
Abstract
Purpose
To assess the incidence of migration after endovascular aneurysm sealing (EVAS) in conjunction with chimney grafts (chEVAS) for repair of abdominal aortic aneurysms (AAAs).
Materials and Methods
A retrospective, observational cohort study was conducted of 31 patients (mean age 75.7 years; 27 men) treated for juxtarenal AAA between April 2013 and December 2018 at single centers in New Zealand and the Netherlands. The majority of patients received >1 chimney graft (13 single, 13 double, and 5 triple) during chEVAS. Six patients had only the first postoperative scan, so the migration analysis was based on 25 patients.
Results
Median seal length assessed on the first postoperative computed tomography scan was 36.5 mm. The assisted technical success rate was 93.5% with 2 technical failures. Median time to final imaging follow-up was 17 months in 25 patients. At the latest follow-up, there were no cases of caudal migration >10 mm. Freedom from caudal movement of 5 to 9 mm was estimated as 86.1% at 1 year and 73.9% at 2 years; freedom from clinically relevant migration (movement requiring reintervention) was 100% at both time intervals. However, at 3 years there were 2 cases of caudal movement of 5 to 9 mm and a type Ia endoleak warranting reintervention. No correlation between migration and aneurysm growth (p=0.851), endoleak (p=0.562), or the number of chimney grafts (p=0.728) was found. During follow-up, 2 patients (7%) had aneurysm rupture and 10 (33%) had reinterventions. Eight patients (27%) died; 2 were aneurysm-related (7%) and due to the consequences of a reintervention.
Conclusion
In the 2 years following chEVAS, there was no caudal migration >10 mm, but nearly a quarter of patients had caudal movement of 5 to 9 mm. A trend was observed toward ongoing migration that required intervention at 3-year follow-up. chEVAS is technically challenging and should be considered only for patients with no viable alternative treatment option.
Keywords
Introduction
Endovascular aneurysm repair (EVAR) has supplanted open repair as the most common treatment option for abdominal aortic aneurysm (AAA) due to reduced early morbidity and mortality.1–4 However, EVAR is associated with long-term modes of failure not seen with open repair, resulting in higher reintervention rates.5,6 Since the introduction of EVAR, endograft designs and delivery systems have evolved to respond to these complications and to increase anatomical applicability of the devices. 7
Endovascular aneurysm sealing (EVAS) was commercially introduced in 2013 and is based on the principle of “active sac management” through the use of dual endobags mounted on balloon-expandable endoframes. The Nellix EVAS System (Endologix, Irvine, CA, USA) was designed to achieve complete aneurysm sac exclusion, with the expectation of a low endoleak rate, particularly type II. Initial results of EVAS were positive for the most part,8,9 but the occurrence of migration after EVAS was a particular problem, with an incidence ranging between 2% and 17%10–12 based on diverse definitions of migration. Various factors may contribute to migration, including patient anatomy and suboptimal positioning of the device. 13 Anatomical features predisposing to migration include hostile infrarenal neck anatomy and a small blood volume within the aneurysm sac, which causes incomplete polymer filling of the endobags, reducing endoframe support and lessening resistance to lateral bending and subsequent migration forces. 14
Hostile infrarenal neck refers to short, wide, conical, or severely angulated necks and those with significant thrombus and/or calcification. 8 Common endovascular management options for patients with a hostile infrarenal neck include fenestrated EVAR (fEVAR), chimney EVAR (chEVAR), and chimney EVAS (chEVAS). Theoretically, chEVAS should be better than chEVAR because the compliant endobags fill the space between the Nellix stents and the chimney grafts, reducing the incidence of gutter type Ia endoleak. This advantage of chEVAS has been confirmed in bench models15,16 and subsequently reported in clinical practice, most notably in the ASCEND Registry. 17
Logically, migration after chEVAS might occur less frequently and to a lesser degree compared to standard EVAS for several reasons. First, the device is sealing into a healthier aortic segment, usually a neck below the superior mesenteric artery (SMA) or celiac trunk. An adequate neck length of at least 20 mm can be achieved using this technique of moving the landing zone up the aorta. Second, the infrarenal EVAS device also achieves fixation by filling the blood lumen within the aneurysm sac and the proximal and distal sealing zones without the assistance of hooks or barbs. Third, the proximal endobag shelf in chEVAS has considerably less cross-sectional area compared to conventional infrarenal EVAS due to the space occupied by the chimney grafts. This could reduce the downward displacement force on the implant.
The current study investigates the incidence of migration and endoleak when the Nellix System is used in conjunction with chimney grafts to determine if the migration is less frequent with the chEVAS configuration than the infrarenal EVAS device.
