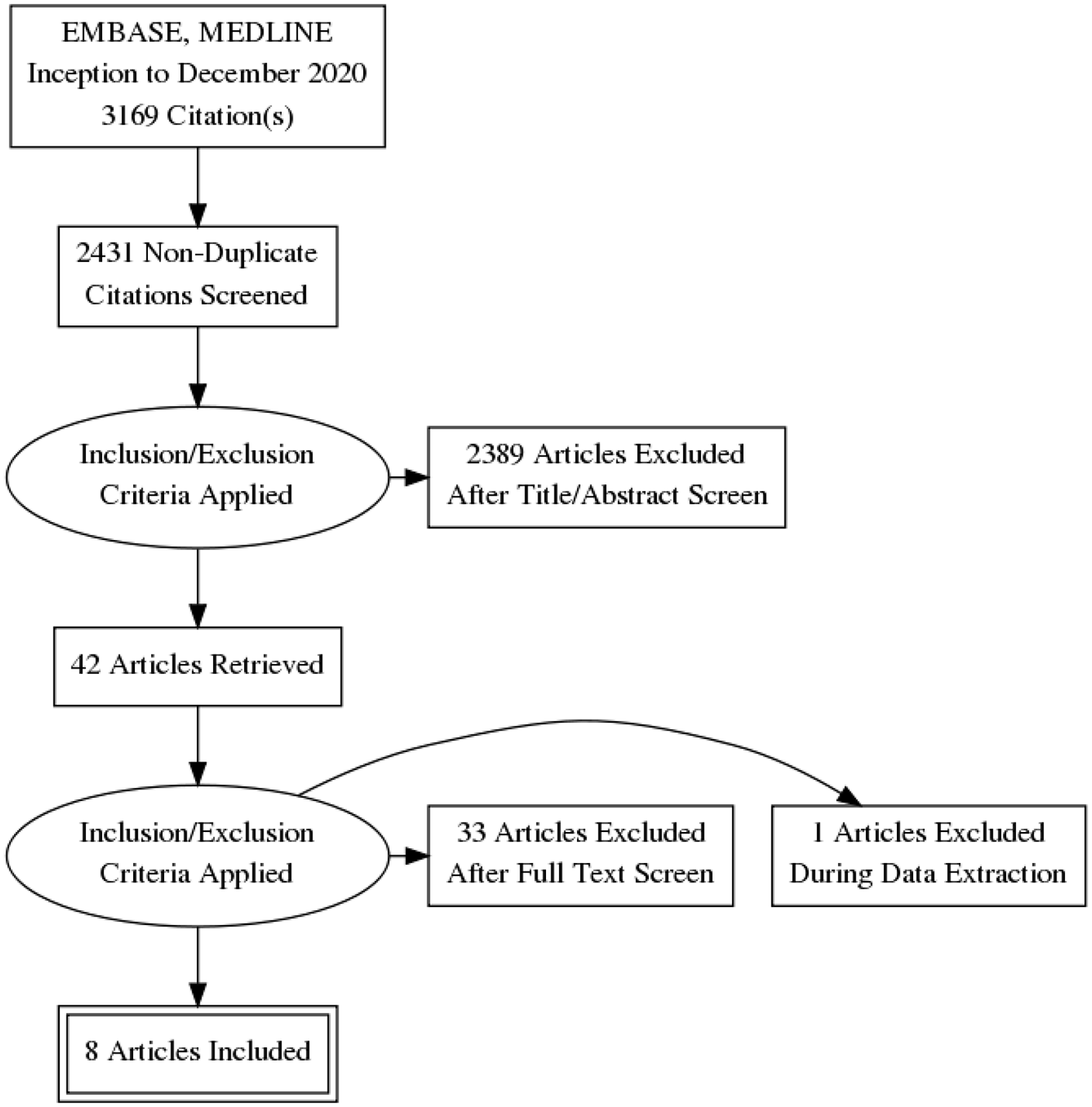
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Study Characteristics
Patient, intervention, and outcome characteristics of the included studies are presented in Table 1. There were 176 patients with BTE arterial disease, 55% males, mean age ranging from 53 to 64 years, and with multiple comorbidities, primarily hypertension (86%), peripheral vascular disease (68%), dyslipidemia (63%), chronic kidney disease or ESRD (55%), diabetes (55%), and coronary artery disease (50%). Also, 71% of the patients had a significant smoking history. With respect to CHI clinical presentation, 51% presented with rest pain, 31% with tissue loss or gangrene, and 22% with ulcers. Only 16 (12.5%) patients had active ipsilateral pre-existing AVF for hemodialysis (8 brachiocephalic and 8 radiocephalic).3,4,10
Study Characteristics.