Materials and Methods
Study Design and Patient Sample
A retrospective, observational study was conducted of chEVAS patients treated electively for asymptomatic AAAs at 2 active and experienced EVAS centers in New Zealand and the Netherlands between April 2013 and December 2018. Both research sites acquired local ethics committee approval according to national guidelines (New Zealand: HDEC 19/CEN/6; the Netherlands: LHC 2018-1316). The study was conducted according to the principles of the Declaration of Helsinki and in accordance with the applicable guidelines, regulations, and acts. Patients gave informed consent for the procedure and the use of anonymized data in research.
Patients were considered for chEVAS if they were deemed unfit for open surgical repair and for fEVAR. Of 52 chEVAS cases performed during the study period, 16 patients were excluded because the procedure was performed as a reintervention for EVAS, EVAR, or open repair (n=2). Additionally, 2 patients could not be contacted to provide consent, 2 patients were treated for symptomatic intact or ruptured AAA, and 1 patient received the chimney grafts in the internal iliac artery and none proximally. These exclusions left 31 patients (mean age 75.7 years; 27 men) for analysis of migration and endoleak. The majority (n=25) of patients were from the New Zealand center. Baseline clinical and anatomical characteristics are presented in Table 1. The comorbidity profile was typical of an AAA cohort. All aneurysms were juxtarenal and 30 were fusiform. Eight (27%) patients had a maximum sac to lumen diameter ratio >1.40.
Baseline Clinical and Anatomical Characteristics of the 31 Patients in the Study. a
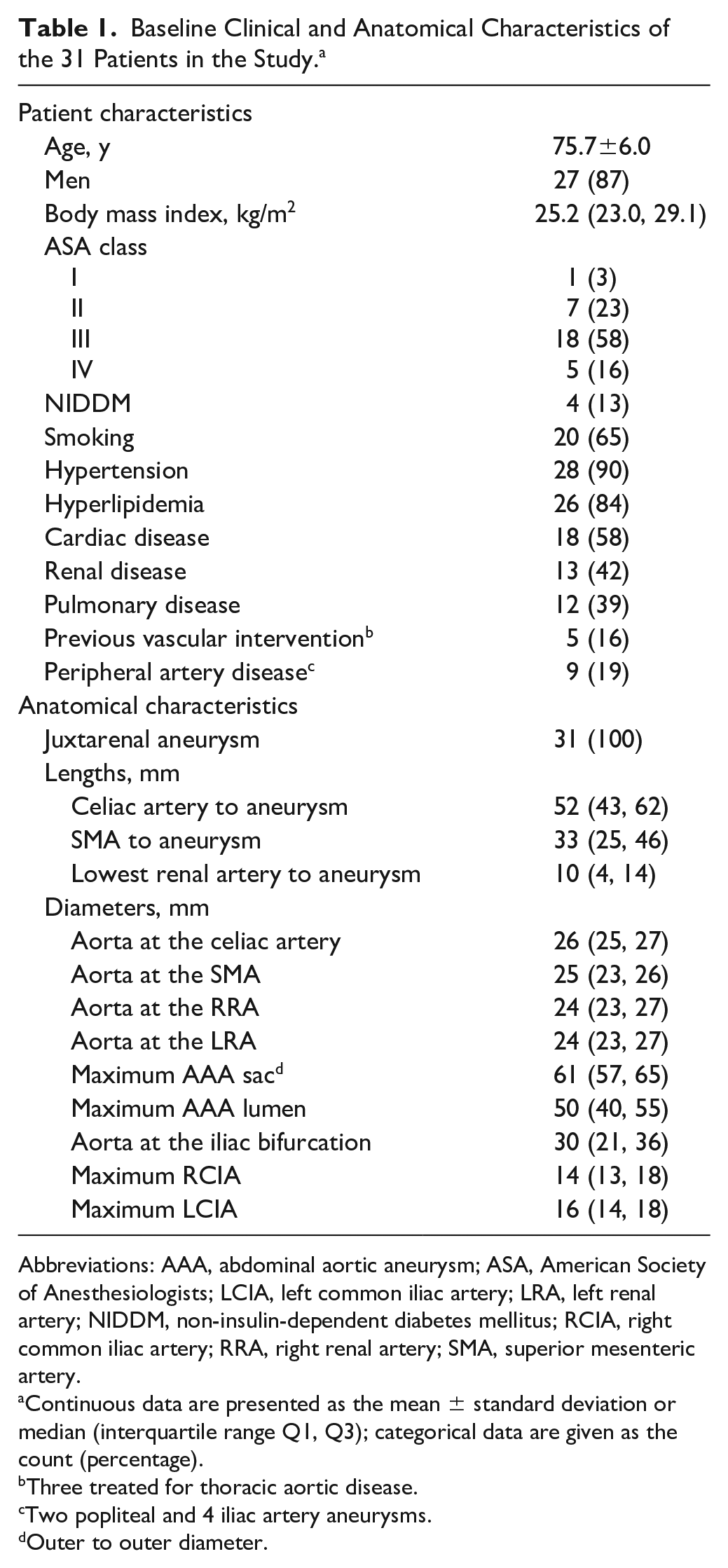
Abbreviations: AAA, abdominal aortic aneurysm; ASA, American Society of Anesthesiologists; LCIA, left common iliac artery; LRA, left renal artery; NIDDM, non-insulin-dependent diabetes mellitus; RCIA, right common iliac artery; RRA, right renal artery; SMA, superior mesenteric artery.