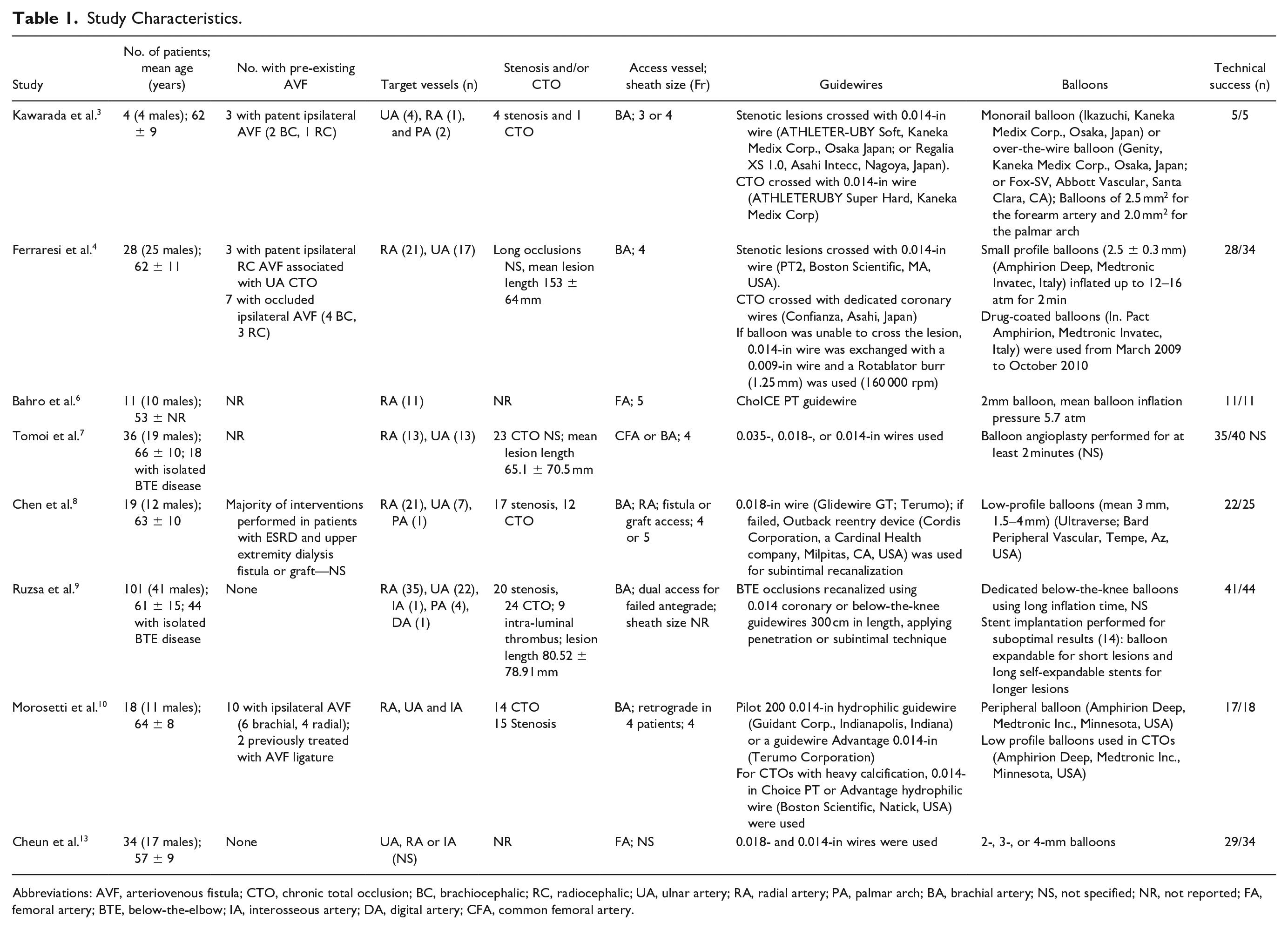
Abbreviations: AVF, arteriovenous fistula; CTO, chronic total occlusion; BC, brachiocephalic; RC, radiocephalic; UA, ulnar artery; RA, radial artery; PA, palmar arch; BA, brachial artery; NS, not specified; NR, not reported; FA, femoral artery; BTE, below-the-elbow; IA, interosseous artery; DA, digital artery; CFA, common femoral artery.
Technique and Technical Success
BTE revascularization was commonly performed for radial and/or ulnar artery disease, and seldom for isolated interosseous artery, palmar arch, or digital artery disease (Table 1). Revascularization was achieved or initially attempted predominately using an antegrade brachial puncture and 4- or 5-Fr vascular sheath.3,4,7-10 Other alternatives used in failed antegrade brachial cases included dual access (for example, femoral and radial artery, or radial artery/palmar arch), 9 fistula/graft access, 8 retrograde transradial access, 10 or the palmar-loop-technique.2,16 Two studies exclusively used the femoral artery for access.6,13 The total number of patients who had femoral artery access was 86 (40%).
All studies used 0.014- or 0.018-in guidewires to cross stenotic lesions or chronic total occlusions (CTOs), with low-profile balloons (1.5–4 mm) for PTA. If the guidewire failed to cross the lesion, other alternatives used were stiffer 0.014-in guidewire, 3 dedicated coronary wires, 4 0.009-in wire with atherectomy of calcified plaque using a Rotablator (Boston Scientific, MA, USA), 4 or subintimal recanalization technique.8,9 One study exclusively explored the Diamondback 360 Peripheral Orbital Atherectomy System (OAS) (Cardiovascular Systems, Inc., MN, USA) for crossing BTE CTOs. 6 The total number of patients who had atherectomy was 13 (7.4%).
Drug-eluting balloons were used in one study for primary revascularization, 4 and in another study for management of restenosis. 9 The number of patients who had drug-eluting balloons was either not reported 4 or not specified. 9 Stents were used in one study for BTE revascularization due to suboptimal results with PTA alone (sluggish flow and/or residual stenosis between 30% and 50%), with either balloon expandable stents for short lesions or self-expandable stents for long lesions. 9