Continuous data are presented as the mean ± standard deviation or median (interquartile range Q1, Q3); categorical data are given as the count (percentage).
Three treated for thoracic aortic disease.
Two popliteal and 4 iliac artery aneurysms.
Outer to outer diameter.
Procedure
The conventional EVAS procedure 18 as well the chEVAS technique 17 have been described previously. For chEVAS, percutaneous or open access was achieved through the femoral arteries for introduction of the Nellix devices, while the chimney grafts were introduced via brachial, axillary, or subclavian artery accesses. Depending on the aneurysm morphology, chimney grafts [typically Advanta V12 (Getinge, Gothenburg, Sweden) and Viabahn (W. L. Gore & Associates Inc, Flagstaff, AZ, USA)] were placed in the renal arteries, SMA, and/or the celiac trunk. Once the Nellix stents and chimney grafts were in position, the Nellix stents were usually deployed first, which facilitated a more parallel course for the chimney grafts during their subsequent deployment. The endobags were pre-filled with saline to verify the calculated volume for the polymer fill, while the delivery balloons were kept inflated in all chimney grafts and Nellix systems. Polymer fill was performed to a pressure of at least 180 mm Hg after aspiration of the prefill. Angiography was performed to confirm aneurysm seal; if necessary, a secondary fill of the endobags was performed.
Aneurysm Morphology and Device Migration
Preoperative and follow-up computed tomography angiography (CTA) scans collected at 1, 6, and 12 months and annually thereafter were assessed for this analysis by an independent radiologist (A.S.) and independently reviewed (A.Ho.) with the use of 3-dimensional vascular planning software (Syngo.via; Siemens, Erlangen, Germany). Diameters at the level of the celiac artery, SMA, right and left renal arteries, maximum aneurysm, and left and right common iliac arteries were measured perpendicular to the center lumen line from the outer-to-outer walls and directly caudal to the specified vessel. The maximum aneurysm diameter and maximum aortic flow lumen diameter were used to calculate the aortic diameter ratio. The caudal extent of the aneurysm neck was where the aortic diameter was increased >20% compared with the aortic diameter at the level of the lowest renal artery. Aneurysm neck lengths were measured from the caudal orifice of the celiac trunk, the SMA, and the lowest renal artery to the caudal end of the aneurysm neck. All visceral arteries were checked for stenosis and occlusion.
Seal length was determined as the distance between the top end of the highest Nellix stent-graft and the beginning of the aneurysm on the first postoperative CT. The top 5 mm of the Nellix stent-graft is not covered by endobag, however, for uniformity of measurements. this was included in the seal zone length.
Follow-up imaging recorded the Nellix graft position relative to the caudal orifice of the SMA, with positive values being above the SMA and negative values being below the SMA. Any fracture of the Nellix endoframes or complication of the chimney grafts was reported, including occlusion, stent fracture, evident position change, and compression.
Migration was assessed by comparing the first postoperative CTA to the latest available follow-up imaging. When a CTA at a follow-up window was absent but a CTA on a later follow-up showed no migration, it was assumed there was no migration in the interim. Clinically relevant migration after EVAR is reported as caudal migration ≥10 mm or caudal movement of 5 to 9 mm with the need for reintervention.
Definitions
Comorbidities were scored according to the Society of Vascular Surgery comorbidity grading scale. 19 Hypertension was defined as known history of hypertension or use of antihypertensive medication. Hyperlipidemia was defined as known history or the use of a statin or elevated lipid levels (low-density lipoprotein, total cholesterol, and triglyceride levels above normal limits for age). Renal insufficiency was based on a serum creatinine ≥2.4 mg/dL or dialysis dependency. Smoking included current and prior smoking in the past 10 years. 19 An aneurysm was considered juxtarenal when the infrarenal neck length was <10 mm or when the neck length was 10 to 15 mm but with hostile features (infrarenal diameter >28 mm, infrarenal neck angle >60°, circumferential calcium, or circumferential thrombus).
Technical success was defined as successful introduction and deployment of the device without open conversion, death, type I or III endoleak, or graft limb occlusion within 24 hours after the procedure. The term “assisted technical success” was applied to cases in which unplanned endovascular or surgical procedures were required to successfully exclude the aneurysm during the index chEVAS procedure. 20
Endoleaks were defined according to the Society for Vascular Surgery reporting standards of vascular surgery, 19 and type Ia endoleaks were defined as specified by van den Ham et al. 21 Type 1S1 endoleak is the appearance of contrast between the endobag and the wall of the proximal neck but not reaching the aneurysm sac itself. In a type 1S2 endoleak, the contrast reaches the aneurysm wall and extends into the aneurysm sac. A type 1S3 endoleak refers to contrast between the endobags inside the aneurysm sac.