Seven of eight studies defined technical success as revascularization of the target vessel with residual stenosis ≤ 30%. Only one study defined technical success as establishing straight-line flow to the hand with final residual diameter stenosis ≤ 50% for balloon angioplasty alone. 7 The weighted average technical success rate was 89.3% (range = 82.4%–100%).
Four studies provided data on restenosis and the weighted average restenosis rate was 29.2% (range = 18%–44%) at 6–48 months follow-up.4,9,10,13 In the Ruzsa et al study, 14 patients had stent implantation for primary revascularization due to suboptimal results from PTA alone. 9 The stent or balloon restenosis rate in this study was 14.3% versus 13.3% at 1 year follow-up, and this was not statistically significant in the study.
Clinical Success and Long-Term Outcomes
Definitions for clinical success and outcomes varied among the studies and they are summarized in Supplementary Table 2. Short and long-term study outcomes are presented in Table 2.
Study Outcomes and Restenosis Data.
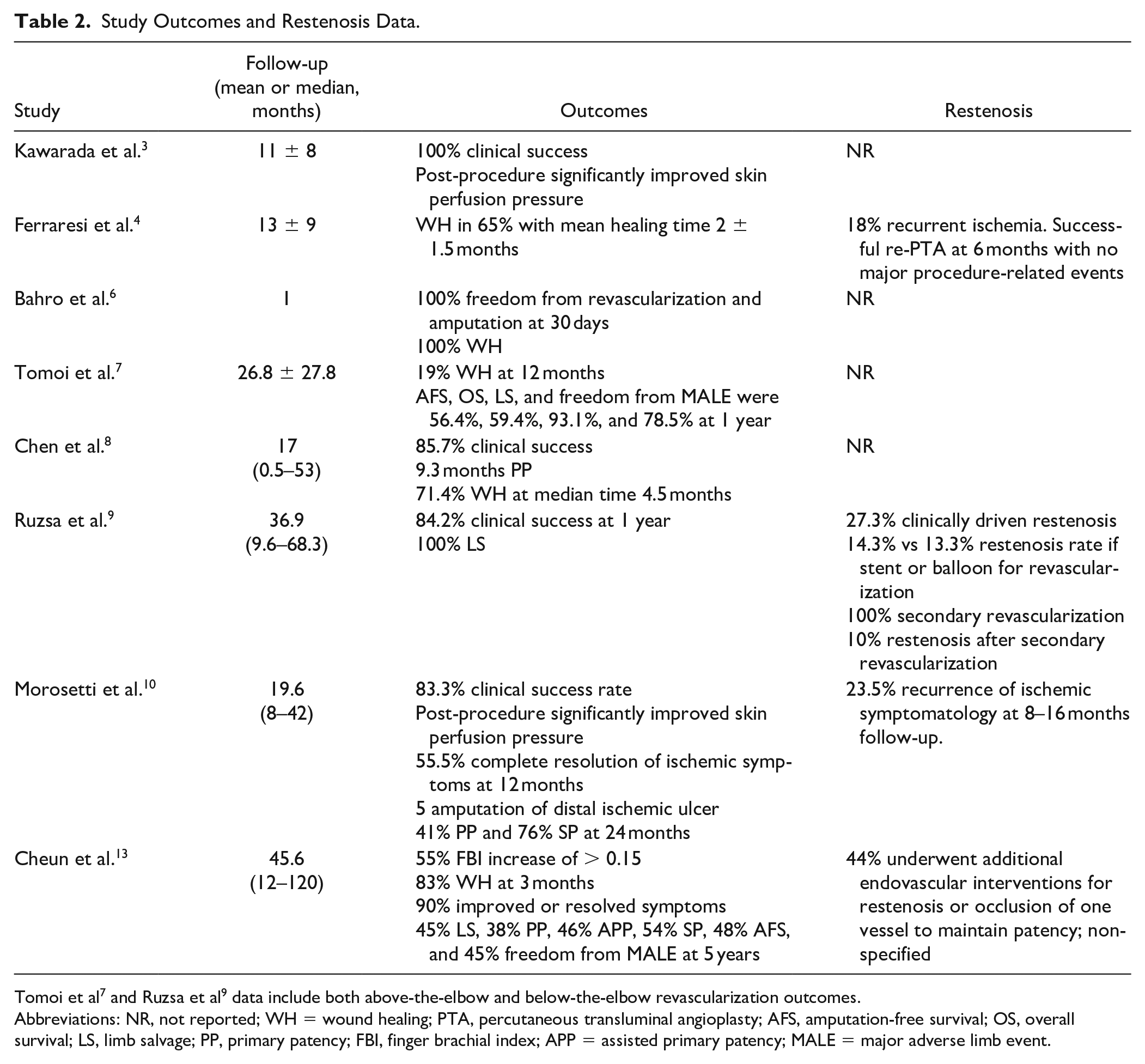
Tomoi et al 7 and Ruzsa et al 9 data include both above-the-elbow and below-the-elbow revascularization outcomes.
Abbreviations: NR, not reported; WH = wound healing; PTA, percutaneous transluminal angioplasty; AFS, amputation-free survival; OS, overall survival; LS, limb salvage; PP, primary patency; FBI, finger brachial index; APP = assisted primary patency; MALE = major adverse limb event.
Post-revascularization mean follow-up was 29.7 ± 17.1 months. The weighted average clinical success rate, including wound healing and improved symptomatology, was 69.9% (range = 19%–100%). The limb salvage rate was 93.1% in the Tomoi et al study at 12 months follow-up 7 and 100% in the Ruzsa et al study at 36.9 months follow-up. 9 Cheun et al provided the longest follow-up outcomes data with primary patency, assisted primary patency, secondary patency, limb salvage, amputation-free survival, and freedom from major adverse limb events (MALEs) rates at 38%, 46%, 54%, 45%, 48%, and 45% at 5 years, respectively. 13