Mortality was reported as all-cause mortality and as aneurysm-related mortality at 6 months, 1 year, and 2 years. Aneurysm-related mortality included death due to aneurysm rupture or the consequence of a primary or secondary procedure or surgical conversion.
Statistical Analysis
Continuous variables were presented as mean and standard deviation or as median and interquartile range (IQR Q1, Q3) depending on the distribution of data based on Kolmogorov-Smirnov tests and histograms. Categorical variables were presented as counts (percentages). Correlations between migration and aneurysm growth, endoleak, the number of chimney grafts, and the aortic diameter ratio were explored using a 2-sided Pearson chi-square test. The threshold of statistical significance was p<0.05. Kaplan-Meier survival analysis was performed with censoring for patients lost to follow-up. All statistical analyses were performed using IBM SPSS Statistics (version 24.0; IBM Corporation, Armonk, NY, USA).
Results
Procedure Details
All patients had the procedure under general anesthesia, and the majority had bilateral percutaneous accesses (22, 71%). The Advanta V12 was used in 71% of the chimneys, the Viabahn in 19%, and other stents in 10%. Nine of the 13 single chimney procedures (11 left and 2 right renal arteries) were performed before 2016. Eleven of the 13 double chimneys were in the renal arteries. Additionally, 1 patient received a stent in the SMA and right renal artery, and 1 patient had stenting of 2 right renal arteries. Of the 5 triple chimneys, 1 had stents in an accessory renal artery and both main renal arteries; the other 4 patients had chimneys to both renal arteries and the SMA. The median polymer fill volume was 109 mL (IQR 75, 132) at a median pressure of 220 mm Hg (IQR 210, 240). There were 10 secondary fills with a median volume of 10 mL (IQR 8, 14). Additionally, median seal length analyzed on the first postoperative CTA was 36.5 mm (IQR 30.3, 51.3).
Primary technical success was achieved in 20 of 31 patients (64%). Another 9 cases required additional unplanned procedures to successfully seal the aneurysm (93% assisted technical success). Four iliac stents were placed for acute angulation, distal endoleak, stenosis, and inadequate distal seal; additional renal stenting for inadequate stent length or dislocation was done in 3. One patient needed an SMA stent because the origin was compromised by the renal artery chimneys. Finally, 1 patient required additional stent placement in the renal artery because of migration and relining of the chimney for common iliac artery rupture after postdilation. Other details of the procedures are given in Table 2.
Details of the 31 Procedures. a
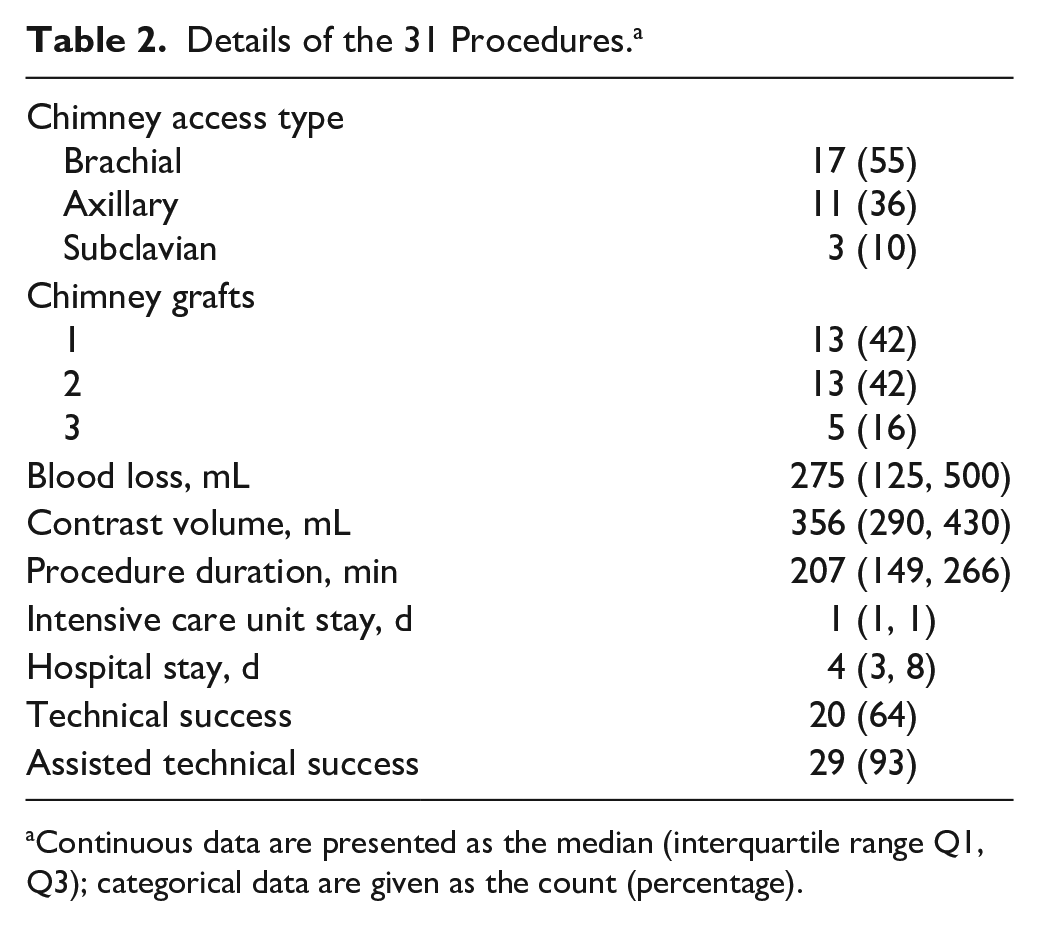
Continuous data are presented as the median (interquartile range Q1, Q3); categorical data are given as the count (percentage).
Of the 2 failures, 1 was due to a small postoperative type Ib endoleak. The second case required conversion to remove the Nellix system because the nosecone could not be retrieved by endovascular means.
Overall Complications
Aneurysm-related complications are reported in Table 3. Of 10 reinterventions (33%) required after the index procedure, 2 were for aneurysm rupture. The first had ongoing sac expansion during follow-up and had a rupture at 3 months. The patient was treated with a Nellix-in-Nellix procedure, 22 with a small type Ia endoleak persisting postoperatively. Five days later the patient died, possibly due to cardiac arrest. The second patient had a type Ib endoleak with contained rupture at 8 months, which was treated with open conversion. This was complicated by an acute on chronic kidney insufficiency that resolved during hospitalization.
Aneurysm-Related Complications. a
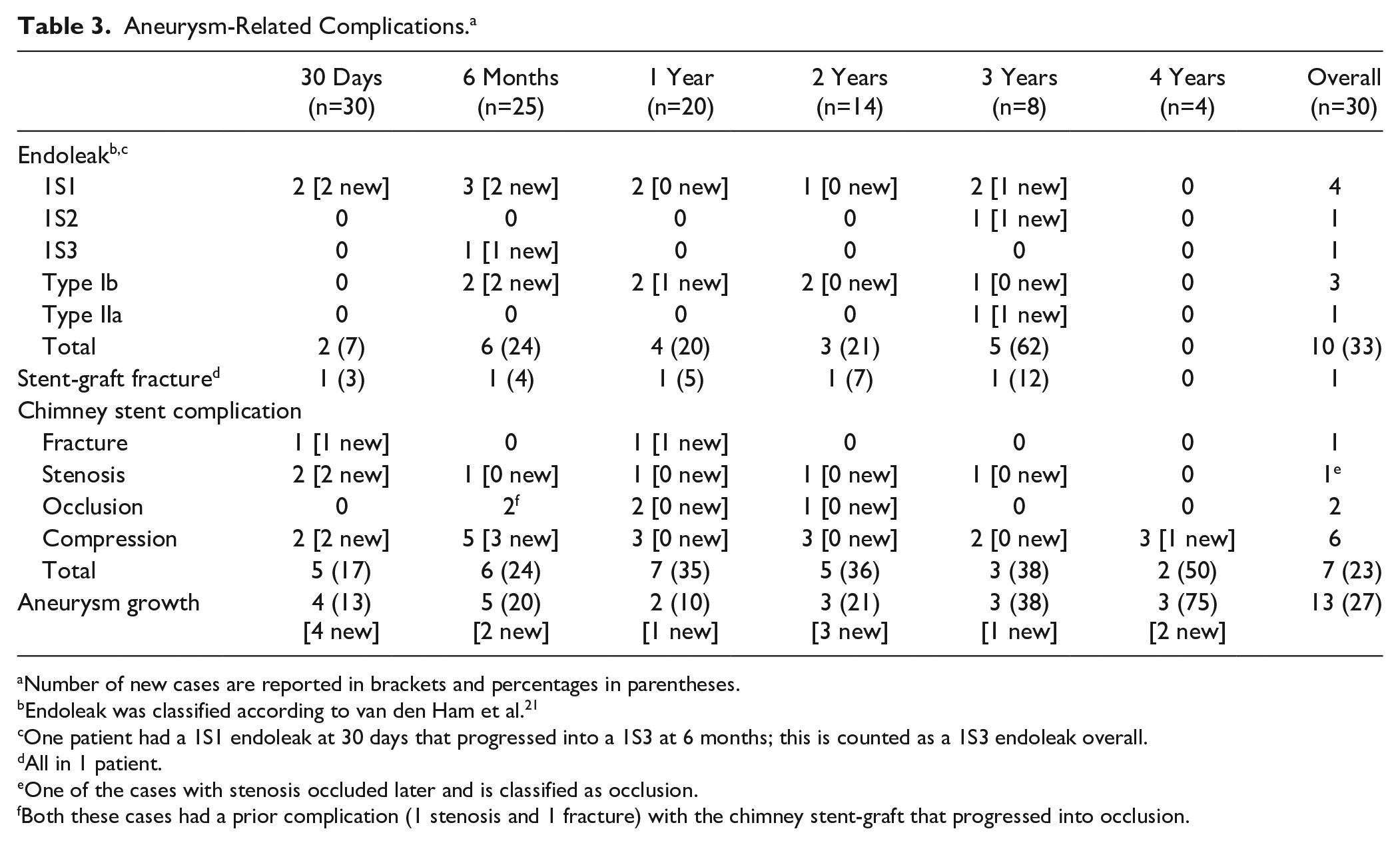
Number of new cases are reported in brackets and percentages in parentheses.