Predictors of Technical and Clinical Success
Three studies described predictors of hand/wound healing, clinical success, cumulative patency, amputation-free survival, and freedom from MALEs, and they are summarized in Table 3.4,7,13
Outcomes and Predictors.
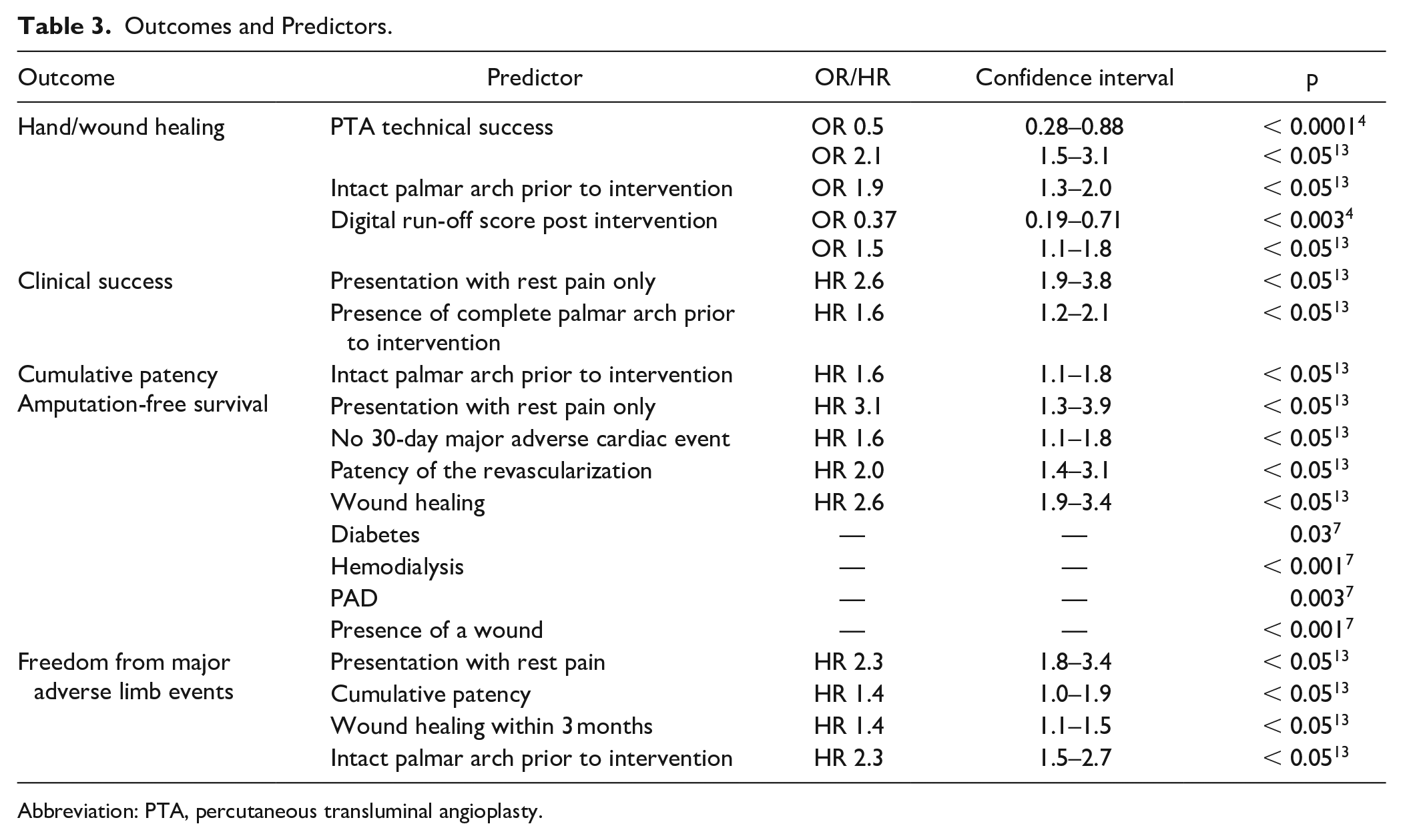
Abbreviation: PTA, percutaneous transluminal angioplasty.
Complications and Mortality
Complications and limb loss data are presented in Table 4. Short-term complications (< 30 days) (4.7%) included access site hematomas (10/19), pseudoaneurysms (3/19), flow-limiting dissections (2/19), radial artery perforation or re-thrombosis (3/19), and contrast-induced nephropathy (1/19). The 30-day major adverse cardiac event and MALE rates reported by Cheun et al were 1 and 3%, respectively. 13 Although the Ruzsa et al study reported 42/101 cumulative major adverse event rate at 3 years, the data includes outcomes for both ATE and BTE revascularization. 9 Nearly 20% of patients required an amputation, and most (96%) were minor (either distal phalanges or digits). Only 2 patients required above-wrist amputations. 7 Mortality data are summarized in Table 4. The pooled mortality rates across studies at 14 months, 36 months, and 60 months were 20.5% (17/83), 25.5% (47/184), and 33.1% (78/236), respectively.
Complications, Limb Loss, and Mortality Data.
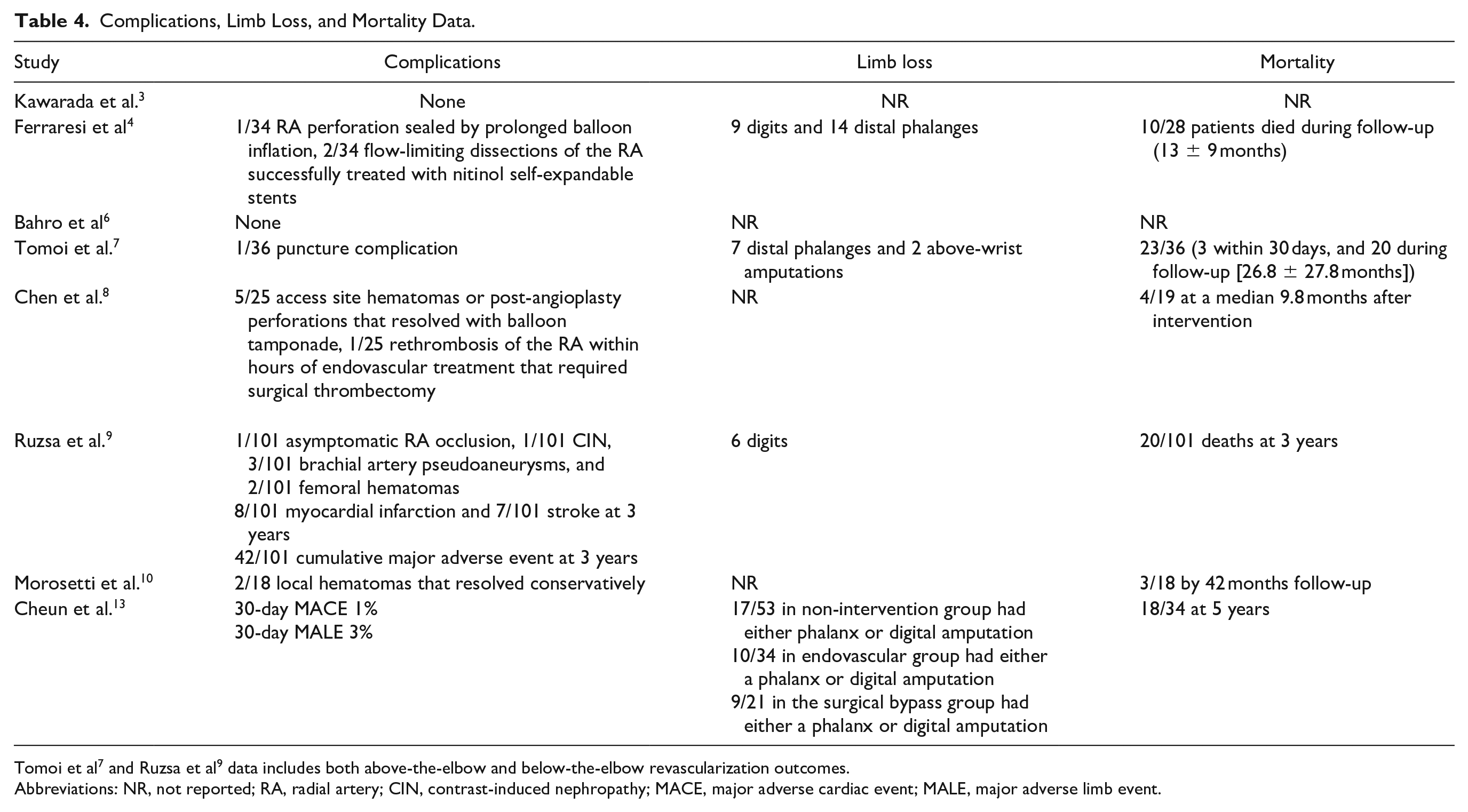
Tomoi et al 7 and Ruzsa et al 9 data includes both above-the-elbow and below-the-elbow revascularization outcomes.
Abbreviations: NR, not reported; RA, radial artery; CIN, contrast-induced nephropathy; MACE, major adverse cardiac event; MALE, major adverse limb event.
Conservative Management, Endovascular Management or Surgical Bypass