Endoleak was classified according to van den Ham et al. 21
One patient had a 1S1 endoleak at 30 days that progressed into a 1S3 at 6 months; this is counted as a 1S3 endoleak overall.
All in 1 patient.
One of the cases with stenosis occluded later and is classified as occlusion.
Both these cases had a prior complication (1 stenosis and 1 fracture) with the chimney stent-graft that progressed into occlusion.
Additionally, another patient had a Nellix-in-Nellix procedure for aneurysm growth. The other reinterventions were performed for 3 type Ib endoleaks and 2 renal stenoses (1 patient had 2 reinterventions, one for renal stenosis and the other later for a type Ib endoleak).
Of 8 patients (27%) who died in follow-up, 2 died at 6 months, 4 at 1 year, and 2 at 2 years. There were 2 aneurysm-related deaths as described above. The remaining causes of death were cancer (n=2), trauma (n=1), cardiac (n=1), stroke (n=1), and unknown (n=1).
Migration and Endoleak
Six patients (20%) had only the first postoperative scan, so evaluation of migration was based on 25 patients. The median time to the last follow-up CTA in these patients was 17 months (IQR 6, 35), and the median time to the last clinical follow-up visit was 23 months (IQR 10, 37).
There were no cases of caudal migration >10 mm throughout follow-up (Figure 1), but 7 of the 25 patients (28%) had caudal movement at 2 years (n=5) or beyond (n=2). The maximum observed caudal movement was 8 mm, which occurred at 3 years. Freedom from caudal movement of 5 to 9 mm (Figure 2) was estimated at 86.1% at 1 year and 73.9% at 2 years.
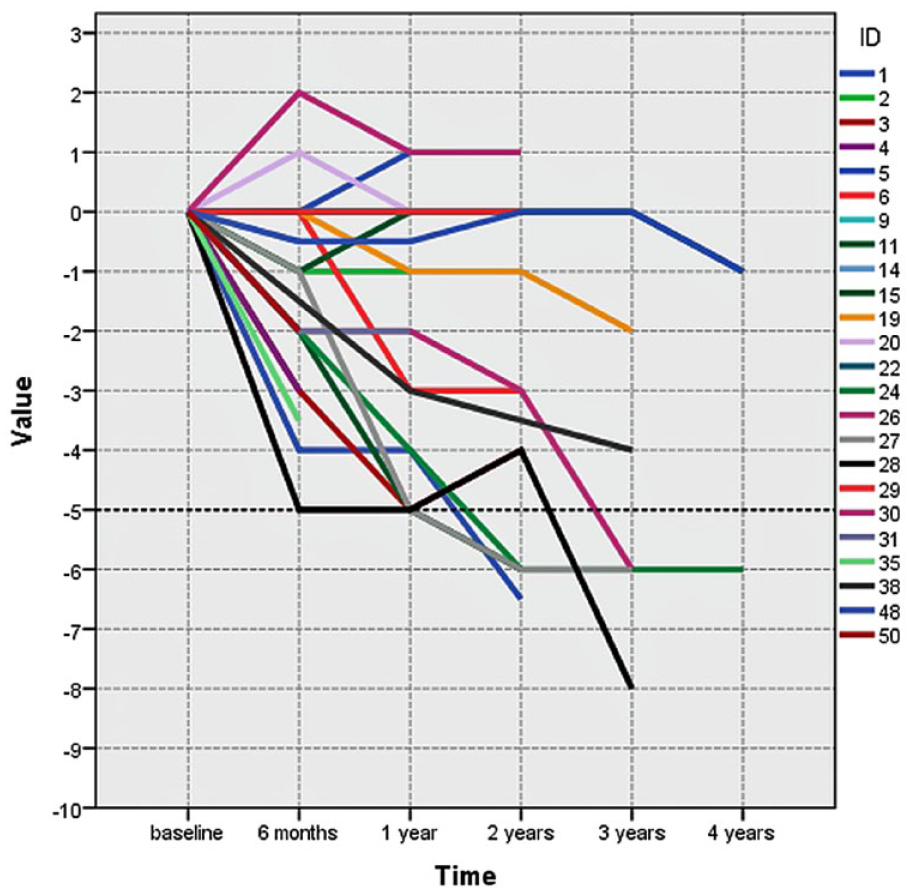
Plot of the maximum amount of migration of at least one of the Nellix stent-grafts over time. Each line represents 1 case. The dotted line indicates the cutoff point of significant (≥5 mm) caudal migration.