Cheun et al examined the outcomes of patients presenting with CHI due to BTE obstructive disease who underwent non-operative versus operative management (endovascular or surgical bypass). 13 Of 108 patients (average age = 59; 56% male), 34 underwent endovascular therapy with a median 1.5 vessels (UA, RA and/or IA) treated, 21 underwent a saphenous vein bypass to either the RA (12) and/or ulnar artery (11), and 53 were managed conservatively.
At baseline, there was a higher proportion of patients with diabetes in the endovascular and surgical bypass groups compared with the no intervention group (94% and 81% vs 72%, p = 0.03). The remaining demographics and comorbidities were similar. There was also a higher number of patients with intact palmar arch anatomy in the endovascular and bypass groups (52% and 68%, vs 12%, p = 0.001).
At follow-up, there was a significantly higher percentage of patients who had improved finger-brachial index (55% and 85% vs 11%, p = 0.002), wound healing rate (83% and 95% vs 69%, p = 0.002), and 3-month symptom relief (75% and 82% vs 7%, p = 0.002) in the endovascular and surgical bypass groups compared with the conservative management group. Although the clinical efficacy (47% and 59% vs 33%, p = 0.12) and limb salvage rates (45% and 55% vs 37%) were higher in the operative management group, they did not reach statistical significance.
There was no significant difference in overall morbidity, 30-day objective performance goals, or 90-day mortality rates between all groups. There was also no significant difference in overall amputation rate (either a phalanx or a digit) between all groups: 17/53 (32%) in the conservative management group, 10/34 (29%) in the endovascular treatment group, and 9/21 (43%) in the surgical bypass group.
The amputation-free survival and overall survival rates at 5 years were significantly higher in the endovascular and bypass groups compared with the conservative management group (48% and 65% vs 35%, p = 0.04 for AFS; 48% and 65% vs 33%, p = 0.04 for OS).