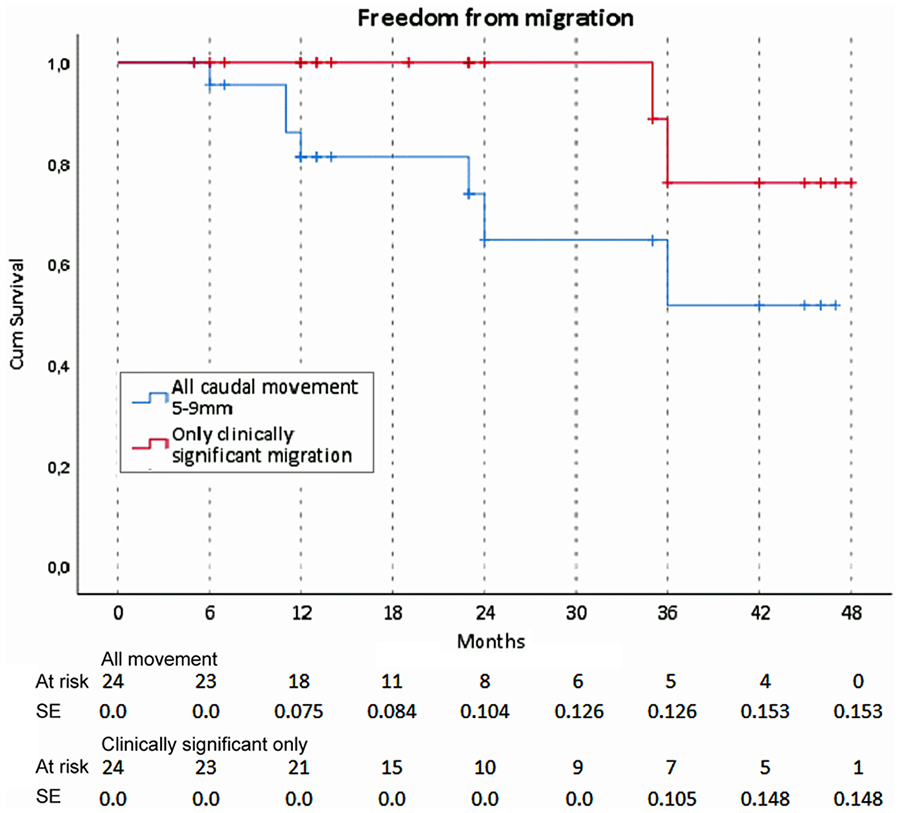
Freedom from caudal movement of 5 to 9 mm and freedom from clinically significant migration. The standard error exceeded 10% at 24 months for the 5- to 9-mm migration and 36 months for the clinically significant migration outcome.
Up to 2 years there was no clinically significant migration (caudal movement and a reintervention). At 3 years, however, 2 cases of caudal movement of 8 and 6 mm, respectively, and type Ia endoleak warranted reintervention. As such, the freedom from clinically significant migration was 76.2% at 3 years (Figure 2). One patient had migration with aneurysm growth and a type 1S1 endoleak. This patient underwent a Nellix-in-Nellix procedure with 3 vessel chimney after 4 years. The other patient had migration with aneurysm growth and a type 1S2 endoleak, which required conversion at 3.5 years. Unfortunately, the patient suffered a fatal stroke 7 days after the open procedure. Additionally, 1 patient with caudal movement of 5 to 9 mm from 1 year onward had sac shrinkage from 57 mm preoperatively to 47 mm at 1 year and 44 mm at 3 years. No other complications related to migration or endoleak were observed in the patients who had migration. There was no correlation between migration and aneurysm growth (p=0.851), endoleak (p=0.562), the number of chimney grafts (p=0.728), or the aortic diameter ratio and migration (p=0.402).
Discussion
Chimney EVAS has been a theoretically interesting alternative to other treatment options for patients with hostile neck anatomy, particularly if patients are not suitable for fEVAR, chEVAR, or open repair. Bench models and early clinical experience confirmed a low incidence of gutter type Ia endoleaks, potentially because the compliant endobags successfully fill the spaces between the Nellix stents and chimney grafts.16–18 In addition, it has been proposed that chEVAS may have better resistance to migration forces compared with conventional infrarenal EVAS. Factors that might contribute to reduced migration forces include friction force between the Nellix stents, chimney stents, and aortic wall; a healthier aortic sealing zone below the SMA; and a reduced proximal endobag shelf area due to the chimney stents.