The primary, assisted primary, and secondary patency rates at 5 years trended toward the bypass group compared with the endovascular group, however this did not reach statistical significance (38% vs 54%, 46% vs 64%, and 54% vs 69%). Bypass grafting was a predictor for cumulative patency (HR = 2.2, 95% CI = 1.9%–3.4%). The endovascular group had a statistically significant lower rate of MALEs compared with the bypass group (45% vs 64%, p = 0.02).
Discussion
CHI due to BTE obstructive arterial disease is an emerging and debilitating problem particularly for patients with diabetes and chronic kidney disease. 4 The true prevalence is difficult to assess because most patients are managed conservatively.4,5,13 The broader collateral networks in the arm and reduced relative strain of the upper extremity muscle mass compared with the lower limbs, are thought to provide compensatory response to stenotic lesions and delay the onset of symptoms.3,10,17 Quality of life preservation requires early identification of CHI patients to minimize tissue loss and preserve hand function.
The understanding of the pathophysiology in BTE obstructive arterial disease is evolving, but parallels have been drawn from the below-the-knee (BTK) arterial literature. It is likely BTE obstructive arterial disease is a combination of medial calcification (Mönckeberg’s sclerosis) and to a lesser degree atherosclerosis that results in luminal stenosis.18,19 In a histopathological study of 239 lower extremity arteries collected from patients who underwent amputation due to critical limb ischemia, atherosclerosis was more frequent in the femoral and popliteal arteries compared to the infrapopliteal arteries. 20 Diabetes and chronic kidney disease are risk factors for increased medial calcification, 19 and therefore, it is not surprising that these patients are the ones that suffer the most from extensive BTE occlusive disease. Furthermore, in patients with type 2 diabetes, medial calcification was associated with a 4-fold increased risk for lower extremity amputation. 21 Further understanding of the underlying pathophysiology leading to BTE occlusive disease is necessary to adequately identify patients and manage their disease.
Pre-existing ipsilateral AV fistula and history of prior endovascular intervention via radial access (eg, coronary angiogram/revascularization) are also considerations in this population. However, the incidence of symptomatic steal syndrome is low, occurring in 4%–10% of patients undergoing vascular access for hemodialysis.22-25 AV fistula management may also fail to improve digital blood flow in patients with diffuse BTE vascular disease. 26 Conversely, treating a stenotic non-AVF related artery can reduce or resolve hand ischemia while sparing the AVF for dialysis (eg, PTA of ulnar artery stenosis in a patient with radiocephalic AVF). 4 In this systematic review, only 12.5% of patients were reported to have an active ipsilateral AV fistula. Vascular complications following transradial access, particularly for coronary angiography and percutaneous coronary intervention, are summarized elsewhere. 27 None of the included studies in this systematic review reported on history of previous transradial access.
Similar to BTK revascularization, the goal of endovascular treatment of BTE vessel disease is to establish inline flow to the palmar arch, preferably via both radial artery and ulnar artery supply. In the studies included in this review, 0.014- and 0.018-in guidewires were essential to cross vascular lesions, including CTOs, with low-profile balloons for angioplasty using an anterograde brachial access and 4- or 5-Fr vascular sheaths. Low-profile balloons can be particularly helpful for more distal lesions; they can also reduce access site hemostasis complications and minimize patient discomfort for those with advanced ischemic hand symptoms. 3 If antegrade recanalization fails, other options include dual access (for example, femoral artery/radial artery or radial artery/palmar arch), 9 retrograde access using transradial-transbrachial approach, 10 subintimal recanalization,8,9 or the palmar arch loop technique. 10 The latter is akin to the pedal plantar loop technique for BTK revascularization. 28 Atherectomy has been described for BTE arterial occlusive disease, but due to limited available evidence to date, no definitive conclusions can be drawn. 6
There was a high technical success rate across all studies ranging from 82% to 100% (weighted average was 89.3%), demonstrating that PTA is feasible and can reliably establish inline flow to the palmar arch. The restenosis rate varied from 18% to 44% at 6–48 months follow-up in 4 studies.4,9,10,13 Primary patency, assisted primary patency, and secondary patency rates were reasonable at 38%, 46%, and 54% at 5 years, respectively. 13 Cheun et al showed that an intact palmar arch prior to intervention was predictive of cumulative patency. 13 Use of drug-eluting balloons and stents was rare for primary revascularization in the included studies, and as such, no meaningful conclusions can be made with respect to their efficacy in managing BTE vessel disease.
The definition of clinical success varied across studies, as well as the follow-up algorithm and measured secondary outcomes. For example, Kawarada et al defined clinical success as resolution of resting pain or improvement in an ulcer or gangrene. 3 Comparatively, Ruzsa et al defined clinical success as an improvement of at least one clinical category in the Rutherford-Becker classification. 9 Therefore, while the average rate for clinical success was effective at 69.9%, the lack of a standardized definition limits the generalizability of this statistic. Analysis of the Ruzsa et al study is also somewhat limited by the variable etiology of chronic CHI.
Three studies described predictors of hand/wound healing, clinical success, cumulative patency, amputation-free survival, and freedom from MALEs, as summarized on Table 3. In both the Ferraresi et al and Cheun et al studies, digital run-off post revascularization was predictive of hand/wound healing.4,13 Building on this concept, the Ferraresi et al study described a useful quantitative tool, the modified digital obstruction index, which is predictive of clinical success of revascularization. This modified digital obstruction index is based on giving one point for each patent digital artery in the final angiogram, for a maximum of 9 points. The premise behind this tool is that obstructive disease within the digital vessels will ultimately reduce hand-healing even if successful PTA of inflow lesions was established. In the Cheun et al study, the status of the palmar arch prior to intervention was also predictive of wound healing, clinical success, cumulative patency, and freedom from MALE. 13
PTA of BTE vessels is safe. Two studies reported no complications, and the remaining studies reported predominately minor complications pertaining to access site hematoma or pseudoaneurysm. One study reported a case of rethrombosis of the radial artery shortly following revascularization, which required surgical thrombectomy. However, this was due to inappropriate postprocedure heparin dosing.
Cheun et al was the only comparative study that examined the outcomes of BTE CHI patients who underwent conservative management, endovascular treatment, or surgical bypass. 13 There were significantly higher rates of improved finger-brachial index, wound healing, and 3-month symptom relief among patients who had operative management (either endovascular or surgical bypass) versus conservative therapy. The overall survival and AFS rates were also significantly higher. However, it is important to note these findings may be confounded by the statistically significant higher proportion of patients in the operative groups with intact palmar arch anatomy prior to the interventions. Interestingly, there was no significant difference in the amputation rate (either a phalanx or digit) between all management groups: 17/53 (32%) in the non-operative group, 10/34 (29%) in the endovascular group, and 9/21 (43%) in the surgical bypass group. While this may seem to contradict the aforementioned benefits of PTA revascularization or surgical bypass compared to non-operative management, this finding instead reinforces the need for early identification of CHI patients, particularly with diffuse BTE vessel disease, to establish inflow to the palmar arch and digital vessels, and thereby improve wound healing and reducing the amputation rate. More comparative studies are necessary to elucidate the long-term benefit of endovascular PTA compared to surgical bypass and conservative management.
The limitations of this systematic review include inherent biases of retrospective, nonrandomized, observational studies, utilizing Embase and MEDLINE only for the literature search, small population size, clinical success definition heterogeneity, differences in wound care regimens and follow-up criteria at each institution, and limited data on the use of drug-coated balloons and stenting.
Conclusion
Critical hand ischemia due to below-the-elbow obstructive arterial disease is a devastating condition, and may result in amputation. There is currently no consensus on the revascularization strategy for these patients, and most are managed conservatively. Early identification is necessary to preserve hand function. PTA of BTE vessels is feasible with high technical success. Further comparative studies are necessary to establish the long-term clinical benefits of PTA revascularization compared to non-operative management and surgical bypass.
Supplemental Material
sj-docx-1-jet-10.1177_15266028211050309 – Supplemental material for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review
Supplemental material, sj-docx-1-jet-10.1177_15266028211050309 for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review by Ghassan Awad El-Karim, Sean A. Kennedy, Roberto Ferraresi, Jamil A.K. Addas, George D. Oreopoulos, Arash Jaberi, Kong Teng Tan and Sebastian Mafeld in Journal of Endovascular Therapy
Supplemental Material
sj-docx-2-jet-10.1177_15266028211050309 – Supplemental material for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review
Supplemental material, sj-docx-2-jet-10.1177_15266028211050309 for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review by Ghassan Awad El-Karim, Sean A. Kennedy, Roberto Ferraresi, Jamil A.K. Addas, George D. Oreopoulos, Arash Jaberi, Kong Teng Tan and Sebastian Mafeld in Journal of Endovascular Therapy
Supplemental Material
sj-docx-3-jet-10.1177_15266028211050309 – Supplemental material for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review
Supplemental material, sj-docx-3-jet-10.1177_15266028211050309 for Percutaneous Transluminal Angioplasty for Below-the-Elbow Critical Hand Ischemia: A Systematic Review by Ghassan Awad El-Karim, Sean A. Kennedy, Roberto Ferraresi, Jamil A.K. Addas, George D. Oreopoulos, Arash Jaberi, Kong Teng Tan and Sebastian Mafeld in Journal of Endovascular Therapy
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.