A comparison with other studies is complicated by inconsistent definitions of migration. Stenson et al 23 recently published an analysis including 79 cases of chEVAS of which 57 were performed in an elective setting. They reported freedom from migration (≥5 mm) of 100% at 1 year and 85.7% at 2 years. Although they had a larger sample and more complex cases, our freedom from caudal movement (≥5 mm) was lower at both time points (86.1% at 1 year and 73.9% at 2 years). However, in both our study and Stenson’s, migration becomes problematic at or beyond 3 years’ follow-up.
The hypothesis of our study, that chEVAS might have lower rates of migration compared to EVAS, was not confirmed. The only cases of clinically significant migration occurred at 3 years, and both required reintervention for a type I endoleak. This 7% migration rate is comparable to migration after standard EVAS. The DEVASS registry 10 showed clinically significant migration of 7.1% at 2 years for EVAS cases treated within the instructions for use (IFU). The EVAS investigational device exemption trial 13 had a 6.0% migration >10 mm rate at 3 years. Of course, these rates are based on much larger patient samples than ours. Additionally, differences in aneurysm anatomy make a comparison between chEVAS and EVAS difficult, especially with the added consideration of a relatively challenging patient cohort.
Caudal migration may also occur due to hostile neck anatomy with a conventional endovascular approach, including fEVAR. England et al 24 reported an incidence of 21% caudal movement >4 mm after fEVAR, which is slightly lower compared to the 23% of caudal movement that was observed in the current study. However, all cases described in the current study were considered to have anatomies unsuitable for fEVAR. Unfortunately, no further information was available regarding the specific causes for unsuitability; the decision to perform chEVAS instead of alternative treatment in these cases was based on multiple factors and decided in a physician panel. Although chEVAS is also related to late migration, it might remain a last resort option for patients not fit for open repair and with anatomies not suitable for fEVAR.
Disturbingly, there were 2 patients who had aneurysm rupture after their Nellix procedure, of which one had a fatal outcome after endovascular reintervention. There was one other aneurysm-related death that occurred after open conversion for endoleak. These complications may have occurred due to the learning curve that is related to any new type of device but should not be taken lightly. It indicates the high risk associated with secondary intervention after EVAS and warrants ongoing surveillance.
It has been hypothesized that minimal caudal movement after EVAS may stabilize once the endobags are properly fixated. However, the data in this study indicate that once the stents move caudally, there is a trend toward progressing migration over time, as has been portrayed in Figure 1. A longer follow-up period and a larger number of patients would be needed to confirm this observation.
The low primary technical success rate shows the complexity of the chEVAS procedure, indicating it should be performed only by physicians with extensive experience in EVAS. Despite the capabilities and experience of the surgeons in our cohort, there were 2 technical failures, one of which led to conversion. This was due to a problem with the device design and resulted in changes to the design of the device. However, a good assisted technical success rate was achieved with additional steps during the index procedure, which suggests that chEVAS is technically challenging but feasible.
To achieve a good-quality seal zone for juxtarenal aneurysms and aneurysms with a hostile neck, the infra-SMA seal zone should be at least 20 mm. This generally involves stenting both renal arteries. However, there were a relatively large number of single chimneys in this study. The majority were in patients treated during the early experience with chEVAS, when a shorter seal zone length was accepted. Even though no correlation was observed between the number of chimney grafts and the occurrence of migration, it is advisable to perform at least a double chimney in order to achieve good seal. The high proportion of single chimneys may have negatively affected the results.
Limitations
It is crucial to acknowledge that this study had a small sample size with a limited follow-up. As such, the study could be underpowered, and results must be interpreted with caution. Stenson et al 23 showed high technical failure rates of chEVAS past 3 years, which was not available in our follow-up. The only 2 cases of clinically significant migration, our primary endpoint, occurred 3 years after the index procedure. Additionally, patients were selected for chEVAS if they were deemed unsuitable for open surgical repair or fEVAR, which produces a challenging cohort of patients. This selection bias must be taken into account. Despite these limitations, these midterm results give more insight into the benefits and drawbacks of chEVAS. Of note, the higher than anticipated midterm migration rate with EVAS prompted refinement of the Nellix IFU in 2016 and led to voluntary restriction of sales in 2019.
Conclusion
The incidence of clinically relevant migration after chEVAS is similar to that reported after EVAS performed inside the IFU at 2 years. Moreover, a trend was observed toward ongoing migration at 3 years that requires intervention. It is advisable to keep patients who underwent chEVAS under surveillance for such complications. Longer follow-up and a larger sample are indicated in order to draw more robust conclusions.
Footnotes
Authors’ Note
This study was presented at the 2019 Annual Veith Symposium (November 21, 2019; New York, NY, USA).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michel M. P. J. Reijnen and Andrew Holden are members of the Endologix scientific advisory board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.